Alkali: Examples include sodium hydroxide (lye), calcium hydroxide (lime, cement, plaster), and ammonia.
 Acids: sulfuric acid (battery fluid)
Acids: sulfuric acid (battery fluid)
 Mace (chloroacetophenone) and teargas
Mace (chloroacetophenone) and teargas
 Organic solvents
Organic solvents
 Detergents
Detergents
Symptoms
 Pain, redness, tearing, decreased vision
Pain, redness, tearing, decreased vision
Signs
 Mild to moderate
Mild to moderate
 Burns and edema of the eyelid
Burns and edema of the eyelid
 Conjunctival injection, chemosis, abrasion
Conjunctival injection, chemosis, abrasion
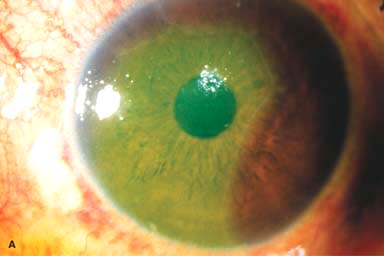
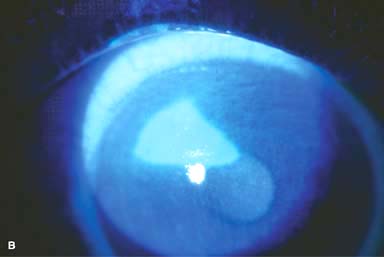
 Punctate or large epithelial defects on cornea (Fig. 11-1A)
Punctate or large epithelial defects on cornea (Fig. 11-1A)
 Mild anterior chamber activity
Mild anterior chamber activity
 Severe
Severe
 Severe burns of the skin of the eyelids
Severe burns of the skin of the eyelids
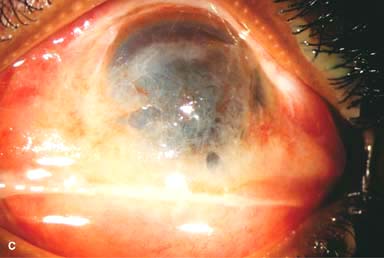
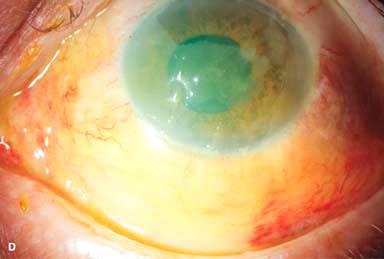
 Severe chemosis, conjunctival necrosis, conjunctival ischemia (sludging or absence of blood flow through conjunctival vessels) (Fig. 11-1B–E)
Severe chemosis, conjunctival necrosis, conjunctival ischemia (sludging or absence of blood flow through conjunctival vessels) (Fig. 11-1B–E)
 Scleral/limbal ischemia
Scleral/limbal ischemia
 Significant anterior chamber activity
Significant anterior chamber activity
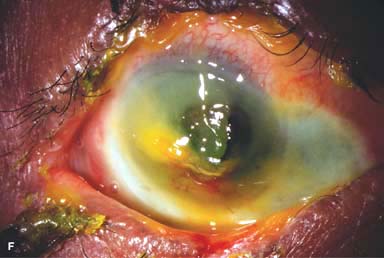
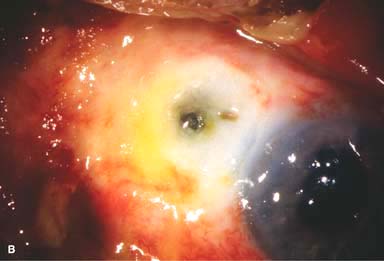
 Corneal epithelial defects, edema, or melting (Fig. 11-1F)
Corneal epithelial defects, edema, or melting (Fig. 11-1F)
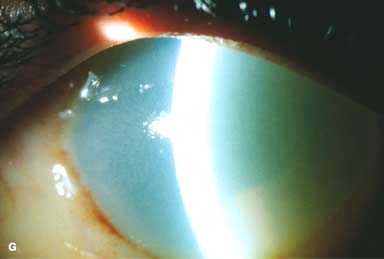
 Poor or no view of the anterior chamber because of corneal haze (Fig. 11-1G)
Poor or no view of the anterior chamber because of corneal haze (Fig. 11-1G)
 Intraocular pressure may be low, normal, or elevated in acute stages.
Intraocular pressure may be low, normal, or elevated in acute stages.
 The degree of limbal ischemia and corneal haziness carries prognostic importance.
The degree of limbal ischemia and corneal haziness carries prognostic importance.
Treatment
 Mild cases may be treated on an outpatient basis. Severe injuries may require hospitalization.
Mild cases may be treated on an outpatient basis. Severe injuries may require hospitalization.
 Copious irrigation with normal saline through an IV infusion set for at least 30 minutes and repeated every 30 minutes until neutral pH is reached.
Copious irrigation with normal saline through an IV infusion set for at least 30 minutes and repeated every 30 minutes until neutral pH is reached.
 Mechanical removal of foreign particles and debridement of necrotic tissues should be performed with a cotton-tipped applicator or jeweler’s forceps under topical anesthesia.
Mechanical removal of foreign particles and debridement of necrotic tissues should be performed with a cotton-tipped applicator or jeweler’s forceps under topical anesthesia.
 Frequent instillation of preservative-free tear drops (q1h)
Frequent instillation of preservative-free tear drops (q1h)
 Cycloplegics (e.g., scopolamine 0.25% or atropine 1% t.i.d.)
Cycloplegics (e.g., scopolamine 0.25% or atropine 1% t.i.d.)
 Topical antibiotic ointment (e.g., erythromycin, bacitracin, or tetracycline) q2h if an eye patch is not used. Pressure patching may aid in reepithelialization.
Topical antibiotic ointment (e.g., erythromycin, bacitracin, or tetracycline) q2h if an eye patch is not used. Pressure patching may aid in reepithelialization.
 Control intraocular pressure if it is elevated, either with topical drops or oral carbonic anhydrase inhibitors
Control intraocular pressure if it is elevated, either with topical drops or oral carbonic anhydrase inhibitors
 For injuries with significant inflammation and without risk of corneal melting, topical corticosteroid (e.g., dexamethasone 0.1% or prednisolone 1%) q1–2h may be used during the first week, tapered during the second week, and increased after epithelial healing if necessary. A combination antibiotic–corticosteroid (e.g., tobramycin 0.3%–dexamethasone 0.1% ointment) q1–2h can also be used.
For injuries with significant inflammation and without risk of corneal melting, topical corticosteroid (e.g., dexamethasone 0.1% or prednisolone 1%) q1–2h may be used during the first week, tapered during the second week, and increased after epithelial healing if necessary. A combination antibiotic–corticosteroid (e.g., tobramycin 0.3%–dexamethasone 0.1% ointment) q1–2h can also be used.
 Topical acetylcysteine 10% drops q.i.d. may help control collagenase activity and corneal melting.
Topical acetylcysteine 10% drops q.i.d. may help control collagenase activity and corneal melting.
 High-dose vitamin C 1 g PO t.i.d. and topical ascorbate 10% drops q1–6h may be helpful in severe alkali burns.
High-dose vitamin C 1 g PO t.i.d. and topical ascorbate 10% drops q1–6h may be helpful in severe alkali burns.
 Doxycycline 100 mg PO b.i.d. can be used to decrease collagenase activity.
Doxycycline 100 mg PO b.i.d. can be used to decrease collagenase activity.
 Early amniotic membrane graft or amniotic membrane on a scleral ring (e.g., Pro-Kera) may be beneficial in severe cases.
Early amniotic membrane graft or amniotic membrane on a scleral ring (e.g., Pro-Kera) may be beneficial in severe cases.
 If there is symblepharon formation, daily sweeping of the fornices with a cotton-tipped applicator or glass rod can be performed under topical anesthesia to break the adhesions. Alternatively, a scleral shell may be used.
If there is symblepharon formation, daily sweeping of the fornices with a cotton-tipped applicator or glass rod can be performed under topical anesthesia to break the adhesions. Alternatively, a scleral shell may be used.
 For progressive corneal melting or perforation, tissue adhesive, amniotic membrane graft, limbal stem cell graft, lamellar patch graft, or penetrating keratoplasty may be necessary.
For progressive corneal melting or perforation, tissue adhesive, amniotic membrane graft, limbal stem cell graft, lamellar patch graft, or penetrating keratoplasty may be necessary.
Complications
 Corneal haze or scarring
Corneal haze or scarring
 Infectious keratitis
Infectious keratitis
 Dry eyes
Dry eyes
 Symblepharon
Symblepharon
 Cicatricial entropion or ectropion
Cicatricial entropion or ectropion
 Trichiasis or distichiasis
Trichiasis or distichiasis
 Punctal stenosis or occlusion
Punctal stenosis or occlusion
 Limbal stem cell deficiency
Limbal stem cell deficiency
 Pannus formation
Pannus formation
 Cataract
Cataract
 Glaucoma
Glaucoma
Prognosis
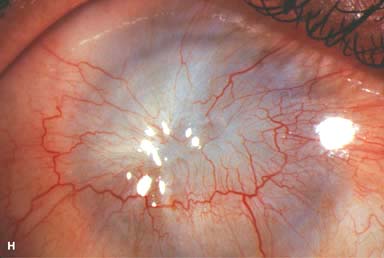
 Dismal to excellent, depending on the severity of the injury (Fig. 11-1H). In general, alkaline substances cause the most severe injuries, because they penetrate ocular tissues easily.
Dismal to excellent, depending on the severity of the injury (Fig. 11-1H). In general, alkaline substances cause the most severe injuries, because they penetrate ocular tissues easily.
Figure 11-1. Chemical burn. A. A mild acid injury caused a large corneal abrasion, which has been stained with yellow fluorescein dye. There is minimal to no conjunctival blanching, and the cornea is essentially clear. Mild chemical burns generally resolve without serious consequences. B. A sulfuric acid injury occurred to this patient’s right eye. There is a large central and inferior corneal epithelial defect and mild inferior conjunctival blanching. Chemical burn. C. This eye withstood a battery acid (sulfuric acid) injury. There is moderate conjunctival blanching and mucus adherent to the conjunctiva and cornea. D. The left eye of the patient seen in B has a much more extensive sulfuric acid injury. The epithelium is necrotic and has already sloughed off of the superior cornea. There is extensive conjunctival and scleral blanching inferiorly and nasally. Chemical burn. E. High-magnification view of the eye seen in D demonstrates ischemia of the conjunctiva and sclera. There is segmentation of the red blood cells, indicating lack of blood flow. The greater the degree of ischemia, the worse is the prognosis. F. A severe lye (sodium hydroxide) injury caused extensive ischemic damage in the lower two-thirds of the eye. The cornea has undergone necrosis centrally, leading to a perforation requiring an emergency corneal transplant. This alkali injury eventually resulted in enucleation. Chemical burn. G. Twelve days after a severe alkali injury, the conjunctiva and sclera remain blanched and the cornea is opaque. There has been no reepithelialization of the damaged cornea or conjunctiva. H. Many years after a severe chemical burn, the cornea remains totally scarred and vascularized.


THERMAL AND ELECTRICAL BURNS
THERMAL BURNS
Thermal burns can be mild to severe and can occur at any age. Cigarette burns are not uncommon in small children, whose eyes may be at hand level of a person holding a cigarette.
Etiology
 Curling irons
Curling irons
 Cigarettes, especially children
Cigarettes, especially children
 Flames
Flames
 Hot liquids
Hot liquids
 Molten metals
Molten metals
Symptoms
 Pain, redness, decreased vision
Pain, redness, decreased vision
Signs
 Thermal burns on skin of eyelids
Thermal burns on skin of eyelids
 Conjunctival injection, chemosis, epithelial defects
Conjunctival injection, chemosis, epithelial defects
 Punctate or large epithelial defects on cornea
Punctate or large epithelial defects on cornea
 A white area of cauterized epithelium (Fig. 11-2a)
A white area of cauterized epithelium (Fig. 11-2a)
 In severe cases
In severe cases
 Anterior chamber reaction
Anterior chamber reaction
 Corneal haze and edema
Corneal haze and edema
 Limbal or scleral ischemia, corneal or scleral perforation (Fig. 11-2b)
Limbal or scleral ischemia, corneal or scleral perforation (Fig. 11-2b)
Treatment
 Removal of foreign bodies and debridement of devitalized tissues
Removal of foreign bodies and debridement of devitalized tissues
 Topical antibiotic ointment to prevent infection and to lubricate the ocular surface (e.g., erythromycin, bacitracin, polymyxin B/bacitracin, ciprofloxacin q2–6h)
Topical antibiotic ointment to prevent infection and to lubricate the ocular surface (e.g., erythromycin, bacitracin, polymyxin B/bacitracin, ciprofloxacin q2–6h)
 Cycloplegics (e.g., cyclopentolate 1% or scopolamine 0.25% t.i.d.)
Cycloplegics (e.g., cyclopentolate 1% or scopolamine 0.25% t.i.d.)
 Pressure patching, lateral tarsorrhaphy, or amniotic membrane graft should be considered for large or nonhealing epithelial defects.
Pressure patching, lateral tarsorrhaphy, or amniotic membrane graft should be considered for large or nonhealing epithelial defects.
 Topical corticosteroids (similar to use in chemical burns) to reduce inflammation and prevent symblepharon formation during the first 1 to 2 weeks, bearing in mind that they can potentiate corneal melting.
Topical corticosteroids (similar to use in chemical burns) to reduce inflammation and prevent symblepharon formation during the first 1 to 2 weeks, bearing in mind that they can potentiate corneal melting.
Complications
 Corneal scarring
Corneal scarring
 Irregular astigmatism
Irregular astigmatism
 Decreased vision
Decreased vision
 Infectious keratitis
Infectious keratitis
Prognosis
 Depends on the severity of the injury, especially the exact cause of the burn and duration of contact. Short-contact burns, such as those from curling irons and cigarettes, have an excellent prognosis. Molten metal that adheres to the cornea causes a much more substantial injury. Eyelid damage can cause exposure problems and long-term difficulties with corneal healing.
Depends on the severity of the injury, especially the exact cause of the burn and duration of contact. Short-contact burns, such as those from curling irons and cigarettes, have an excellent prognosis. Molten metal that adheres to the cornea causes a much more substantial injury. Eyelid damage can cause exposure problems and long-term difficulties with corneal healing.
ELECTRICAL BURNS
Ocular electrical burns usually result from electrical injuries to the head or a lightning strike. In addition to corneal and scleral burns, they can also cause acute uveitis. The lens is frequently involved, and cataracts may develop months to years later. Eyelid damage can cause exposure problems and long-term difficulties with corneal healing.
Figure 11-2. Thermal injury. A. A curling iron briefly touched this cornea, causing coagulation of the corneal epithelium and turning it white. It can be removed mechanically or it will slough off naturally. Generally, these eyes recover without sequelae, because the length of time the heat is in contact with the cornea is minimal. Electrical injury. B. An electrical injury caused a localized area of scleral melt with uveal prolapse. Additionally, the electrical injury produced necrosis of a large portion of upper eyelid tissue, resulting in severe exposure. The eye was treated with a scleral patch graft and eyelid skin grafting.

ULTRAVIOLET KERATOPATHY (ARC WELDER’S FLASH)
Severe, painful punctate keratopathy can result hours after exposure to significant levels of ultraviolet light.
Etiology
 Usually caused by welding or using a sunlamp without proper protective eyewear. Milder forms can also be seen in patients with significant sun exposure, such as after a day at the beach or after skiing.
Usually caused by welding or using a sunlamp without proper protective eyewear. Milder forms can also be seen in patients with significant sun exposure, such as after a day at the beach or after skiing.
Symptoms
 Symptoms usually develop 6 to 10 hours after the exposure.
Symptoms usually develop 6 to 10 hours after the exposure.
 Pain, photophobia, foreign-body sensation, tearing, redness, and decreased vision
Pain, photophobia, foreign-body sensation, tearing, redness, and decreased vision
Signs
 Spasm of eyelids in severe cases
Spasm of eyelids in severe cases
 Punctate epithelial erosions, especially in the interpalpebral regions (Fig. 11-3)
Punctate epithelial erosions, especially in the interpalpebral regions (Fig. 11-3)
 Eyelid edema, conjunctival hyperemia
Eyelid edema, conjunctival hyperemia
Treatment
 Preservative-free artificial tears q2–3h
Preservative-free artificial tears q2–3h
 Topical antibiotic drops (e.g., a fluoroquinolone) t.i.d. to q.i.d. and antibiotic ointment (e.g., erythromycin, tetracycline, bacitracin, polymyxin B/bacitracin, or ciprofloxacin) at bedtime. For more severe cases, topical antibiotic ointment q.i.d. will provide more lubrication and comfort.
Topical antibiotic drops (e.g., a fluoroquinolone) t.i.d. to q.i.d. and antibiotic ointment (e.g., erythromycin, tetracycline, bacitracin, polymyxin B/bacitracin, or ciprofloxacin) at bedtime. For more severe cases, topical antibiotic ointment q.i.d. will provide more lubrication and comfort.
 Cycloplegics (e.g., cyclopentolate 1% or scopolamine 0.25% t.i.d.)
Cycloplegics (e.g., cyclopentolate 1% or scopolamine 0.25% t.i.d.)
 Pressure patching or a bandage soft contact lens for severe epithelial erosions
Pressure patching or a bandage soft contact lens for severe epithelial erosions
 Emphasize to the patient the importance of protective eyewear.
Emphasize to the patient the importance of protective eyewear.
Complications
 Rarely, infectious keratitis
Rarely, infectious keratitis
Prognosis
 Typically excellent
Typically excellent
Figure 11-3. Welder’s flash. Significant central punctate epitheliopathy is present in this patient 6 hours after welding without adequate eye protection. (Courtesy of Irving Raber, MD.)

CORNEAL ABRASION
Corneal abrasions result from corneal surface trauma that causes removal of a portion of the epithelial layer.
Etiology
 Mechanical trauma (e.g., fingernail, paper edge, tree branch)
Mechanical trauma (e.g., fingernail, paper edge, tree branch)
 Chemical injuries, medicamentosa keratitis
Chemical injuries, medicamentosa keratitis
 Foreign body
Foreign body
 Contact lens
Contact lens
 Misdirected eyelashes
Misdirected eyelashes
 Neurotrophic or exposure keratopathy
Neurotrophic or exposure keratopathy
 Iatrogenic (e.g., after removal of corneal sutures, epithelial debridement)
Iatrogenic (e.g., after removal of corneal sutures, epithelial debridement)
Symptoms
 Pain, especially upon blinking; foreign-body sensation; photophobia; tearing; redness; often decreased vision
Pain, especially upon blinking; foreign-body sensation; photophobia; tearing; redness; often decreased vision
 Topical anesthetic drops relieve the pain (and facilitate the eye examination).
Topical anesthetic drops relieve the pain (and facilitate the eye examination).
Signs
 Epithelial defect that may be detected grossly or at the slit lamp. It is easily seen with fluorescein dye using the cobalt blue light (Fig. 11-4).
Epithelial defect that may be detected grossly or at the slit lamp. It is easily seen with fluorescein dye using the cobalt blue light (Fig. 11-4).
Treatment
 Search for and remove any foreign body in the conjunctival fornices and under the upper eyelid.
Search for and remove any foreign body in the conjunctival fornices and under the upper eyelid.
 Epilate any misdirected eyelashes.
Epilate any misdirected eyelashes.
 Topical antibiotic ointment (e.g., erythromycin, tetracycline, bacitracin, polymyxin B/bacitracin, or ciprofloxacin) q2–6h. Topical antibiotic drops may be used if the abrasion is small or if the patient finds that ointments blur vision.
Topical antibiotic ointment (e.g., erythromycin, tetracycline, bacitracin, polymyxin B/bacitracin, or ciprofloxacin) q2–6h. Topical antibiotic drops may be used if the abrasion is small or if the patient finds that ointments blur vision.
 Cycloplegics (e.g., cyclopentolate 1% or scopolamine 0.25% t.i.d.)
Cycloplegics (e.g., cyclopentolate 1% or scopolamine 0.25% t.i.d.)
 Pressure patching or a bandage soft contact lens are occasionally used for large defects. Small defects generally do not require patching or bandage soft contact lens.
Pressure patching or a bandage soft contact lens are occasionally used for large defects. Small defects generally do not require patching or bandage soft contact lens.
 For traumatic or contact lens–induced abrasions, bandage contact lenses and patching are relatively contraindicated because they increase the risk of infection. A topical antibiotic with good gram-negative coverage (e.g., a fluoroquinolone, tobramycin, gentamicin, polymyxin B/neomycin/gramicidin) should be used.
For traumatic or contact lens–induced abrasions, bandage contact lenses and patching are relatively contraindicated because they increase the risk of infection. A topical antibiotic with good gram-negative coverage (e.g., a fluoroquinolone, tobramycin, gentamicin, polymyxin B/neomycin/gramicidin) should be used.
Complications
 Corneal scar
Corneal scar
 Infectious keratitis
Infectious keratitis
 Decreased vision
Decreased vision
 Recurrent erosions
Recurrent erosions
Prognosis
 Generally excellent. Patients need to be followed closely until the abrasion heals, especially those at higher risk of infection, such as after contact lens–related and vegetable matter–related trauma and when treated with a bandage soft contact lens.
Generally excellent. Patients need to be followed closely until the abrasion heals, especially those at higher risk of infection, such as after contact lens–related and vegetable matter–related trauma and when treated with a bandage soft contact lens.
Figure 11-4. Corneal abrasion. A. A tennis ball hit the eye of this 12-year-old boy, causing multiple linear corneal abrasions. It also caused a traumatic iritis. B. A triangular corneal abrasion is evident superiorly with the cobalt blue light after fluorescein stain. There is some punctate epithelial staining surrounding the abrasion.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


