Trauma
3.1 CHEMICAL BURN
Treatment should be instituted IMMEDIATELY, even before testing vision, unless an open globe is suspected.
NOTE: This includes alkali (e.g., lye, cements, plasters, airbag powder, bleach, ammonia), acids (e.g., battery acid, pool cleaner, vinegar), solvents, detergents, and irritants (e.g., mace).
Emergency Treatment
1. Copious but gentle irrigation using saline or Ringer lactate solution for at least 30 minutes. Tap water can be used in the absence of these solutions and may be more efficacious in inhibiting elevated intracameral pH than normal saline for alkali burns. NEVER use acidic solutions to neutralize alkalis or vice versa as acid–base reactions themselves can generate harmful substrates. An eyelid speculum and topical anesthetic (e.g., proparacaine) can be placed prior to irrigation. Upper and lower fornices must be everted and irrigated. After exclusion of open globe, particulate matter should be flushed or manually removed. Manual use of intravenous tubing connected to an irrigation solution facilitates the irrigation process.
2. Wait 5 to 10 minutes after irrigation is stopped to allow the dilutant to be absorbed, then check the pH in the fornices using litmus paper. Irrigation is continued until neutral pH is achieved (i.e., 7 to 7.4).
NOTE: The volume of irrigation fluid required to reach neutral pH varies with the chemical and with the duration of the chemical exposure. The volume required may range from a few liters to many liters (more than 8 to 10 L).
3. Conjunctival fornices should be swept with a moistened cotton-tipped applicator or glass rod to remove any sequestered particles of caustic material and necrotic conjunctiva, especially in the case of a persistently abnormal pH. Double eversion of the eyelids with Desmarres eyelid retractors is especially important in identifying and removing particles in the deep fornix. Calcium hydroxide particles may be more easily removed with a cotton-tipped applicator soaked in disodium ethylenediaminetetraacetic acid.
4. Acidic or basic foreign bodies embedded in the conjunctiva, cornea, sclera, or surrounding tissues may require surgical debridement or removal.
MILD-TO-MODERATE BURNS
Signs
(See Figure 3.1.1.)
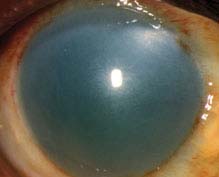
FIGURE 3.1.1. Alkali burn.
Critical. Corneal epithelial defects range from scattered superficial punctate keratopathy (SPK), to focal epithelial loss, to sloughing of the entire epithelium. No significant areas of peri limbal ischemia are seen (i.e., no blanching of the conjunctival or episcleral vessels).
Other. Focal areas of conjunctival epithelial defect, chemosis, hyperemia, hemorrhages, or a combination of these; mild eyelid edema; mild anterior chamber (AC) reaction; first- and second-degree burns of the periocular skin with or without lash loss.
NOTE: If you suspect an epithelial defect but do not see one with fluorescein staining, repeat the fluorescein application to the eye. Sometimes the defect is slow to take up the dye. If the entire epithelium sloughs off, only Bowman membrane remains, which may take up fluorescein poorly.
Work-Up
1. History: Time of injury? Specific type of chemical? Time between exposure until irrigation was started? Duration of and type of irrigation? Eye protection? Sample of agent, package or label, or material safety data sheets are helpful in identifying and treating the exposing agent.
2. Slit-lamp examination with fluorescein staining. Eyelid eversion to search for foreign bodies. Evaluate for conjunctival or corneal ulcerations or defects. Check the intraocular pressure (IOP). In the presence of a distorted cornea, IOP may be most accurately measured with a Tono-Pen or pneumotonometer. Gentle palpation may be used if necessary.
Treatment
1. See Emergency Treatment above.
2. Cycloplegic (e.g., scopolamine 0.25%). If limbal ischemia is suspected, avoid phenylephrine because of its vasoconstrictive properties.
3. Topical antibiotic ointment (e.g., erythromycin) q1–2h while awake or pressure patch for 24 hours.
4. Oral pain medication (e.g., acetaminophen with or without codeine) as needed.
5. If IOP is elevated, acetazolamide 250 mg p.o. q.i.d., acetazolamide 500 mg sequel p.o. b.i.d. or methazolamide 25 to 50 mg p.o. b.i.d. or t.i.d. may be given. Electrolytes, especially potassium, should be monitored in patients on these medications. Add a topical beta-blocker (e.g., timolol 0.5% b.i.d.) if additional IOP control is required. Alpha-agonists may be avoided because of their vasoconstrictive properties.
6. Frequent (e.g., q1h while awake) use of preservative-free artificial tears or gel if not pressure patched.
Follow-Up
Daily initially and then every few days until the corneal epithelial defect is healed. Topical steroids may then be used to reduce significant inflammation. Monitor for corneal epithelial breakdown, stromal thinning, and infection.
SEVERE BURNS
Signs (in addition to the above)
Critical. Pronounced chemosis and conjunctival blanching, corneal edema and opacification, a moderate-to-severe AC reaction (may not be appreciated if the cornea is opaque).
Other. Increased IOP, second- and third-degree burns of the surrounding skin, and local necrotic retinopathy as a result of direct penetration of alkali through the sclera.
Work-Up
Same as for mild-to-moderate burns.
Treatment
1. See Emergency Treatment above.
2. Hospital admission rarely needed for close monitoring of IOP and corneal healing.
3. Debride necrotic tissue containing foreign matter.
4. Cycloplegic (e.g., scopolamine 0.25% or atropine 1%, b.i.d. to t.i.d.). Avoid phenylephrine because it is a vasoconstrictor.
5. Topical antibiotic (e.g., trimethoprim/polymyxin B or fluoroquinolone drops q.i.d.; erythromycin or bacitracin ointment four to nine times per day).
6. Topical steroid (e.g., prednisolone acetate 1% or dexamethasone 0.1% four to nine times per day) if significant AC or corneal inflammation is present. May use a combination antibiotic—steroids such as tobramycin/dexamethasone drops or ointment q1–2h.
7. Consider a pressure patch between drops or ointment.
8. Antiglaucoma medications as above if the IOP is increased or cannot be determined.
9. Frequent (e.g., q1h while awake) use of preservative-free artificial tears or gel if not using frequent ointments.
10. Oral tetracyclines may also reduce collagenolysis and stromal melting (e.g., doxycycline 100 mg p.o. b.i.d.).
11. Lysis of conjunctival adhesions b.i.d. by using a glass rod or a moistened cotton-tipped applicator covered with an antibiotic ointment to sweep the fornices may be helpful. If symblepharon begins to form despite attempted lysis, consider using a scleral shell or ring to maintain the fornices.
12. Other considerations:
—Therapeutic soft contact lens, collagen shield, amniotic membrane graft (e.g., Pro-Kera or sutured/glued), or tarsorrhaphy (usually used if healing is delayed beyond 2 weeks).
—Ascorbate and citrate for alkali burns has been reported to speed healing time and allow better visual outcome. Administration has been studied intravenously (i.v.), orally (ascorbate 500 to 2,000 mg q.d.), and topically (ascorbate 10% q1h). Caution in patients with renal compromise secondary to potential renal toxicity.
—If any melting of the cornea occurs, other collagenase inhibitors may be used. (e.g., acetylcysteine 10% to 20% drops q4h).
—If the melting progresses (or the cornea perforates), consider cyanoacrylate tissue adhesive. An emergency patch graft or corneal transplantation may be necessary; however, the prognosis is better if this procedure is performed at least 12 to 18 months after the injury.
Follow-Up
These patients need to be monitored closely, either in the hospital or daily as outpatients. Topical steroids should be tapered after 7 to 10 days because they can promote corneal melting. Long-term use of preservative-free artificial tears q1–6h and lubricating ointments q.h.s to q.i.d may be required. A severely dry eye may require a tarsorrhaphy or a conjunctival flap. Conjunctival or limbal stem cell transplantation from the fellow eye may be performed in unilateral injuries that fail to heal within several weeks to several months.
SUPER GLUE (CYANOACRYLATE) INJURY TO THE EYE
NOTE: Rapid-setting super glues harden quickly on contact with moisture.
Treatment
1. If the eyelids are glued together, they can be separated with gentle traction. Lashes may need to be cut to separate the eyelids. Misdirected lashes, hardened glue mechanically rubbing the cornea, and glue adherent to the cornea should be carefully removed with fine forceps. Copious irrigation with warm normal saline or warm compresses may be used to loosen hardened glue on the lids, lashes, cornea, or conjunctiva.
2. Epithelial defects are treated as corneal abrasions (see 3.2, Corneal Abrasion).
3. Warm compresses q.i.d. may help remove any remaining glue stuck in the lashes that did not require urgent removal.
Follow-Up
Daily until corneal epithelial defects are healed.
3.2 Corneal Abrasion
Symptoms
Sharp pain, photophobia, foreign body sensation, tearing, discomfort with blinking, history of scratching, or hitting the eye.
Signs
(See Figure 3.2.1.)
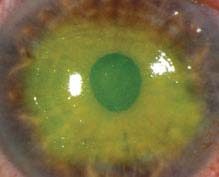
FIGURE 3.2.1. Corneal abrasion with fluorescein staining.
Critical. Epithelial defect that stains with fluorescein, absence of underlying corneal opacification (presence of which indicates infection or inflammation).
Other. Conjunctival injection, swollen eyelid, mild AC reaction.
Differential Diagnosis
 Recurrent erosion (see 4.2, Recurrent Corneal Erosion).
Recurrent erosion (see 4.2, Recurrent Corneal Erosion).
 Herpes simplex keratitis (see 4.15, Herpes Simplex Virus).
Herpes simplex keratitis (see 4.15, Herpes Simplex Virus).
 Confluent SPK (see 4.1, Superficial Punctate Keratopathy).
Confluent SPK (see 4.1, Superficial Punctate Keratopathy).
Work-Up
1. Slit-lamp examination: Use fluorescein dye, measure the size (e.g., height and width) of the abrasion, and diagram its location. Evaluate for an AC reaction, infiltrate (underlying corneal opacification), corneal laceration, and penetrating trauma.
2. Evert the eyelids to ensure that no foreign body is present, especially in the presence of vertical or linear abrasions.
Treatment
1. Antibiotic
—Noncontact lens wearer: Antibiotic ointment (e.g., erythromycin, bacitracin, or bacitracin/polymyxin B q2–4h) or antibiotic drops (e.g., polymyxin B/trimethoprim or a fluoroquinolone q.i.d.). Abrasions secondary to fingernails or vegetable matter should be covered with a fluoroquinolone drop (e.g., ciprofloxacin, moxifloxacin) or ointment (e.g., ciprofloxacin) at least q.i.d.
—Contact lens wearer: Must have antipseudomonal coverage. May use antibiotic ointment or antibiotic drops at least q.i.d.
NOTE: The decision to use drops versus ointment depends on the needs of the patient. Ointments offer better barrier and lubricating function between eyelid and abrasion but tend to blur vision temporarily. They may be used to augment drops at bedtime. We prefer frequent ointments.
2. Cycloplegic agent (e.g., cyclopentolate 1% to 2% b.i.d or t.i.d.) for traumatic iritis which may develop 24 to 72 hours after trauma. Avoid steroid use for iritis with epithelial defects because it may retard epithelial healing and increase the risk of infection. Avoid use of long-acting cycloplegics for small abrasions to allow for faster visual recovery.
3. Patching is rarely necessary. Patching may be helpful for comfort, but DO NOT patch if the mechanism of injury involves vegetable matter, fingernails, or if the patient wears contact lenses. Be careful that the patch is properly placed so that the upper lid is totally prevented from opening as this can cause a serious abrasion.
4. Consider topical nonsteroidal anti-inflammatory drug (NSAID) drops (e.g., ketorolac 0.4% to 0.5% q.i.d. for 3 days) for pain control. Avoid in patients with other ocular surface disease and in postoperative patients. Oral acetaminophen, NSAIDs, or narcotics (in severe cases) can also be used for pain control.
5. Debride loose or hanging epithelium because it may inhibit healing. A cotton-tipped applicator soaked in topical anesthetic (e.g., proparacaine) or a sterile jewelers forceps (used with caution) may be utilized.
6. No contact lens wear. Some clinicians use bandage contact lenses for therapy. We rarely do unless the size of the abrasion and discomfort warrants it and there is poor healing in the absence of infection. If a bandage contact lens is used, patients should use prophylactic topical antibiotics (e.g., polymyxin B/trimethoprim or a fluoroquinolone q.i.d.) and should be followed-up daily for evaluation and contact lens replacement.
Follow-Up
Noncontact Lens Wearer
1. If patched or given bandage contact lens, the patient should return in 24 hours (or sooner if the symptoms worsen) for re-evaluation.
2. Central or large corneal abrasion: Return the next day to determine if the epithelial defect is improving. If the abrasion is healing, may see 2 to 3 days later. Instruct the patient to return sooner if symptoms worsen. Revisit every 3 to 5 days until healed.
3. Peripheral or small abrasion: Return 2 to 5 days later. Instruct the patient to return sooner if symptoms worsen. Revisit every 3 to 5 days until healed.
Contact Lens Wearer
Close follow-up until the epithelial defect resolves, and then treat with topical fluoroquinolone or tobramycin drops for an additional 1 or 2 days. The patient may resume contact lens wear after the eye feels normal for a week after the cession of a proper course of medication. A new contact lens should be instituted at that time.
3.3 Corneal and Conjunctival Foreign Bodies
Symptoms
Foreign body sensation, tearing, history of trauma.
Signs
(See Figure 3.3.1.)
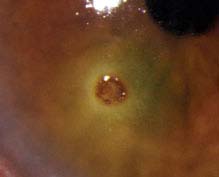
FIGURE 3.3.1. Corneal metallic foreign body with rust ring.
Critical. Conjunctival or corneal foreign body with or without a rust ring.
Other. Conjunctival injection, eyelid edema, mild AC reaction, and SPK. A small infiltrate may surround a corneal foreign body; it is usually reactive and sterile. Vertically oriented linear corneal abrasions or SPK may indicate a foreign body under the upper eyelid.
Work-Up
1. History: Determine the mechanism of injury [e.g., metal striking metal, power tools or weed-whackers may suggest an intraocular foreign body (IOFB), direct pathway with no safety glasses, distance of the patient from the site, etc.]. Attempt to determine the size, weight, velocity, force, shape, and composition of the object.
2. Document visual acuity before any procedure is performed. One or two drops of topical anesthetic may be necessary to control blepharospasm and pain.
3. Slit-lamp examination: Locate and assess the depth of the foreign body. Examine closely for possible entry sites (rule out self-sealing lacerations) pupil irregularities, iris tears and transillumination defects (TIDs), capsular perforations, lens opacities, hyphema, AC shallowing (or deepening in scleral perforations), and asymmetrically low IOP in the involved eye.
NOTE: There may be multiple IOFBs with power equipment or explosive debris.
If there is no evidence of perforation, evert the eyelids and inspect the fornices for additional foreign bodies. Double everting the upper eyelid with a Desmarres eyelid retractor may be necessary. Carefully inspect a conjunctival laceration to rule out a scleral laceration or perforation. Measure the dimensions of any infiltrate and the degree of any AC reaction for monitoring therapy response and progression of possible infection.
NOTE: An infiltrate accompanied by a significant AC reaction, purulent discharge, or extreme conjunctival injection and pain should be cultured to rule out an infection, treated aggressively with antibiotics, and followed intensively (see 4.11, Bacterial Keratitis).
4. Dilate the eye and examine the posterior segment for a possible IOFB (see 3.15, Intraocular Foreign Body).
5. Consider a B-scan ultrasonography, a computed tomography (CT) scan of the orbit (axial and coronal views, 1-mm sections), or ultrasonographic biomicroscopy (UBM) to exclude an intraocular or intraorbital foreign body. Avoid magnetic resonance imaging (MRI) if there is a history of possible metallic foreign body.
Treatment
Corneal Foreign Body (Superficial or Partial Thickness)
1. Apply topical anesthetic (e.g., proparacaine). Remove the corneal foreign body with a foreign body spud, fine forceps, or small-gauge needle at a slit lamp. Multiple superficial foreign bodies may be more easily removed by irrigation.
NOTE: If there is concern for full-thickness corneal foreign body, exploration and removal should be performed in the operating room.
2. Remove the rust ring as completely as possible on the first attempt. This may require an ophthalmic burr (see Figure 3.3.2). It is sometimes safer to leave a deep, central rust ring to allow time for the rust to migrate to the corneal surface, at which point it can be removed more easily.

FIGURE 3.3.2. Burr removal of metallic rust ring.
3. Measure the size of the resultant corneal epithelial defect.
4. Treat as for corneal abrasion (see 3.2, Corneal Abrasion).
NOTE: Erythromycin ointment should not be used for residual epithelial defects from corneal foreign bodies as it does not provide strong enough antibiotic coverage.
5. Alert the patient to return as soon as possible if there is any worsening of symptoms.
Conjunctival Foreign Body
1. Remove foreign body under topical anesthesia.
—Multiple or loose superficial foreign bodies can often be removed with saline irrigation.
—A foreign body can be removed with a cotton-tipped applicator soaked in topical anesthetic or with fine forceps. For deeply embedded foreign bodies, consider pretreatment with a cotton-tipped applicator soaked in phenylephrine 2.5% to reduce conjunctival bleeding.
—Small, relatively inaccessible, buried subconjunctival foreign bodies may sometimes be left in the eye without harm unless they are infectious or proinflammatory. Occasionally they will surface with time, at which point they may be removed more easily. Conjunctival excision is sometimes indicated.
—Check the pH if an associated chemical injury is suspected (e.g., alkali from fireworks). See 3.1, Chemical Burn.
2. Sweep the conjunctival fornices with a glass rod or cotton-tipped applicator soaked with a topical anesthetic to remove any remaining pieces.
3. See 3.4, Conjunctival Laceration if there is a significant conjunctival laceration.
4. A topical antibiotic (e.g., bacitracin ointment, trimethoprim/polymyxin B drops, or fluoroquinolone drops q.i.d.) may be used.
5. Preservative-free artificial tears may be given as needed for irritation.
Follow-Up
1. Corneal foreign body: Follow-up as with corneal abrasion (see 3.2, Corneal Abrasion). If residual rust ring remains, re-evaluate in 24 hours.
2. Conjunctival foreign body: Follow-up as needed, or in 1 week if residual foreign bodies were left in the conjunctiva.
3.4 Conjunctival Laceration
Symptoms
Mild pain, red eye, foreign body sensation; usually, a history of ocular trauma.
Signs
Fluorescein staining of the conjunctiva. The conjunctiva may be torn and rolled up on itself. Exposed white sclera may be noted. Conjunctival and subconjunctival hemorrhages are often present.
Work-Up
1. History: Determine the nature of the trauma and whether a ruptured globe or intraocular or intraorbital foreign body may be present. Evaluate the mechanism for possible foreign body involvement, including size, shape, weight, and velocity of object.
2. Complete ocular examination, including careful exploration of the sclera (after topical anesthesia, e.g., proparacaine or viscous lidocaine) in the region of the conjunctival laceration to rule out a scleral laceration or a subconjunctival foreign body. The entire area of sclera under the conjunctival laceration must be inspected. Since the conjunctiva is mobile, inspect a wide area of the sclera under the laceration. Use a proparacaine-soaked, sterile cotton-tipped applicator to manipulate the conjunctiva. Irrigation with saline may be helpful in removing scattered debris. A Seidel test may be helpful (see Appendix 5, Seidel Test to Detect a Wound Leak). Dilated fundus examination, especially evaluating the area underlying the conjunctival injury, must be carefully performed with indirect ophthalmoscopy.
3. Consider a CT scan of the orbit (axial and coronal views, 1-mm sections) to exclude an intraocular or intraorbital foreign body. B-scan ultrasound may be helpful.
4. Exploration of the site in the operating room under general anesthesia may be necessary when a ruptured globe is suspected, especially in children.
5. Children often do not give an accurate history of trauma. They and nearby observers must be questioned and ophthalmic examination must be especially detailed.
Treatment
In case of a ruptured globe or penetrating ocular injury, see 3.14, Ruptured Globe and Penetrating Ocular Injury. Otherwise:
1. Antibiotic ointment (e.g., erythromycin, bacitracin or bacitracin/polymyxin B q.i.d.). A pressure patch may rarely be used for the first 24 hours for comfort.
2. Most lacerations will heal without surgical repair. Some large lacerations (≥1 to 1.5 cm) may be sutured with 8-0 polyglactin 910 (e.g., Vicryl). When suturing, take care not to bury folds of conjunctiva or incorporate Tenon capsule into the wound. Avoid suturing the plica semilunaris or caruncle to the conjunctiva.
Follow-Up
If there is no concomitant ocular damage, patients with large conjunctival lacerations are re-examined within 1 week. Patients with small injuries are seen as needed and told to return immediately if there is a worsening of symptoms.
3.5 Traumatic Iritis
Symptoms
Dull, aching or throbbing pain, photophobia, tearing, onset of symptoms usually within 3 days of trauma.
Signs
Critical. White blood cells (WBCs) and flare in the AC (seen under high-power magnification by focusing into the AC with a small, bright, tangential beam from the slit lamp).
Other. Pain in the traumatized eye when light enters either eye; lower (due to ciliary body shock) or higher (due to inflammatory debris and/or trabeculitis) IOP; smaller, poorly dilating pupil or larger pupil (due to iris sphincter tears) in the traumatized eye; perilimbal conjunctival injection; decreased vision; occasionally floaters.
Differential Diagnosis
 Nongranulomatous anterior uveitis: No history of trauma, or the degree of trauma is not consistent with the level of inflammation. See 12.1, Anterior Uveitis (Iritis/
Nongranulomatous anterior uveitis: No history of trauma, or the degree of trauma is not consistent with the level of inflammation. See 12.1, Anterior Uveitis (Iritis/
Iridocyclitis).
 Traumatic microhyphema or hyphema: Red blood cells (RBCs) suspended in the AC. See 3.6, Hyphema and Microhyphema.
Traumatic microhyphema or hyphema: Red blood cells (RBCs) suspended in the AC. See 3.6, Hyphema and Microhyphema.
 Traumatic corneal abrasion: May have an accompanying AC reaction. See 3.2, Corneal Abrasion.
Traumatic corneal abrasion: May have an accompanying AC reaction. See 3.2, Corneal Abrasion.
 Traumatic retinal detachment: May produce an AC reaction or may see pigment in the anterior vitreous. See 11.3, Retinal Detachment.
Traumatic retinal detachment: May produce an AC reaction or may see pigment in the anterior vitreous. See 11.3, Retinal Detachment.
Work-Up
Complete ophthalmic examination, including IOP measurement and dilated fundus examination.
Treatment
Cycloplegic agent (e.g., cyclopentolate 2% t.i.d. or scopolamine 0.25% b.i.d.). May use a steroid drop (e.g., prednisolone acetate 0.125% to 1% q.i.d.). Avoid topical steroids if an epithelial defect is present.
Follow-Up
1. Recheck in 5 to 7 days.
2. If resolved, the cycloplegic agent is discontinued and the steroid is tapered.
3. One month after trauma, perform gonioscopy to look for angle recession and indirect ophthalmoscopy with scleral depression to detect retinal breaks or detachment.
3.6 Hyphema and Microhyphema
TRAUMATIC HYPHEMA
Symptoms
Pain, blurred vision, history of blunt trauma.
Signs
(See Figure 3.6.1.)

FIGURE 3.6.1. Hyphema.
Blood or clot or both in the AC, usually visible without a slit lamp. A total (100%) hyphema may be black or red. When black, it is called an “8-ball” or “black ball” hyphema, indicating deoxygenated blood; when red, the circulating blood cells may settle with time to become less than a 100% hyphema.
Work-Up
1. History: Mechanism (including force, velocity, type, and direction) of injury? Protective eyewear? Time of injury? Time and extent of visual loss? Usually the visual compromise occurs at the time of injury; decreasing vision over time suggests a rebleed or continued bleed (which may cause an IOP rise). Use of medications with anticoagulant properties (aspirin, NSAIDs, warfarin, or clopidogrel)? Personal or family history of sickle cell disease or trait? Symptoms of coagulopathy (e.g., bloody nose blowing, bleeding gums with tooth brushing, easy bruising, bloody stool)?
2. Ocular examination, first ruling out a ruptured globe (see 3.14, Ruptured Globe and Penetrating Ocular Injury). Evaluate for other traumatic injuries. Document the extent (e.g., measure the hyphema height) and location of any clot and blood. Measure the IOP. Perform a dilated retinal evaluation without scleral depression. Consider a gentle B-scan ultrasound if the view of the fundus is poor. Avoid gonioscopy unless intractable increased IOP develops. If gonioscopy is necessary, perform gently. Consider UBM to evaluate the anterior segment if the view is poor and lens capsule rupture, IOFB, or other anterior-segment abnormalities are suspected.
3. Consider a CT scan of the orbits and brain (axial and coronal views, with 1-mm sections through the orbits) when indicated (e.g., suspected orbital fracture or IOFB, loss of consciousness).
4. Patients should be screened for sickle cell trait or disease (order Sickledex screen; if necessary, may check hemoglobin electrophoresis) as clinically appropriate.
Treatment
Many aspects remain controversial, including whether hospitalization and absolute bed rest are necessary, but an atraumatic upright environment is essential. Consider hospitalization for noncompliant patients, patients with bleeding diathesis or blood dyscrasia, patients with other severe ocular or orbital injuries, and patients with concomitant significant IOP elevation and sickle cell. In addition, consider hospitalization and aggressive treatment for children, especially those at risk for amblyopia (e.g., those under age 7 to 10), when a thorough clinical exam is difficult, or when child abuse is suspected.
1. Confine either to bed rest with bathroom privileges or to limited activity. Elevate the head of bed to allow blood to settle. Discourage bending or heavy lifting.
2. Place a shield (metal or clear plastic) over the involved eye at all times. Do not patch because this prevents recognition of sudden visual change in the event of a rebleed.
3. Atropine 1% solution b.i.d. to t.i.d. or scopolamine 0.25% b.i.d. to t.i.d.
4. Avoid aspirin-containing products or NSAIDs unless otherwise medically necessary. Consult with prescribing physicians regarding the need for anticoagulant therapy.
5. Mild analgesics only (e.g., acetaminophen). Avoid sedatives.
6. Use topical steroids (e.g., prednisolone acetate 1% q.i.d. to q1h) if any suggestion of iritis (e.g., photophobia, deep ache, ciliary flush), evidence of lens capsule rupture, any protein (e.g., fibrin), or definitive WBCs in AC. Taper the frequency of steroids quickly as soon as signs and symptoms resolve to reduce the likelihood of steroid-induced glaucoma.
NOTE: No definitive evidence exists regarding the use of steroids in improving outcomes for hyphemas. Use must be balanced with the risks of topical steroids (increased infection potential, increased IOP, cataract). In children, particular caution must be used regarding topical steroids. Children often get rapid rises in IOP and with prolonged use there is a significant risk for cataract. As outlined above, in certain cases steroids may be beneficial, but steroids should be prescribed in an individualized manner. Children must be monitored closely for increased IOP and should be tapered off the steroids as soon as possible.
7. For increased IOP:
NOTE: Increased IOP, especially soon after trauma, may be transient, secondary to acute mechanical plugging of the trabecular meshwork. Elevating the patient’s head may decrease the IOP by causing RBCs to settle inferiorly and clot.
—Non—sickle-cell disease or trait (≥30 mm Hg):
 Start with a beta-blocker (e.g., timolol or levobunolol 0.5% b.i.d.).
Start with a beta-blocker (e.g., timolol or levobunolol 0.5% b.i.d.).
 If IOP is still high, add topical alpha-agonist (e.g., apraclonidine 0.5% or brimonidine 0.15% t.i.d.) or topical carbonic anhydrase inhibitor (e.g., dorzolamide 2% or brinzolamide 1% t.i.d.). Avoid prostaglandin analogs and miotics (may increase inflammation). In children under 5, topical alpha-agonists are contraindicated.
If IOP is still high, add topical alpha-agonist (e.g., apraclonidine 0.5% or brimonidine 0.15% t.i.d.) or topical carbonic anhydrase inhibitor (e.g., dorzolamide 2% or brinzolamide 1% t.i.d.). Avoid prostaglandin analogs and miotics (may increase inflammation). In children under 5, topical alpha-agonists are contraindicated.
 If topical therapy fails, add acetazolamide (500 mg p.o. q12h for adults, 20 mg/kg/day divided three times per day for children) or mannitol [1 to 2 g/kg i.v. over 45 minutes q24h]. If mannitol is necessary to control the IOP, surgical evacuation may be imminent.
If topical therapy fails, add acetazolamide (500 mg p.o. q12h for adults, 20 mg/kg/day divided three times per day for children) or mannitol [1 to 2 g/kg i.v. over 45 minutes q24h]. If mannitol is necessary to control the IOP, surgical evacuation may be imminent.
—Sickle-cell disease or trait (≥24 mm Hg):
 Start with a beta-blocker (e.g., timolol or levobunolol 0.5% b.i.d.).
Start with a beta-blocker (e.g., timolol or levobunolol 0.5% b.i.d.).
 All other agents must be used with extreme caution: Topical dorzolamide and brinzolamide may reduce aqueous pH and induce increased sickling; topical alpha-agonists (e.g., brimonidine or apraclonidine) may affect iris vasculature; miotics and prostaglandins may promote inflammation.
All other agents must be used with extreme caution: Topical dorzolamide and brinzolamide may reduce aqueous pH and induce increased sickling; topical alpha-agonists (e.g., brimonidine or apraclonidine) may affect iris vasculature; miotics and prostaglandins may promote inflammation.
 If possible, avoid systemic diuretics because they promote sickling by inducing systemic acidosis and volume contraction. If a carbonic anhydrase inhibitor is necessary, use methazolamide 50 mg p.o. q8h instead of acetazolamide (controversial). If mannitol is necessary to control the IOP, surgical evacuation may be imminent.
If possible, avoid systemic diuretics because they promote sickling by inducing systemic acidosis and volume contraction. If a carbonic anhydrase inhibitor is necessary, use methazolamide 50 mg p.o. q8h instead of acetazolamide (controversial). If mannitol is necessary to control the IOP, surgical evacuation may be imminent.
 AC paracentesis may be considered if IOP cannot be safely lowered medically (see Appendix 13, Anterior Chamber Paracentesis). This procedure is often only a temporizing measure when the need for surgical evacuation is anticipated.
AC paracentesis may be considered if IOP cannot be safely lowered medically (see Appendix 13, Anterior Chamber Paracentesis). This procedure is often only a temporizing measure when the need for surgical evacuation is anticipated.
8. If hospitalized, use antiemetics p.r.n. for severe nausea or vomiting [e.g., prochlorperazine 10 mg intramuscularly (i.m.) q8h or 25 mg q12h p.r.n.; ≤12 years of age, trimethobenzamide suppositories, 100 mg PR q6h p.r.n.].
9. Indications for surgical evacuation of hyphema:
—Corneal stromal blood staining.
—Significant visual deterioration.
—Hyphema that does not decrease to ≤50% by 8 days (to prevent peripheral anterior synechiae).
—IOP ≥60 mm Hg for ≥48 hours, despite maximal medical therapy (to prevent optic atrophy).
—IOP ≥25 mm Hg with total hyphema for ≥5 days (to prevent corneal stromal blood staining).
—IOP 24 mm Hg for ≥24 hours (or any transient increase in IOP ≥30 mm Hg) in sickle trait or disease patients.
—Consider early surgical intervention for children at risk for amblyopia.
NOTE: Previously, systemic aminocaproic acid was used in hospitalized patients to stabilize the clot and to prevent rebleeding. This therapy is rarely used now. Topical aminocaproic acid is currently under research and development. Preliminary studies suggest that it may be useful in reducing the risk of rebleeding. Further research is needed before the role for topical aminocaproic acid in the management of hyphemas can be determined.
Follow-Up
1. The patient should be seen daily after initial trauma to check visual acuity, IOP, and for a slit-lamp examination. Look for new bleeding (most commonly occurs within the first 5 to 10 days), increased IOP, corneal blood staining, and other intraocular injuries as the blood clears (e.g., iridodialysis; subluxated or dislocated lens, or cataract). Hemolysis, which may appear as bright red fluid, should be distinguished from a rebleed, which forms a new, bright red clot. If the IOP is increased, treat as described earlier. Time between visits may be increased once consistent improvement in clinical exam is documented.
2. The patient should be instructed to return immediately if a sudden increase in pain or decrease in vision is noted (which may be symptoms of a rebleed or increased IOP).
3. If a significant rebleed or an intractable IOP increase occurs, hospitalization or surgical evacuation should be considered.
4. After the initial close follow-up period, the patient may be maintained on a long-acting cycloplegic (e.g., atropine 1% solution q.d. to b.i.d., scopolamine 0.25% q.d. to b.i.d.), depending on the severity of the condition. Topical steroids may be tapered as the blood, fibrin, and WBCs resolve.
5. Glasses or eye shield during the day and eye shield at night. As with any patient, protective eyewear (polycarbonate shatterproof lenses) should be worn any time significant potential for an eye injury exists.
6. The patient must refrain from strenuous physical activities (including bearing down or Valsalva maneuvers) for 1 week after the initial injury or rebleed. Normal activities may be resumed once the hyphema has resolved and patient is out of rebleed time frame.
7. Future outpatient follow-up:
—If the patient was hospitalized, see 2 to 3 days after discharge. If not hospitalized, see several days to 1 week after initial daily follow-up period, depending on the severity of condition (amount of blood, potential for IOP increase, other ocular or orbital pathologic processes).
—Four weeks after trauma for gonioscopy and dilated fundus examination with scleral depression for all patients.
—Some experts suggest annual follow-up because of the potential for development of angle-recession glaucoma.
—If any complications arise, more frequent follow-up is required.
—If filtering surgery was performed, follow-up and activity restrictions are based on the surgeon’s specific recommendations.
TRAUMATIC MICROHYPHEMA
Symptoms
See Hyphema above.
Signs
Suspended RBCs only in the AC, visible only with a slit lamp. Sometimes there may be enough suspended RBCs to see a haziness of the AC (e.g., poor visualization of iris details) without a slit lamp; in these cases, the RBCs may settle out as a frank hyphema.
Work-Up
See Hyphema above.
Treatment
1. Most microhyphemas can be treated on an outpatient basis.
2. Scopolamine 0.25% b.i.d. or atropine 1% q.d. In children, scopolamine is usually preferred.
3. Otherwise, see treatment for Hyphema above.
Follow-Up
1. The patient should return on the third day after the initial trauma and again at 1 week. If the IOP is >25 mm Hg at presentation, the patient should be followed for 3 consecutive days for pressure monitoring, and again at 1 week. Sickle-cell–positive patients with initial IOP of ≥24 mm Hg should also be followed for 3 consecutive days.
2. Otherwise, see follow-up for hyphema above.
NONTRAUMATIC (SPONTANEOUS) AND POSTSURGICAL HYPHEMA OR MICROHYPHEMA
Symptoms
May present with decreased vision or with transient visual loss (intermittent bleeding may cloud vision temporarily).
Etiology of Spontaneous Hyphema or Microhyphema
 Occult trauma: must be excluded, evaluate for child or elder abuse.
Occult trauma: must be excluded, evaluate for child or elder abuse.
 Neovascularization of the iris or angle (e.g., from diabetes, old central retinal vein occlusion, ocular ischemic syndrome, chronic uveitis).
Neovascularization of the iris or angle (e.g., from diabetes, old central retinal vein occlusion, ocular ischemic syndrome, chronic uveitis).
 Blood dyscrasias and coagulopathies.
Blood dyscrasias and coagulopathies.
 Iris–intraocular lens chafing.
Iris–intraocular lens chafing.
 Herpetic keratouveitis.
Herpetic keratouveitis.
 Use of anticoagulants (e.g., ethanol, aspirin, warfarin).
Use of anticoagulants (e.g., ethanol, aspirin, warfarin).
 Other (e.g., iris microaneurysm, leukemia, iris or ciliary body melanoma, retinoblastoma, juvenile xanthogranuloma, Fuchs heterochromic iridocyclitis).
Other (e.g., iris microaneurysm, leukemia, iris or ciliary body melanoma, retinoblastoma, juvenile xanthogranuloma, Fuchs heterochromic iridocyclitis).
Work-Up
As for traumatic hyphemas, plus:
1. Gentle gonioscopy initially to evaluate neovascularization or masses in the angle.
2. Consider the following studies:
—Prothrombin time/INR, partial thromboplastin time, complete blood count with platelet count, bleeding time, proteins C and S.
—Fluorescein angiogram of iris.
—UBM to evaluate position of intraocular lens haptics, ciliary body masses or other anterior-segment pathology.
Treatment
Cycloplegia with atropine 1% solution q.d. to t.i.d., or scopolamine 0.25% q.d. to t.i.d., limited activity, elevation of head of bed, and avoidance of medically unnecessary anticoagulants (e.g., aspirin and NSAIDs). Recommend protective plastic or metal shield if etiology unclear. Monitor IOP. Postsurgical hyphemas and microhyphemas are usually self-limited and often require observation only, with close attention to IOP.
3.7 Iridodialysis/Cyclodialysis
Definitions
Iridodialysis: Disinsertion of the iris from the scleral spur. Elevated IOP can result from damage to the trabecular meshwork or from the formation of peripheral anterior synechiae.
Cyclodialysis: Disinsertion of the ciliary body from the scleral spur. Increased uveoscleral outflow occurs initially resulting in hypotony. IOP elevation can later result from closure of a cyclodialysis cleft, leading to glaucoma.
Symptoms
Usually asymptomatic unless glaucoma or hypotony/hypotony maculopathy develop. Large iridodialyses may be associated with monocular diplopia, glare, and photophobia. Both are associated with blunt trauma or penetrating globe injuries. Typically unilateral.
Signs
(See Figure 3.7.1.)

FIGURE 3.7.1. Iridodialysis.
Critical. Characteristic gonioscopic findings as described above.
Other. Decreased or elevated IOP, glaucomatous optic nerve changes (see 9.1, Primary Open-Angle Glaucoma), angle recession, and hypotony syndrome (see 13.11, Hypotony Syndrome). Other signs of trauma include hyphema, cataract and pupillary irregularities.
Differential Diagnosis
In setting of glaucoma, see 9.1, Primary Open-Angle Glaucoma.
Work-Up
See 9.6, Angle-Recession Glaucoma.
Treatment
1. Sunglasses, contact lenses with an artificial pupil, or surgical correction if large iridodialysis and patient symptomatic.
2. If glaucoma develops, treatment is similar to that for primary open-angle glaucoma (see 9.1, Primary Open-Angle Glaucoma). Aqueous suppressants are usually first-line therapy. Miotics are generally avoided because they may reopen cyclodialysis clefts, causing hypotony. Strong mydriatics may close clefts, resulting in pressure spikes. Often these spikes are transient, as the meshwork resumes aqueous filtration.
3. If hypotony syndrome develops due to cyclodialysis clefts, first-line treatment is usually atropine b.i.d to approximate the ciliary body to the sclera and steroids to decrease inflammation. Further surgical treatment as described in section 13.11, Hypotony Syndrome.
Follow-Up
1. See section 9.1, Primary Open-Angle Glaucoma.
2. Carefully monitor both eyes due to the high incidence of delayed open-angle and steroid-response glaucoma in the uninvolved as well as the traumatized eye.
3.8 Eyelid Laceration
Symptoms
Periorbital pain, tearing.
Signs
(See Figure 3.8.1.)

FIGURE 3.8.1. Marginal eyelid laceration.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


