and Yi Ning J. Strube2
(1)
Wright Foundation for Pediatric Ophthalmology and Adult Strabismus Medical Center, Los Angeles, CA, USA
(2)
Queen’s University, Kingston, Ontario, Canada
Keywords
Transposition proceduresKnapp procedureJensen procedureHummelsheim procedureDouble elevator palsy treatmentSplit-tendon transpositionFoster modificationWright modificationAnterior segment ischemiaTransposition surgery is based on changing the location of the muscle insertion so the muscle pulls the eye in a different direction (i.e., changes the vector of forces). Transposition surgeries can be used to treat a rectus muscle paresis, a lost muscle, A and V patterns (Chap. 15), small vertical tropias (Chap. 15), and torsion (Chap. 15). Three transposition procedures are described in this chapter: Knapp, Jensen, and Hummelsheim.
16.1 Knapp Procedure
A full-tendon transfer (Fig. 16.1) was originally described for the management of double elevator palsy, but this procedure also can be used for sixth nerve palsy. The key for successful surgery is symmetrical transposition, to avoid induced vertical or horizontal deviations. Extensive posterior dissection to free the muscle of the intermuscular septum and check ligaments is necessary to mobilize the muscle for the tendon transfer. A possible complication of the full-tendon transfer is anterior segment ischemia. The author prefers the Hummelsheim partial-tendon transfer for the treatment of rectus muscle paralysis. (See Chap. 8 for strategies regarding the treatment of paralytic strabismus.)
Fig. 16.1
This diagram shows the Knapp procedure with the medial rectus (MR) and lateral rectus (LR) muscles transposed superiorly to the insertion of the superior rectus (SR) muscle. This procedure has been described for the treatment of double elevator palsy with poor superior rectus muscle function. Two fornix incisions in the superior temporal and superior nasal quadrants provide the best exposure for this procedure
16.2 Jensen Procedure
The Jensen procedure is a split-tendon transfer with the adjacent muscles tied together but not disinserted (Figs. 16.2, 16.3, and 16.4). This procedure has the advantage of preserving the anterior ciliary arteries and diminishing the risk of anterior segment ischemia. Even with the Jensen procedure, however, some vascular compromise occurs, and anterior segment ischemia has been associated with this procedure. Good exposure can be obtained by placing two separate fornix incisions on either side of the paretic muscle.
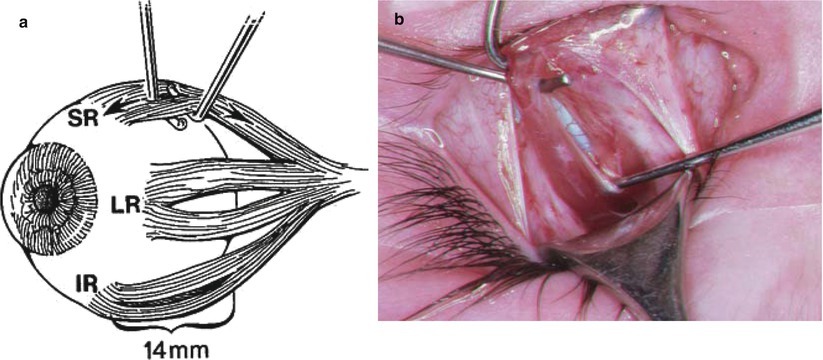
Fig. 16.2




(a) The Jensen procedure used for a left sixth nerve palsy. The superior rectus (SR), inferior rectus (IR), and lateral rectus (LR) muscles are isolated and cleared of surrounding check ligaments and intermuscular septum. Each of the muscles is split exactly one-half tendon width, using two small Stevens hooks. When splitting the superior and inferior rectus muscles, avoid the anterior ciliary arteries. The muscles should be split at least 12–14 mm posterior to the insertion. (b) The left superior rectus muscle is being split with two small Stevens hooks (surgeon’s view). Notice that posterior exposure can be enhanced by removing the lid speculum and inserting a Desmarres retractor under the upper lid
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
