Key points
- •
A transfacial or craniofacial approach allows for wide, potentially en bloc resection and is ideal for tumors that involve surrounding soft tissue, the palate, anterolateral frontal sinus, and dura.
- •
Regardless of an open versus combined approach, a complete resection with negative margins should be the primary goal.
- •
The transfacial approach can be gradual and stepwise depending on the extent of the disease and often begins with a lateral rhinotomy to gain access to facial and orbital regions.
- •
Craniofacial approaches combine the traditional transfacial approaches with a bifrontal or subfrontal craniotomy to provide greater exposure to the ventral skull base.
- •
Transfacial and craniofacial approaches have been greatly refined since their initial descriptions, but now are mostly reserved for advanced lesions not amenable to endoscopic removal.
Introduction
Malignancies of the paranasal sinuses present unique challenges to physicians given their late presentation, diverse histology, and involvement of complex anatomic structures. Surgical resection with sound oncologic principles and reconstruction can restore function and prolong meaningful life. Small tumors of the anterior ventral skull base, such as T1 or T2, can often be managed solely by endoscopic resection. Larger tumors involving complex neurovascular or intraorbital structures often necessitate open transfacial or craniofacial resection. The decision to proceed with endoscopic versus open versus a combined approach should be made based on tumor location, reconstruction options, and surgeon experience. The preoperative planning, surgical steps, postoperative care, and clinical results from the literature are discussed in this article.
Introduction
Malignancies of the paranasal sinuses present unique challenges to physicians given their late presentation, diverse histology, and involvement of complex anatomic structures. Surgical resection with sound oncologic principles and reconstruction can restore function and prolong meaningful life. Small tumors of the anterior ventral skull base, such as T1 or T2, can often be managed solely by endoscopic resection. Larger tumors involving complex neurovascular or intraorbital structures often necessitate open transfacial or craniofacial resection. The decision to proceed with endoscopic versus open versus a combined approach should be made based on tumor location, reconstruction options, and surgeon experience. The preoperative planning, surgical steps, postoperative care, and clinical results from the literature are discussed in this article.
Preoperative planning
The evaluation of every patient with concerns for a sinonasal and ventral skull base malignancy should begin with a thorough clinical history, review of systems and physical examination. With careful attention made to the ocular and cranial nerve examination, the extent and spread of tumor can be predicted. Sinonasal endoscopy is performed for further tumor characterization and to exclude any underlying infection. Imaging is essential to diagnosis and preoperative planning. A combination of computed tomography (CT) and MRI is invaluable for determining the extent of tumor involvement, orbital invasion, and intracranial extension ( Fig. 1 ). Although CT is superior to MRI in evaluating bony detail (particularly the skull base), MRI is beneficial for evaluating the soft tissues, perineural and dural involvement, and intracranial extension (see Fig. 1 ). Contraindications to surgical management of ventral skull base lesions include significant gross brain invasion, bilateral invasion of the optic nerve or optic chiasm, carotid artery invasion, and distant metastasis.
A preoperative evaluation is not complete without a histologic diagnosis by the way of tissue biopsy. Biopsy can often be performed in a clinical setting, but if there is any concern that excessive bleeding may be encountered, biopsy should be performed in the operating room. Before biopsy, imaging should be obtained to exclude an encephalocele or hypervascular tumor. Once a tissue diagnosis has been made, the correct oncologic resection and possible need for multimodality therapy can be planned. Additionally, it is recommended that the patient be presented at a multidisciplinary tumor board to facilitate multimodality management planning.
The role of PET/CT with diagnosis and management of sinonasal and ventral skull base malignancies is ideal for identification of distant metastasis, rather than localization of a primary tumor. PET/CT should be obtained when there is concern for spread beyond the paranasal sinuses, especially for tumors that have a propensity for distant metastasis, such as adenoid cystic carcinoma, lymphoma, mucosal melanoma, and sinonasal undifferentiated carcinoma.
Transfacial and open craniofacial resection are indicated for any benign or malignant tumor of the anterior ventral skull base. Open approaches allow for wide, potentially en bloc resection and are ideal for tumors that involve surrounding facial soft tissue, the palate, anterolateral frontal sinus, and dural involvement lateral to the midpupillary line. An endoscopic endonasal approach can be ideal for smaller, midline tumors, and a combined approach may be beneficial. Regardless of the approach chosen, the goal should always be for complete tumor resection with negative margins while balancing optimal cosmetic and functional outcome. Additionally, the surgeon should feel comfortable with reconstruction of the ventral skull base, which often involves local flaps and free tissue transfer.
Operative setup
All of the following procedures are performed under general anesthesia with endotracheal intubation. Of note, preprocedural tracheostomies before tumor extirpation are not routinely performed unless there is extensive pharyngeal or palatal involvement or if microvascular free flap reconstruction is planned. Constant communication between the surgeon and the anesthesiologist is crucial for any operative case and should not be dismissed. The patient is rotated 180° from anesthesia equipment and both arms tucked at the patient’s side. Perioperative antibiotics, such as a third-generation cephalosporin, are administered 30 minutes before incision. If anterior craniofacial resection is planned, the patient’s head is secured on a horseshoe head holder in a neutral position. If endoscopic assistance will be used, the navigation system is registered. Temporary unilateral or bilateral tarsorrhaphies are performed, and the planned incision is marked and injected with 1% 1:100,000 lidocaine with epinephrine. The skin is then prepared in the usual sterile fashion.
Surgical technique
Transfacial Approach
The transfacial approach is ideal for low-lying tumors involving the anterior nasal cavity, inferior maxilla, and hard palate. The approach and incision can be gradual and stepwise, depending on the extent of the disease. The basic incision begins with a lateral rhinotomy and is extended to a Weber-Ferguson incision if required. The lateral rhinotomy is often combined with a medial, subtotal, or total maxillectomy depending on tumor size and location.
Lateral Rhinotomy and Midfacial Degloving
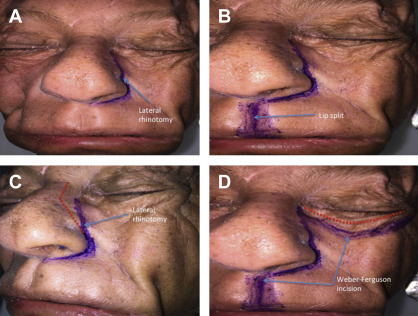
The lateral rhinotomy incision begins at the level of the medial canthus extending inferiorly along the nasal sidewall, around the nasal ala, and into the nasal cavity ( Fig. 2 ). The approach may be extended to a lynch incision for tumors that involve the medial orbit by continuing the incision superiorly to the medial eyebrow. If access to the orbital floor is needed, the rhinotomy incision is carried 90° laterally with a subciliary incision through the lower eyelid crease. A Weber-Ferguson incision and upper lip split can also be included for access to the hard palate and alveolar ridge (see Fig. 2 ). The vertical upper lip incision is made on the ipsilateral side of the philtrum for optimal cosmetic result and scar camouflage.
The incision medial to the eye is deepened and the angular vessels identified and ligated. The periosteum and soft tissue are elevated off the anterior wall of the maxilla, nasal bones, and inferior orbital rim, with careful attention being made to preserve the infraorbital nerve. The periosteum is elevated off the lamina papyracea dislocating the lacrimal sac from the lacrimal fossa. The medial canthal tendon is transected and tagged for future repair. The lacrimal duct is transected sharply without electrocautery to allow further dissection of the medial orbit. The periorbita is elevated, and the anterior and posterior ethmoidal arteries are identified and ligated. A curved osteotome can be used to make a nasal bone osteotomy through the frontal process of the maxilla then medially across the nasal dorsum to allow for medial retraction of the nasal bones and nose.
Midfacial degloving is an alternative to the lateral rhinotomy approach to the nasal cavity, ventral skull base, and infratemporal fossa. The approach involves the release of the soft tissues overlying the nasal skeleton. Its major advantage over the lateral rhinotomy is the lack of external facial incisions and visible scarring. The major limitation is limited visualization of the orbital floors, as the flap is tethered inferiorly by the inferior alveolar nerve. The procedure begins with a full transfixion incision of the columella followed by an intercartilaginous incision that extends past the piriform aperture. A circumvestibular release is completed by carrying the incision down to the periosteum laterally and then curving medially to the nasal cavity floor to meet the transfixion incision. Finally, dissection is carried in the submucoperichondrial plane over the upper lateral cartilages and to the nasal bones. At this time, attention is turned to the oral cavity in which bilateral sublabial incision is made from the first molar on one side to the first molar on the contralateral side leaving a 1-cm cuff of tissue to allow for closure. This incision is carried down to the periosteum of the maxilla, which is then elevated to the level of the inferior orbital rim, piriform aperture medially, and the pterygomaxillary suture posteriorly. This method effectively connects the intraoral component of the approach with the circumvestibular incision to elevate the soft tissue of the middle third of the face and expose essentially the entire maxillary bone bilaterally.
Medial maxillectomy
The medial maxillectomy first begins with an osteotomy made in the anterior-posterior direction in the inferior meatus, the most inferior portion of the medial maxillary sinus. The cut begins at the pyriform rim and extends posteriorly to the posterior maxillary wall. A second cut is made in the anterior-posterior direction through the medial orbit just below the fronto-ethmoidal suture line and anterior ethmoidal artery. A third cut is made through the orbital floor just medial to the infraorbital nerve and foramina, releasing the lamina papyracea and joining the second cut posteriorly. Heavy mayo scissors are then used along the previously made osteotomies and to release the posterior soft tissue attachments. A gentle rocking motion can be applied with one finger inside the nasal cavity and the other in the maxillary sinus to fracture the remaining posterior bony attachments of the palatine bone. Any remaining bony remnants can be removed with Blakesley and Takahashi forceps. Remaining ethmoid mucosa is removed to prevent mucocele formation and final margins are collected. The specimen is removed anteriorly and sent to pathology, and hemostasis is obtained.
Closure first begins with either stenting of the nasolacrimal duct or, more often, marsupialization. The medial canthal ligament is sutured back to the nasal bone with nonabsorbable suture. Any lacerations in the periorbita should be repaired with absorbable suture. The wound is copiously irrigated and closed in a 2-layer fashion.
Subtotal and total maxillectomy
A subtotal maxillectomy is an extension of the medial maxillectomy to include removal of the alveolar ridge, hard palate, or the entire maxilla if necessary. A total maxillectomy includes the orbital floor. Ohngren line, an imaginary line drawn from medial canthus to the angle of the mandible divides the maxillary sinus into infrastructural and suprastructural lesions ( Fig. 3 ). Infrastructural lesions are associated with an earlier presentation and more complete resection, whereas suprastructural lesions present at more advantaged tumor stages and are more difficult to resect carrying a poorer prognosis.
A subtotal maxillectomy begins with a lateral rhinotomy and a modified Weber-Ferguson incision as described previously. A cheek flap is elevated off the anterior maxilla, and the inferior orbital nerve is identified. The cheek flap is carried 1 cm lateral to the lateral canthus. The orbicularis oculi and periorbita are elevated off the orbital rim along the orbital floor posteriorly to the orbital apex. Medial elevation is done above the fronto-ethmoid suture line, identified superior to the anterior and posterior ethmoid arteries. At this point, the surgeon can thoroughly inspect the orbit for tumor involvement. If the tumor involves the periorbita, then an orbital dissection or possibly exenteration is indicated as described in further detail below.
Next, the lacrimal fossa, lamina, and lacrimal duct are identified, and the duct is transected and marsupialized. The attachment of the masseter to the zygoma is divided, and attention is then turned to the intraoral part of the procedure. First, an incision is made within the ipsilateral gingivobuccal sulcus. Next, another incision is made between the ipsilateral lateral incisor and canine and is carried posteriorly and just ipsilateral (2–3 mm) to the midline of the hard palate. At the junction of the hard and soft palate, the incision is turned 90° laterally to join the gingivobuccal incision around the maxillary tubercle. Next, the trimalar suture, floor of the orbital, medial orbital wall (2 mm below the fronto-ethmoid suture line), and palate are cut using a rongeur, osteotome, or high-speed cutting drill. The palate osteotomy should be made through the lateral incisor tooth socket along with preservation of the nasal septum and as much palatal mucosa as possible to aid in reconstruction. A large curved osteotome is used to free the maxilla from the pterygoid plates, and any remaining soft tissue attachments are transected with heavy mayo scissors.
Lastly, the specimen is removed en bloc and sent for final pathology testing. Brisk bleeding may be encountered, most likely from the internal maxillary artery, which can initially be controlled with packing and ligation, once the artery is identified. The cheek skin flap is lined with a split-thickness skin graft, and the cavity is packed with antibiotic impregnated gauze. At this point, a prosthesis is set in place and secured with lag screws. The posterior prosthesis can be sutured to the soft palate to aid in speech and swallowing. If the remaining defect is large, local or free tissue transfer may be required. Once again, careful attention is made to reapproximate the medial canthal tendon to the lacrimal crest, and the incision is meticulously closed in a 2-layer fashion.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


