Combined transcranial and endoscopic endonasal approaches remain useful in the treatment of ventral skull base malignancies. The extended bifrontal transbasal approach provides wide access to the anterior ventral skull base and paranasal sinuses without transfacial incisions. In more extensive lesions, the bifrontal transbasal approach can then be combined with an endoscopic endonasal approach (EEA) from below. This article reviews the indications, surgical technique, and operative nuances of combined transbasal and EEA (cranionasal) approaches for the surgical management of ventral skull base malignancies.
Key points
- •
The use of combined transcranial and endoscopic endonasal approaches or so-called cranionasal approaches to the anterior ventral skull base and paranasal sinuses remain an important option in the surgical treatment of sinonasal and ventral skull base malignancies.
- •
The modified 1-piece extended transbasal approach provides wide panoramic exposure to tumor that invades the frontal lobes, orbital roofs, and cribriform plate without using a transfacial incision or orbital bar removal.
- •
The endoscopic endonasal approach can be combined with the transbasal approach for secondary inspection from below after tumor removal from the transcranial exposure, further resection of tumor within the sinonasal cavity, and reconstruction with a vascularized pedicled nasoseptal flap, if needed.
- •
Skull base reconstruction can be performed using a simultaneous pericranial flap from above and a nasoseptal flap from below (double flap), especially when postoperative adjuvant radiation therapy is anticipated.
Introduction
Since the conception of the bifrontal craniotomy by Frazier in 1913, Derome and Tessier and colleagues popularized the transbasal approach to the anterior ventral skull base. Numerous modifications of the transbasal approach have been developed, each adding varying degrees of bone removal of the supraorbital bar, orbital roof and wall, lateral orbital rims, nasal bones, and paranasal sinuses (frontal, ethmoid, and sphenoid sinuses). In 1988, Raveh and Vuillemin, described the subcranial approach for the removal of fronto-orbital and anteroposterior skull base tumors, which entailed nasal and orbital osteotomies and minimal frontal lobe retraction. In 1991, Kawakami and colleagues, presented the extensive transbasal approach, performing en bloc bilateral orbital roof and frontal sinus osteotomy. This allowed for access to tumors extending laterally into the anterior cranial fossa. Sekhar and colleagues discussed the extended frontal approach in 1992, which added an orbitofrontal or orbitofrontoethmoidal osteotomy. These transbasal modifications have allowed for increased posterior and inferior surgical view toward the clivus with less frontal lobe retraction. These midline subfrontal approaches to the anterior ventral skull base and paranasal sinuses remain critical in the treatment of anterior ventral skull base and sinonasal malignancies.
In the past decade the role of the pure endoscopic endonasal approach (EEA) has gained increasing popularity, driven by continuous advances in endoscopic instrumentation, intraoperative image guidance, and surgical technique. Resections with negative margins via a purely EEA have been successfully performed for tumors confined to the nasal cavity and paranasal sinuses with radiologic evidence of normal cribriform plate and upper ethmoid sinuses.
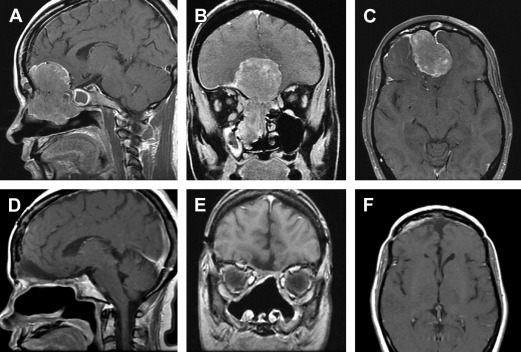
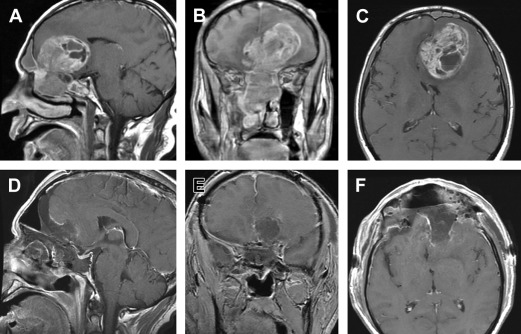
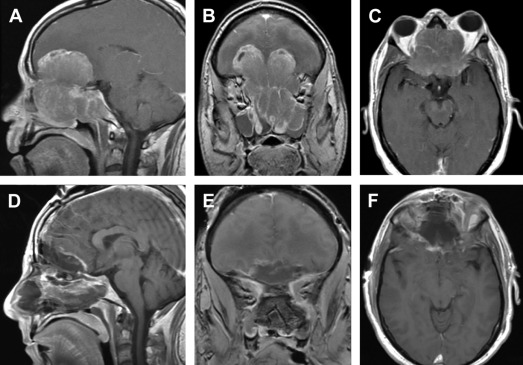
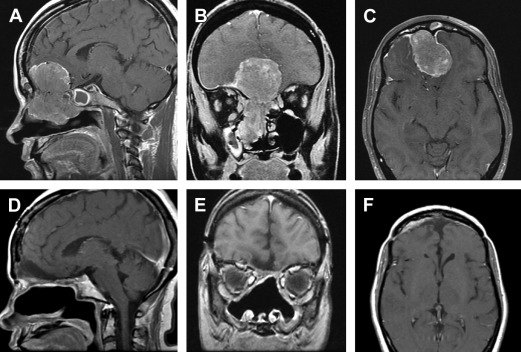
However, limitations of the pure EEA arise when there is significant intracranial extension or considerable extension beyond the lamina papyracea. For instance, when en bloc resection of the tumor including the cribriform plate is necessary, it may be best accomplished with an anterior craniotomy. Thus, open approaches remain an integral component in our surgical armamentarium. In the bifrontal transbasal approach, one can access the cribriform plate and perform a total ethmoidectomy, sphenoidotomy, and midline clivectomy down to the craniovertebral junction. Traditionally, the transbasal approach was often combined with a transfacial approach (combined craniofacial approaches) to treat a vast majority of sinonasal skull base malignancies. This combined approach allowed for access to tumors residing beneath the orbit in the superolateral aspect of the maxillary sinus, where the bifrontal approach alone was restricted from. Although the transfacial approach provides ample exposure for complete tumor removal, it often involved rather invasive techniques, including extensive facial incisions, facial disassembly, lateral rhinotomy, midfacial degloving, and/or facial osteotomies, leaving displeasing cosmetic results. Infectious complications or inadequate healing may lead to malunion of bones or loss of grafts, resulting in unsightly scars and disfigurement. Additionally, compared with craniofacial resection, transnasal endoscopic resection of anterior ventral skull base tumors has been demonstrated to be associated with decreased hospital and intensive care unit (ICU) stay, decreased estimated blood loss, and faster recovery. Subsequently, the EEA has become a more favorable adjunct (endoscopic-assisted craniofacial approaches or cranionasal approaches) due to its superior panoramic visualization, illumination, and avoidance of transfacial skin incisions. In this article, we discuss the role of combined transcranial and EEA approaches (combined cranionasal approach) in the surgical management of ventral skull base malignancies ( Figs. 1–3 ).
Introduction
Since the conception of the bifrontal craniotomy by Frazier in 1913, Derome and Tessier and colleagues popularized the transbasal approach to the anterior ventral skull base. Numerous modifications of the transbasal approach have been developed, each adding varying degrees of bone removal of the supraorbital bar, orbital roof and wall, lateral orbital rims, nasal bones, and paranasal sinuses (frontal, ethmoid, and sphenoid sinuses). In 1988, Raveh and Vuillemin, described the subcranial approach for the removal of fronto-orbital and anteroposterior skull base tumors, which entailed nasal and orbital osteotomies and minimal frontal lobe retraction. In 1991, Kawakami and colleagues, presented the extensive transbasal approach, performing en bloc bilateral orbital roof and frontal sinus osteotomy. This allowed for access to tumors extending laterally into the anterior cranial fossa. Sekhar and colleagues discussed the extended frontal approach in 1992, which added an orbitofrontal or orbitofrontoethmoidal osteotomy. These transbasal modifications have allowed for increased posterior and inferior surgical view toward the clivus with less frontal lobe retraction. These midline subfrontal approaches to the anterior ventral skull base and paranasal sinuses remain critical in the treatment of anterior ventral skull base and sinonasal malignancies.
In the past decade the role of the pure endoscopic endonasal approach (EEA) has gained increasing popularity, driven by continuous advances in endoscopic instrumentation, intraoperative image guidance, and surgical technique. Resections with negative margins via a purely EEA have been successfully performed for tumors confined to the nasal cavity and paranasal sinuses with radiologic evidence of normal cribriform plate and upper ethmoid sinuses.
However, limitations of the pure EEA arise when there is significant intracranial extension or considerable extension beyond the lamina papyracea. For instance, when en bloc resection of the tumor including the cribriform plate is necessary, it may be best accomplished with an anterior craniotomy. Thus, open approaches remain an integral component in our surgical armamentarium. In the bifrontal transbasal approach, one can access the cribriform plate and perform a total ethmoidectomy, sphenoidotomy, and midline clivectomy down to the craniovertebral junction. Traditionally, the transbasal approach was often combined with a transfacial approach (combined craniofacial approaches) to treat a vast majority of sinonasal skull base malignancies. This combined approach allowed for access to tumors residing beneath the orbit in the superolateral aspect of the maxillary sinus, where the bifrontal approach alone was restricted from. Although the transfacial approach provides ample exposure for complete tumor removal, it often involved rather invasive techniques, including extensive facial incisions, facial disassembly, lateral rhinotomy, midfacial degloving, and/or facial osteotomies, leaving displeasing cosmetic results. Infectious complications or inadequate healing may lead to malunion of bones or loss of grafts, resulting in unsightly scars and disfigurement. Additionally, compared with craniofacial resection, transnasal endoscopic resection of anterior ventral skull base tumors has been demonstrated to be associated with decreased hospital and intensive care unit (ICU) stay, decreased estimated blood loss, and faster recovery. Subsequently, the EEA has become a more favorable adjunct (endoscopic-assisted craniofacial approaches or cranionasal approaches) due to its superior panoramic visualization, illumination, and avoidance of transfacial skin incisions. In this article, we discuss the role of combined transcranial and EEA approaches (combined cranionasal approach) in the surgical management of ventral skull base malignancies ( Figs. 1–3 ).
Combined transbasal and endoscopic endonasal approach
With the advent of skull base endoscopy, the EEA and its extended variations have changed the paradigm by which ventral skull base lesions are treated. In recent years, the surgical landscape of endoscopic skull base surgery has evolved as this anatomic territory became better understood. By taking advantage of the natural anatomic corridors, such as the transnasal, transsphenoidal, transethmoidal, and transmaxillary corridors, structures from the clivus to the Meckel cave to the pterygopalatine fossa are now accessible without external incisions. The versatility of EEA has increased minimally invasive surgical access to the ventral skull base dramatically. In our practice, most sinonasal and anterior ventral skull base malignancies are treated with a purely endoscopic endonasal transcribriform approach. However, if one is to choose a transbasal approach from above, this can be used in conjunction with a complementary EEA from below to treat large lesions involving multiple anatomic compartments (see Figs. 1–3 ). The transbasal approach provides exposure from the third ventricle to the base of the clivus with relatively limited frontal lobe retraction. In the past, such lesions were traditionally treated with extended transbasal approaches combined with open transfacial approaches involving facial skin incisions and facial osteotomies. Because the extended EEAs provide wide panoramic access and visualization to the ventral skull base in the sagittal and coronal planes, the traditional transfacial approaches have gradually fallen out of favor and use. From a transcranial approach, the anterior nasal cavity and superolateral regions of the maxillary sinus are difficult to visualize (blind spots). However, the EEA allows excellent visualization and access to the entire paranasal sinuses, including these blind spots, particularly with angled endoscopy. Through this synergistic combined approach, the surgeon can work from above to control and remove intracranial tumor, and also from “below” to control tumor in the sinonasal cavity. A combined approach also can be used from a reconstruction strategy because the EEA can provide an additional vascularized pedicled nasoseptal flap, if needed. This may be useful in cases in which the pericranial flap is compromised from prior craniotomies, or needs to be supplemented from below. Alternatively, the pericranial flap can serve as the primary source of vascularized reconstruction if the nasoseptal flap is compromised or invaded by a sinonasal malignancy.
Surgical considerations: approach selection
Several considerations go into deciding on an appropriate operative approach for sinonasal skull base malignancies, such as anatomic location, degree of tumor extension in the sagittal and coronal plane, degree of intracranial involvement, vascular or cranial nerve encasement, brainstem compression, tumor consistency, history of prior surgical approach, surgeon’s preference, and level of experience. When selecting the optimal approach based on anatomic location, consideration should be taken to choose an approach that not only has the most direct route to the tumor, but also optimizes exposure and visualization of the tumor interface with critical structures so as to avoid neurologic damage and surrounding vital structures, such as the orbit, optic nerves, carotid arteries, cavernous sinus, and frontal lobes.
History of prior surgery is important and may affect the surgical approach selected. Postoperative changes, such as altered anatomy, loss of landmarks, edema, and fibrosis may make definitive surgical resection and accurate evaluation of the extent of disease more challenging. Individual surgeons may have different thresholds as to when an open approach should be warranted or added to their endoscopic resection. Hanna and colleagues held a low threshold for adding a craniotomy to the EEA (combined cranionasal approach) if there was dural involvement or transdural spread and/or invasion of the skull base, whereas Nicolai and colleagues continued EEA for selected patients with skull base invasion and focal dural infiltration. The surgeon must also be aware that some cases with significant tumor extension into multiple compartments may require a combination of more than 1 approach to adequately remove the tumor. Typically, the use of EEA exclusively is contraindicated when there is involvement of skin and subcutaneous tissue, nasolacrimal sac, anterior table of frontal sinus, carotid artery, and extensive dural and brain parenchymal involvement. In these instances, the addition of a transfacial or transcranial approach is warranted for optimal resection of the malignancy. Thus, it is important to maintain the open approaches in the surgical repertoire for various indications.
Preoperative considerations
Preoperative MRI is essential to assess the tumor and to check for intracranial extension. Computed tomography angiography (CTA) is useful to assess the anatomy of the anterior and posterior arterial circulation relative to the tumor, to rule out any vascular encasement, and to study the neighboring venous anatomy, including the cavernous sinus, petrosal sinuses, and any large draining veins. CTA is preferred over magnetic resonance angiography, as it also shows the bony anatomy of the skull base in high resolution. Digital subtraction angiography is reserved for complicated vascular anatomy not adequately assessed on CTA or for balloon test occlusion in cases of significant arterial encasement. In patients with sellar and suprasellar tumor involvement, baseline pituitary function should be assessed with appropriate endocrine testing. It is important to obtain formal baseline neuro-ophthalmological testing for patients who present with visual disturbances due to optic nerve and/or orbital involvement.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


