Key points
- •
Due to the close proximity of critical structures, initial evaluation should include assessment of visual complaints (eg, diplopia) and extraocular movements, unilateral middle ear effusion suggesting Eustachian tube obstruction, as well as thorough endoscopic examination of the nasal cavity. Additionally, evaluation of the neck should be performed to rule out any lymphadenopathy.
- •
Orbital involvement may be suspected from history, physical examination, and imaging. Nonetheless, the gold standard for determining orbital involvement, is intraoperative frozen section and permanent pathology, as it may be difficult to ascertain whether imaging is showing periorbital edema, orbital content displacement, or frank invasion.
- •
In lesions involving the cavernous sinus, avoidance of internal carotid artery resection lowers the risk of cerebrovascular accident and hemorrhage, although resection is sometimes necessary with extensive tumor involvement. In cases in which the internal carotid artery must be sacrificed, revascularization procedures should be considered.
| CN | Cranial Nerve |
| CT | Computed Tomography |
| ITF | Infratemporal Fossa |
| MR | Magnetic Resonance |
| PPF | Pterygopalatine Fossa |
Introduction
The therapeutic repertoire for management of sinonasal and ventral skull base malignancies has expanded significantly in recent decades. A variety of considerations are responsible for these advances, including innovative surgical and optical technologies, increased understanding of endoscopic endonasal anatomy, and the increasingly targeted nature of nonsurgical therapies. As a result, the management of ventral skull base malignancies has evolved from extensive resection with potentially devastating and disfiguring sequelae to a largely minimally invasive endeavor. Advances in the care of patients with these malignancies have facilitated the formation of interdisciplinary skull base teams, with otolaryngologists, neurosurgeons, radiation oncologists, and medical oncologists all playing a critical role. Despite these developments, advanced lesions still present significant clinical challenges due to the close proximity of critical structures. This overview presents an up-to-date survey of novel therapies and surgical approaches that may be of use in the challenging clinical scenarios typically associated with sinonasal and ventral skull base malignancies.
Introduction
The therapeutic repertoire for management of sinonasal and ventral skull base malignancies has expanded significantly in recent decades. A variety of considerations are responsible for these advances, including innovative surgical and optical technologies, increased understanding of endoscopic endonasal anatomy, and the increasingly targeted nature of nonsurgical therapies. As a result, the management of ventral skull base malignancies has evolved from extensive resection with potentially devastating and disfiguring sequelae to a largely minimally invasive endeavor. Advances in the care of patients with these malignancies have facilitated the formation of interdisciplinary skull base teams, with otolaryngologists, neurosurgeons, radiation oncologists, and medical oncologists all playing a critical role. Despite these developments, advanced lesions still present significant clinical challenges due to the close proximity of critical structures. This overview presents an up-to-date survey of novel therapies and surgical approaches that may be of use in the challenging clinical scenarios typically associated with sinonasal and ventral skull base malignancies.
Diagnosis
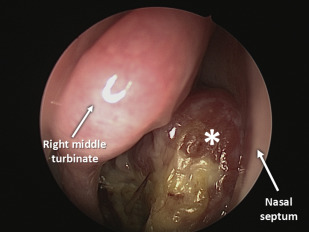
Initial diagnosis of sinonasal and ventral skull base malignancies can be difficult, as presenting signs and symptoms may be nonspecific. Patients often present with nasal congestion, facial pain, facial discomfort, or rhinorrhea indistinguishable from chronic rhinosinusitis. Deciding which patients warrant more rigorous diagnostic workup can be a difficult undertaking. Additional aspects of the history that may support obtaining further workup include unilateral symptoms of acute onset, as well as complaints associated with cranial neuropathies. Due to the close proximity of critical structures, initial evaluation should include assessment of visual complaints (eg, diplopia) and extraocular movements, unilateral middle ear effusion suggesting Eustachian tube obstruction, as well as thorough endoscopic examination of the nasal cavity ( Fig. 1 ). Additionally, evaluation of the neck should be performed to rule out lymphadenopathy. Although uncommon with most sinonasal and ventral skull base malignancies, lymph node metastasis may be present with nasal cavity tumors and nasopharyngeal carcinoma; in fact, this is the most common presentation among patients with the latter.
In addition to a thorough examination that includes endoscopic evaluation, patients with worrisome clinical signs and symptoms, particularly those with paresthesias, diplopia, unilateral symptoms, and cranial neuropathies, should undergo imaging evaluation. Computed tomography (CT) scans with 2- to 4-mm cuts are the “workhorse” imaging modality for initial evaluation of sinonasal pathologies, as this provides detailed information regarding bone, ventral skull base, and orbital involvement ( Fig. 2 A ). Magnetic resonance (MR) imaging further delineates soft tissue involvement, and is helpful in assessing the extent of dural invasion in ventral skull base malignancies ( Fig. 2 B–D); the use of postcontrast gadolinium-enhanced MR is critical (see Fig. 2 B–D). These modalities are also used for intraoperative neuronavigation purposes in patients who are surgical candidates. Although conventional MR and CT provide valuable information and can allow the operating surgeon to formulate a detailed surgical plan, evaluation with angiography may also be necessary depending on the extent of the lesion and concern for involvement of vascular structures. CT ( Fig. 3 ) and MR angiography are noninvasive alternatives to conventional angiography, and can be helpful for evaluating the integrity of major vessels. For example, these modalities can usually determine the extent of tumor involvement around the internal carotid artery, helping determine whether a purely endoscopic approach is appropriate or whether a combined approach is warranted. Conventional angiography can also provide additional information if there is significant tumor encasement, particularly with regard to the extent of collateral circulation. PET and PET-CT imaging is also valuable for evaluating regional and distal metastases ( Figs. 4 and 5 ).
In addition to obtaining appropriate imaging, there are several other critical aspects of initial and preoperative evaluation. For sinonasal and ventral skull base lesions involving the sella, many surgeons advocate obtaining baseline levels of hormones produced by the pituitary gland, and close collaboration with endocrinology colleagues. Just as importantly, there should be comprehensive discussion of obtaining a biopsy when feasible. Biopsy of undiagnosed nasal lesions in the office without first obtaining imaging is discouraged in most situations, as imaging can provide information about intracranial connection and the vascular nature of a lesion. Some lesions with the potential to be vascular in origin are more safely biopsied in the operating room.
Anatomic considerations in endoscopic approaches
There are numerous anatomic variants that should be noted on preoperative imaging. Although these are many of the same structures essential for success in endoscopic sinus surgery, there are additional considerations in more advanced lesions involving the sinonasal and ventral skull base. A comprehensive review of individual structures relevant to specific lesions is discussed (see Satish Govindaraj and colleagues article, “ Evaluation of Patients with Sinonasal and Ventral Skull Base Malignancies ,” and Thomas J. Willson and colleagues article, “ Anatomic Consideration in Sinonasal and Ventral Skull Base Malignancy Surgery ,” and specific chapters focusing on pterygopalatine, infratemporal, clival, and orbital lesions).
The depth of the olfactory fossa should be noted on preoperative CT. The Keros classification organizes this value into 3 different types: a type 1 Keros lamina lateralis (1–3 mm) is relatively “safe” compared with a type 3 lamina (8–16 mm), as the latter is more easily disrupted intraoperatively.
There are several relevant structures associated with the sphenoid sinus. The presence of an Onodi cell may be important, as these may encompass the optic nerve. In general, knowing the location of the optic nerve and internal carotid artery is important, as there can be bony dehiscence over these structures in a significant proportion of patients. Deviation of the sphenoid intersinus septum should be noted as well, particularly in relation to the internal carotid artery. Finally, involvement of the cavernous sinus and associated structures should be noted.
Several structures should be evaluated in preoperative imaging to prevent orbital complications. Failure to recognize variants in the medial orbital wall can result in injury to the extraocular muscles. Furthermore, the preoperative CT should be evaluated for the uncinate attachment to avoid violation of the lamina papyracea. Other key structures of which to note the location are the ethmoidal vessels; in particular, damage to an anterior ethmoid artery located within the ethmoid sinus can cause this structure to retract into the orbit, causing a retro-orbital hematoma. If this artery needs to be divided (as is typically performed in endoscopic anterior ventral skull base resections), it should be done closer to the cribriform plate to prevent this complication. With regard to tumor involvement of orbital structures, CT can help delineate involvement of orbital bone, superior orbital fissure, inferior orbital fissure, and optic foramen. Expansion of these foramina suggest tumor involvement. As detailed previously, MR can further evaluate soft tissue involvement, including neural involvement; importantly, secretions located in the lacrimal sac can sometimes be distinguished from tumor invasion. In a significant proportion of cases, however, it may be difficult even for MR imaging to distinguish edema from invasion of soft tissues.
Several structures related to the frontal sinus are readily identified on preoperative imaging. The operating surgeon should be cognizant of suprabullar cells, frontal cells, and the extent of an agger nasi cell. When present, the agger nasi cell is located anteriorly, with suprabullar cells and the fovea ethmoidalis posteriorly. A discussion of extended frontal sinusotomy procedures, such as a Draf III, is beyond the scope of this analysis; however, performance of these may need to be considered depending on the location and extent of the lesion. With regard to an endoscopic anterior ventral skull base resection, the posterior table of the frontal sinus is the anterosuperior limit whereas the planum sphenoidale is the posteroinferior limit of tumor resection. These can both be identified on preoperative imaging.
A variety of lesions have been noted to involve the clivus, the bony structure separating the nasopharynx and the posterior cranial fossa. Clival anatomy can be evaluated on fine cut CT. The upper portion of the clivus is behind the sphenoid sinus and sellar structures, although inferiorly the clivus is behind the posterior sphenoid body and basioocciput. Most clival lesions originate at the midline and are chordomas, whereas paramedian lesions should raise the index of suspicion for other etiologies such as chondrosarcomas. CT can help evaluate the impact on surrounding structures; lesions that elevate the pituitary gland are likely clival or nasopharyngeal in origin, rather than being an invasive pituitary lesion with inferior extension. Considerations related to open and combined approaches are comprehensively detailed (see Elizabeth Perkins and colleagues article, “ Transfacial and Craniofacial Approaches for Resection of Sinonasal and Ventral Skull Base Malignancies ,” and James K. Liu and colleagues article, “ Combined Endoscopic and Open Approaches in the Management of Sinonasal and Ventral Skull Base Malignancies ,” in this issue).
Outcomes
Until recently, craniofacial resection and other open techniques were predominantly used in the management of sinonasal and ventral skull base malignancies. With the shift toward endoscopic endonasal and combined approaches in a significant proportion of cases, questions have arisen regarding the efficacy of such minimally invasive approaches. One theoretic concern with endoscopic approaches stems from the traditional oncologic principle of en bloc resection, which is not followed with endoscopic techniques. In one retrospective analysis comparing open and closed approaches, transnasal endoscopic skull base resection was noted to be associated with a shorter hospital stay and lower recurrence rate; no differences were noted in survival or metastasis rates. A later and larger study by the same group had similar findings. Another intra-institutional series noted that there was not an increased risk of positive margins with the use of endoscopic approaches. The literature on this topic is almost entirely composed of small single-institution series, and further larger-scale analysis may be needed. Nonetheless, initial investigations into this question do not reveal any consensus regarding decreased efficacy by use of minimally invasive endoscopic techniques. These findings should still be viewed carefully, as selection bias typically caused smaller ventral skull base malignancies to be generally treated with the endoscopic approach, and much larger lesions with inherently poorer prognosis to be treated with the open approaches.
Malignancies involving the sinonasal and ventral skull base are typically discovered at advanced stages, thus harboring a poor prognosis. There are numerous specific staging systems based on histology, and the American Joint Committee on Cancer (AJCC) also offers a staging system for all sinonasal cancers. Going by the AJCC staging classification, 5-year survival drops from 63% for stage I disease down to 35% for stage IV malignancies. These figures may vary widely by specific structures and pathology encountered. In general, squamous cell carcinoma is the most common histology encountered among sinonasal and ventral skull base malignancies. The 5-year disease-specific survival is generally highest for nasal cavity tumors when compared to other paranasal sinus sites. Further staging and specific figures for outcomes and survival rates are discussed in greater detail (see Dipan D. Desai and colleagues article, “ Staging of Sinonasal and Ventral Skull Base Malignancies ,” and Rami Abdou and Soly Baredes’s article, “ Population-Based Results in the Management of Sinonasal and Ventral Skull Base Malignancies ,” in this issue).
Endoscopic endonasal resection
Surgical nuances vary based on training, experience, surgeon preference (both neurosurgeon and otolaryngologist), as well as the specific location of a lesion. There are, however, several general principles that should be well understood by practitioners involved in these surgical procedures. Performing a complete endoscopic resection of a ventral skull base lesion near the cribriform region (anterior skull base lesion) involves resection of the cribriform plates, any involved dura, and olfactory bulbs. The specific structures involved with a malignancy guide the extent of further resection.
There are many variations based on surgical preferences, and the steps listed later in this article simply represent the techniques used at our own institutions. Many of these steps are discussed in further detail in other articles in this issue and are only briefly described here. After appropriate preoperative surgical planning, the intranasal component of a lesion is debulked with powered instrumentation. Ideally, the nasal septum and lateral nasal wall structures are visualized all the way posteriorly to the choanae before progressing further. Care should be taken to preserve the nasal septal mucosa during cases in which a nasoseptal flap may be used. However, it is preferable to use the nasoseptal flap on the unaffected side to prevent the possibility of repairing a created ventral skull base defect with a flap invaded by malignant cells. Bilateral total ethmoidectomies, maxillary antrostomies, followed by an extended sphenoid sinusotomy are performed. Care is taken to avoid damage to the nasoseptal flap pedicle. Identification of the sphenopalatine foramen area is an important surgical step. In cases in which a pedicled nasoseptal flap is used, the sphenopalatine artery is cauterized only on the side contralateral to the flap. At this point we also identify critical structures adjacent to the sphenoid sinus, including the optic nerve (cranial nerve II) and the internal carotid arteries.
When necessary, a Draf III frontal sinusotomy is performed to further expand access in lesions abutting the frontal sinuses. If the lesion involves the ethmoid sinuses and medial maxilla, an endoscopic modified medial maxillectomy is typically performed. More detailed steps to remove the crista galli, resect the dural margins, and to address other ventral skull base structures are described (see Ghassan Alokby and Roy R. Casiano’s article, “ Endoscopic Resection of Sinonasal and Ventral Skull Base Malignancies ,” in this issue).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


