Key points
- •
The surgical approach should be sufficiently wide to allow the limits of dissection to be visualized and accessed easily with a 0° endoscope and straight instruments.
- •
Following fixed anatomic landmarks and finding normal boundaries are 2 principles that ensure safe surgery and complete resection in distorted anatomy.
- •
Rather than avoiding the internal carotid artery for fear of causing injury, it should be sought out and identified to ensure its safety and guide surgery.
- •
The junction of the vidian nerve and cartilaginous eustachian tube lies just anterior to the anterior genu of the petrous internal carotid artery and is an excellent surgical guide.
- •
The most common postoperative comorbidities are ipsilateral palate numbness, eustachian tube dysfunction (rather than effusion), and trismus.
Introduction
The pterygopalatine fossa (PPF) and infratemporal fossa (ITF) house complex and densely packed neurovascular anatomy. Surgery in this area is made possible by improved anatomic understanding of the complex ventral skull base anatomy, advances in endoscopic instrumentation, and improved ventral skull base reconstruction strategies.
The transition from traditional craniofacial to endoscopic resections of sinonasal and ventral skull base malignancies initially brought on concerns about the appropriateness of the procedure. There was speculation that the lack of en bloc tumor resection in an endoscopic approach may compromise oncologic results. However, many clinicians are of the opinion that an en bloc resection of tumors in locations such as the skull base is rarely possible regardless of the approach used. The goal is always complete resection with negative margins regardless of technique. The endoscopic approach offers several additional advantages, including a shorter operation time, less morbidity, and a shorter hospital stay. In addition, complication rates have been shown to be lower and the reduction of quality of life likely less than in open resections.
Introduction
The pterygopalatine fossa (PPF) and infratemporal fossa (ITF) house complex and densely packed neurovascular anatomy. Surgery in this area is made possible by improved anatomic understanding of the complex ventral skull base anatomy, advances in endoscopic instrumentation, and improved ventral skull base reconstruction strategies.
The transition from traditional craniofacial to endoscopic resections of sinonasal and ventral skull base malignancies initially brought on concerns about the appropriateness of the procedure. There was speculation that the lack of en bloc tumor resection in an endoscopic approach may compromise oncologic results. However, many clinicians are of the opinion that an en bloc resection of tumors in locations such as the skull base is rarely possible regardless of the approach used. The goal is always complete resection with negative margins regardless of technique. The endoscopic approach offers several additional advantages, including a shorter operation time, less morbidity, and a shorter hospital stay. In addition, complication rates have been shown to be lower and the reduction of quality of life likely less than in open resections.
Preoperative planning
If a portion of the tumor is accessible in the nasal or paranasal cavity, a tissue biopsy can be taken either in the office or in the operating room to gain further information as to the origin of the disorder for the purposes of treatment planning. A lesion extending anterior to the head of the middle turbinate that is without the clear appearance of a vascular neoplasm can safely be biopsied in a clinic setting. A bleeding tumor edge in the anterior nasal cavity can readily be managed with topical vasoconstriction and bipolar electrocautery with minimal discomfort to the patient. A problem posterior to this becomes more cumbersome and difficult for the patient to tolerate. However, tumors in the PPF or ITF often cannot be reached for biopsy without a surgical approach identical to that used for the endoscopic resection. In this scenario, imaging characteristics, location, involved structures, and tumor behavior are used to determine the most likely disorder, on which surgical planning is based. It is important also to prepare for any alterations to the plan that could occur if intraoperative diagnosis is different than expected. A metastatic work-up should also be completed before proceeding to the operating theater with either combined computed tomography (CT) and MRI or fluorodeoxyglucose PET.
Preoperative CT imaging for lesions of the PPF and ITF is useful to assess the surrounding bony anatomy, expansion versus erosion of the involved bone, and widening of adjacent foramina. T1 postcontrast MRI with fat suppression removes the fat signal of the ITF and the marrow of the bone of the skull base, and is vital for evaluating tumor margins, surrounding soft tissue detail, any tumor extension into the orbit, or involvement of adjacent nerves or dura. V2 should be followed from the roof of the maxillary sinus through the foramen rotundum, and V3 through the foramen ovale. Perineural spread associated with the vidian nerve is common, so it should be considered preoperatively as well. Particular attention should also be paid to perineural involvement in the cavernous sinus and the descending palatine nerve, because either of these could alter management. Involvement of the descending palatine nerve may indicate a need for some degree of hard palate resection. Any tumor extension through the inferior orbital fissure or intracranially must be noted as well. Direct extension through the middle cranial fossa will be apparent, so it is subtler dural enhancement, particularly adjacent to foramina, that is important to detect. Research has shown that 1 mm and greater than or equal to 2 mm of dural thickening correlate with a positive predictive value of dural invasion of 46.7% and 100%, respectively. Tumor positioned laterally to the internal carotid artery (ICA) at its carotid foramen precludes a strictly endoscopic approach. An open approach, whether combined, staged, or on its own, is required to access this area. A checklist of important preoperative imaging evaluation steps is shown in Box 1 .
CT
- •
Fine cut, bony windows, 3 view
- ○
Expansion versus erosion of bone
- ○
Widening of foramen rotundum and ovale
- ○
Adjacent normal bony anatomy
- ○
Involvement of hard palate
- ○
MRI
- •
T1, postgadolinium, fat suppression
- ○
Margins of tumor
- ○
Surrounding normal soft tissue
- ○
Orbital extension
- ▪
Periorbita
- ▪
Inferior orbital fissure
- ▪
- ○
Intracranial extension
- ▪
Direct through middle cranial fossa
- ▪
Dural thickening or enhancement
- ▪
Attention to foramen rotundum and ovale
- ▪
- ○
Perineural spread
- ▪
V2
- ▪
V3
- ▪
Vidian nerve
- ▪
Descending palatine nerve
- ▪
- ○
ICA
- ▪
Intact flow
- ▪
Tumor lateral to carotid foramen
- ▪
- ○
Parapharyngeal disease
- ○
Inferior soft tissue extent
- ○
These imaging studies should be compatible with and used for image guidance during the procedure. Image guidance is a useful surgical adjunct to help surgeons confirm the location of vital structures when local anatomy is altered by tumor distortion or invasion and to verify the completeness of resection. However, it is simply a tool and does not replace the surgeon’s knowledge of the local anatomy, and should have limited influence on the previously planned surgical resection.
Access to PPF and ITF malignancies should be decided preoperatively based on tumor pathology and stage. For resection of malignant tumors of the PPF or ITF, adequate access should not be compromised by efforts to keep the approach conservative or by concerns for subsequent sinonasal function. The approach should be sufficiently wide to allow the limits of dissection to be visualized and accessed with 0° instruments at all times.
Surgical technique
Preparation
Immediately following intubation, the patient’s nose is packed with ten 75-mm by 12-mm (3-inch by 0.5-inch) patties soaked in a 10-mL mixture of 1% ropivacaine and 1:1000 adrenaline (5 mL each); clinicians should ensure they are in place for a minimum of 10 minutes before beginning the case so they may have a maximum topical vasoconstriction effect. The patient receives 1 g of intravenous ceftriaxone and has a Foley catheter and an arterial line placed for close monitoring. The image guidance is set up and registered to the patient with verification of accuracy. The bed should be in reverse Trendelenburg with the head elevated to 15° to decrease central venous pressure and maximize hemostasis and operative conditions. A solution of 1% ropivacaine with 1:100,000 adrenaline is injected locally, with particular attention to the root of the middle turbinate, the septum, the inferior turbinate, and the floor of the nose in this case. If the tumor burden in the nasal cavity is large enough to prevent adequate local injection in these areas, a greater palatine injection through the mouth is an effective alternative. Once the heart rate returns to a more bradycardic range, preferably under 70 beats/min, following the epinephrine effects from the local injection, the case is begun.
Lateral Access
Almost always, when addressing malignant disorders far lateral access into the ITF requires additional procedures beyond antrostomies. This requirement should be part of the surgical plan and performed outright rather than decided intraoperatively as a result of struggling with visualization and mobility. Any attempts at limited access almost certainly lead to loss of oncologic integrity in the tumor resection.
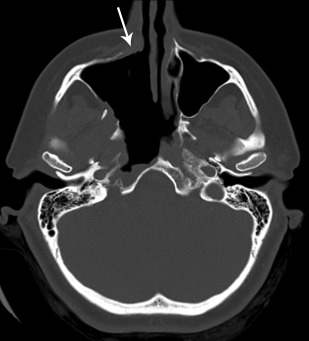
A modified medial maxillectomy is a standard part of accessing this region. However, a total rather than a modified medial maxillectomy can be used. In this case, the maxillary sinus is entered anterior to the nasolacrimal duct. If strictly lateral access is necessary, then this prelacrimal approach can remain low and the nasolacrimal duct can be cut cleanly, leaving the sac intact without the need for further reconstructive intervention ( Fig. 1 ). If superior and lateral access is necessary, disruption of the nasolacrimal apparatus may include the nasolacrimal sac, in which case an endoscopic dacryocystorhinostomy may be necessary to ensure adequate function postoperatively.
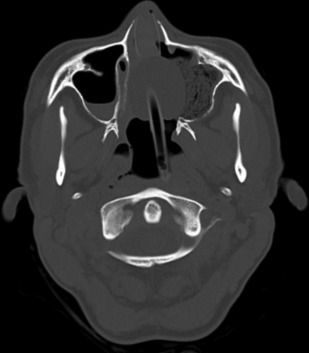
An endoscopic Denker maxillotomy is another option for lateral access. In this procedure, the entire medial buttress is removed with a drill ( Fig. 2 ). The lacrimal apparatus is disrupted similar to a total medial maxillectomy. Complications related to the procedure include injury to the anterior superior alveolar nerve; potential transection of the canine root; and, importantly, loss of lateral support of the alar cartilage to the pyriform aperture. Alar retraction can occur when performed endoscopically but is usually less severe than when done open.