33 Tracheostomy Tracheostomy is an ancient operation designed to relieve upper airway obstruction and prevent death by asphyxiation. The aim of the procedure is to create a hole in the anterior wall of the trachea to help patients breathe—bypassing any obstruction in the airway at the level of the larynx or above. The word tracheostomy is derived from Greek words trachea for windpipe and stoma for mouth. The correct term for the operation should be tracheotomy, as the Greek suffix tomo means to cut. The word tracheotomy first appeared in print in 1649, but was not commonly used until a century later when it was introduced by the German surgeon Lorenz Heister in 1718.1 The early days of tracheostomy were dogged by controversy, as many reputable physicians such as Hippocrates were opposed to the operation because of its high mortality and morbidity rate. Although there are several documentations of surgeons performing tracheotomies as lifesaving procedures from the 1500s, it was not until 1825 when Bretonneu reported a successful tracheotomy in a 5-year-old girl with diphtheria did the operation regain its popularity. Trousseau later reported 200 cases of tracheotomy for diphtheria—giving legitimacy to the operation—despite only 50 of his cases surviving the operation! In the early days, tracheostomies were often performed “high,” entering the trachea via the larynx, thereby dividing the cricoid cartilage. This led to laryngeal stenosis. A “low” tracheostomy (entering the trachea directly) was discouraged as dividing the thyroid isthmus was frowned upon. In 1923, Chevalier Jackson of Pittsburgh recognized that dividing the cricoid led to stenosis. He described placement of the tracheostomy below the first tracheal ring and the necessary meticulous aftercare. Due to his contributions, mortality from tracheostomy plummeted from 25% to 1 or 2%, and he is rightfully regarded as the father of the modern tracheostomy.2 There are really only three indications for a tracheostomy: upper airway obstruction, prolonged ventilation, and tracheobronchial toilet. As diphtheria is no longer a major scourge, fewer emergent tracheostomies are performed for upper airway obstruction. The most common causes for upper airway obstruction requiring a tracheostomy would be neoplasm of the larynx, pharynx, or other sites in the neck; head, maxillofacial, or neck trauma; and neck abscesses and neurological conditions such as bilateral vocal cord paralysis (Table 33.1). Even in these situations, intubation is often possible, and tracheostomy then becomes an elective procedure. Complex head and neck surgery often begins with an elective tracheostomy, as upper airway obstruction is anticipated postoperatively.3 In pediatric patients, the most common indications for tracheostomy are subglottic stenosis, bilateral vocal cord paralysis, congenital airway malformations, and tumors.4 Today, the most common indication for tracheostomy is for patients who require prolonged ventilation. This enables patients on mechanical ventilation to be extubated and potentially reduces the duration of an intensive care unit (ICU) admission. There is much debate as to when a tracheostomy should be performed in an intubated patient. Recent reviews have shown that whether a tracheostomy is performed early (within 10 days of intubation) or late (after 10 days of intubation) does not have an impact on the patients’ mortality in hospital or morbidity from pneumonia, beyond reducing their ICU stay.5,6 Ideally, however, because of the risk of irreversible damage to glottic mucosa from an endotracheal tube (ETT), a patient should have an elective tracheostomy if he is unlikely to be extubated within 7 days of intubation. There is an oft-quoted dictum attributed to Moser “the time to do a tracheostomy is when you first think of it” which has much truth in it. In patients in whom the cough reflex is poor, saliva is chronically aspirated with retention of mucus in the tracheobronchial tree; thus, tracheostomy allows for suctioning and tracheobronchial “toilet.” It is important to note that tracheostomy per se does not obliterate the risk of aspiration. Indeed, some patients may aspirate as a result of a tracheostomy. Therefore, aspiration is not in itself an indication for tracheostomy if a patient can cough adequately and clear their secretions. There are very few absolute contraindications to a tracheostomy when the indication for one is clear. The method of tracheostomy however depends on many factors – both anatomical and physiological—and percutaneous dilatational tracheostomy (PDT) may be contraindicated in certain circumstances7 (Table 33.2). Table 33.1 Common Causes of Upper Airway Obstruction Requiring Tracheostomy in Adults and Children
History
Indications and Contraindications
Upper Airway Obstruction
Prolonged Ventilation
Tracheobronchial Toilet
Adult | Pediatric |
• Neoplasm ○Larynx ○Thyroid ○Other neck sites • Trauma ○Head ○Maxillofacial ○Neck • Infection ○Neck abscesses ○Tetanus • Others ○Neurological ○Foreign body aspiration | • Congenital ○Subglottic stenosis ○Bilateral vocal cord paralysis ○Congenital airway malformations ○Craniofacial syndromes ○Laryngeal clefts ○Lymphovascular abnormalities • Acquired ○Subglottic stenosis ○Tumors • Laryngomalacia |
A large goiter that overlies the length of the cervical trachea, large anterior neck veins, or a “high-riding” innominate artery are reasons to avoid a PDT and perform a conventional surgical tracheostomy. Imaging, either by ultrasound or computed tomography, is often useful when there is concern about anomalous anatomy.
Coagulopathy is another perennial concern particularly if this cannot be corrected. Some surgeons would prefer PDT in this instance, as the shorter cut skin edges bleed less and undissected tissue planes allow for better tamponade. High ventilating pressures too are a concern when performing a tracheostomy, as the risk of surgical emphysema and pneumothorax is substantial. It is often advisable to delay tracheostomy in these patients until ventilating pressures are reduced.
Recent reports have shown that in many conditions previously thought to be contraindications for PDT such as obesity, burns to the neck, and emergency airway situations, PDT may be safely performed given that the necessary precautions are taken.8–10
Advantages and Disadvantages
The advantages of tracheostomy over noninvasive ventilation (e.g., a tight-fitting face mask) or an ETT are obvious. A tracheostomy reduces the anatomical dead space of the upper airway by approximately 150 mL or 50%. This reduces the work of breathing, airway resistance, peak inspiratory pressures, and intrinsic or auto positive end-expiratory pressures (PEEP) substantially.11 Improvements in ventilator synchronization and triggering, as well as better clearance of secretions may facilitate earlier weaning offthe ventilator.8 A tracheostomy tube is less irritating to the upper airway than an ETT and allows tracheostomized patients to be unsedated and more alert. It also allows patients to eat and talk—albeit with a speaking valve.
Table 33.2 Contraindications to Percutaneous Dilatational Tracheostomy
• Age less than 8 y • Gross distortion of neck anatomy ○Hematoma ○Enlarged thyroid ○Tumor ○High innominate artery • Acute airway obstruction requiring emergency airway ○Obesity with short neck obscuring landmarks ○Medically uncorrectable bleeding diatheses – PT or APTT more than 1.5 times normal range – Platelets less than 50,000 – Bleeding time more than 10 min ○PEEP more than 20 cm of water ○Soft tissue infections at the puncture site |
y, year(s); PT, prothrombin time; APTT, activated partial thromboplastin time, min, minute(s); PEEP, positive end-expiratory pressures.
There are, however, disadvantageous physiological changes in a tracheostomized patient. Airflow bypasses the nose and throat where humidification and warming normally occur. Unfiltered, dry and cold air enters the trachea directly, stimulating the proliferation of mucus-producing goblet cells and disrupting normal mucociliary clearance, hence the excessive mucus that is produced soon after a patient has a tracheostomy. This mucus can cause plugging of the lower bronchioles or form crusts that may obstruct the larger airways. Over time, the normal respiratory mucosa of the trachea undergoes squamous metaplasia.12
Evidence is divided on whether the presence of a tracheostomy tube impairs the mechanism of swallowing and therefore increases the risk of aspiration. It was initially thought that a tracheostomy tube may impair swallowing by splinting the larynx and preventing the normal upward excursion of the larynx. The presence of an inflated tracheostomy tube cuff, or a one-way valve (such as the Passy-Muir valve that allows some air to be directed into the larynx and pharynx for speech production) may also impede the stimulation of subglottic pressure receptors, thus impairing a specific segmental swallowing reflex.13,14 There is, however, no evidence that tracheostomy increases aspiration or laryngeal penetration.15
The loss of a cough reflex following tracheostomy is to be expected as patients cannot generate high intrathoracic tracheal pressures to initiate a cough. This impedes their ability to clear the secretions. When secretions are copious soon after tracheostomy, suctioning is necessary to clear these secretions. Eventually, patients develop an effective cough, and secretions lessen, making suctioning no longer necessary.
Methods
Surgical Tracheostomy
A surgical tracheostomy is performed in either an elective, urgent, or emergent manner. It is the safest way to secure an airway and is occasionally lifesaving.
Patient positioning is critical to facilitating a smooth procedure. A head support and shoulder roll allow for neck extension and good exposure of the trachea. The surgeon should palpate the surgical landmarks, for example, the sternal notch, the cricoid cartilage, and the anterior border of sternocleidomastoid muscles and mark these out. It is also advisable to feel for the carotid arteries and a high-riding innominate artery. If there is any doubt, an ultrasound scan may shed light on any anomalies.
A skin crease incision is made halfway between the cricoid cartilage and sternal notch. The length of this incision very much depends on the experience of the surgeon and the depth of subcutaneous tissue overlying the trachea. Typically, incisions are 2 to 4 cm.
Infiltration with epinephrine is advisable. In the awake patient, the use of a dental syringe with a mixture of a local anesthetic and epinephrine is best. Infiltration should proceed down to the trachea gradually. Finally, pass the needle into the tracheal lumen and infiltrate liberally while getting the patient to cough. This maneuver ensures good tracheal anesthesia.
A good surgical assistant is crucial in performing a surgical tracheostomy. Retraction of tissues during the procedure eases the surgery. Ensure that the theater staff, including the anesthetist, is prepared before commencing the operation. In particular, check that the correct tracheostomy tube is available.
Begin by making a transverse skin incision with a blade, and deepen this to the subplatysmal plane using monopolar diathermy. Lift the skin flaps for no more than 2 cm superiorly and inferiorly. In many patients, the platysma is absent in the midline and only present in the lateral-most aspect of the incision. A self-retaining retractor is then placed to hold the skin flaps apart. The superficial investing layer of deep cervical fascia is then divided in the midline and deepened to expose the strap muscles. The strap muscles can then be retracted laterally to expose the isthmus of the thyroid gland (Fig. 33.1).
Conventionally, the isthmus of thyroid gland is mobilized, clamped, divided, and transfixed—revealing the trachea beneath. However, in many patients, division and ligation of the thyroid isthmus is unnecessary if a plane can be created between the upper border of the thyroid isthmus and the cricoid cartilage. The pretracheal fascia tightly binds the thyroid gland to the trachea. This needs to be divided to reveal the cartilaginous rings of the trachea.
Once exposure is adequate and hemostasis secured, theater staff and the anesthetist should be warned that the surgeon is about to enter the trachea. In an awake patient, a further intratracheal infiltration of local anesthesia ensures that the patient does not cough when the trachea is incised. To avoid airway fires, diathermy is no longer used at this point. The patient is ventilated on low flow oxygen, and the ETT is passed inferiorly to ensure that the cuff is not inadvertently ruptured when the trachea is entered.
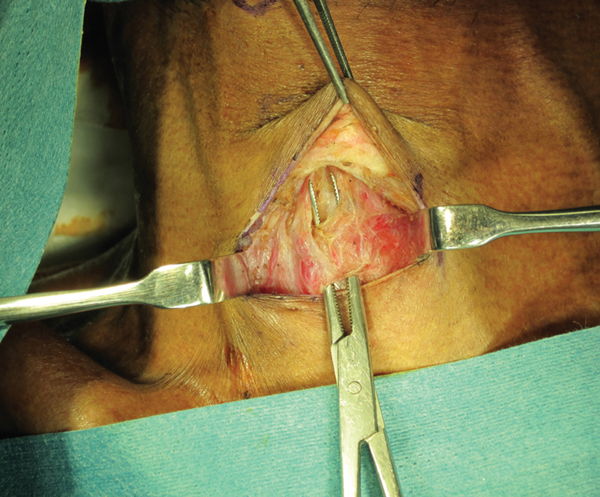
Figure 33.1 Retraction of strap muscles laterally to expose the trachea in the midline.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


