Toxic Retinopathies
F. W. Fraunfelder
Retinal toxicity is noted primarily in patients who take systemic medications rather than topical ocular medications. Exceptions, such as cystoid macular edema secondary to latanoprost, do occur but are rare. Although the liver and kidney are the most common areas to develop drug toxicity when the medication is administered systemically, a severe insult needs to occur before laboratory values become abnormal. However, in the eye, if the macula is involved, a small fraction of 1% damage may reveal a significant abnormality to the patient and to the examining physician.
The key to suspecting an adverse ocular effect is a high degree of clinical suspicion. A physician who is familiar with the signs and symptoms of an adverse ocular drug side effect will be better prepared to recognize and treat what can be easily overlooked, especially if a patient takes many systemic medications.
There are more than 30,000 prescription drugs available in the United States alone, and many more available worldwide. Over-the-counter drugs are frequently used by many patients, and these can have adverse ocular effects as well. It would be impractical to try to comprehensively cover every known retinal change reported from every type or class of drug. Therefore, presented here are representative medications known to currently be in use and have recent reports of causing retinal toxicity. These examples should serve as a frame of reference when other medications from the same class are suspected of causing a drug-induced ocular side effect or when retinal toxicity is suspected from a systemic medication.
Six medications or classes of drugs follow (chloroquine/hydroxychloroquine, isotretinoin, sildenafil, vigabatrin, tamoxifen, and phenothiazines) with the goal of familiarizing the clinician with what type of retinal toxicity to look out for, the goal of management, and guidelines for follow-up.
A good source for further inquiry into ocular side effects is the National Registry of Drug-Induced Side Effects from which the book Drug-Induced Ocular Side Effects was produced (1). The objectives of the Registry are as follows:
To establish a national center where possible drug-induced ocular side effects can be accumulated
To add to this database the spontaneous reporting data of possible drug-induced ocular side effects collected from the Food and Drug Administration and the World Health Organization
To compile the data in the world literature on reports of possible drug-induced ocular side effects in humans
To publish some of these data every 4 to 5 years in book form
To make available these data to physicians who feel they have a possible drug-induced ocular side effect
You can contact the Registry to help with a suspected drug reaction, to gain access to data in the Registry, or to report a case. When sending data, include the following: name of drug, dosage, length of time on drug, suspected reaction/s, what happened if the drug was stopped, if rechallenged, concomitant drugs, and name and address of person reporting (optional, but encouraged).
Reports can be mailed to the following:
National Registry of Drug-Induced Ocular Side Effects
Casey Eye Institute
3375 S.W. Terwilliger Blvd.
Portland, OR 97201-4197
Fax 503-494-4286
Chloroquine/Hydroxychloroquine
Although hydroxychloroquine is widely used in Britain, North America, and Australia, chloroquine is widely used in Europe, South America, and Asia. Hydroxychloroquine use has markedly increased because it has become a first-line drug for some forms of arthritis and lupus erythematosus.2 Probably all side effects seen with chloroquine can also be seen with hydroxychloroquine, but serious ones are primarily seen in overdose situations. Toxicity to the retina because of these drugs is dose related. The greatest risk for overdosing is in obese patients. The aminoquinolines are absorbed by cellular tissue, and since adipose tissue is relatively acellular, obese patients may be overdosed. A second group that is occasionally overdosed includes small, thin, elderly patients in whom the base dosage of each pill is excessive. An additional group that may show toxic changes are those with renal disease, since this is where the drug is primarily detoxified and higher than normal blood levels may occur2,3,4 (Fig. 33.1).
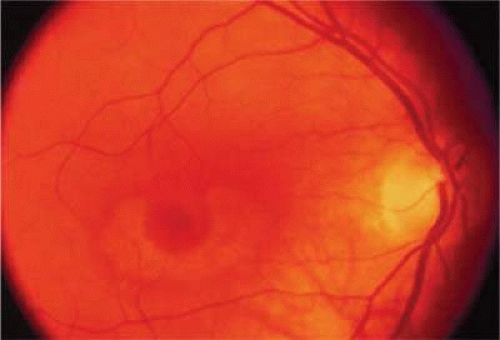 Figure 33.1. Chloroquine retinopathy. |
Toxic maculopathy is usually reversible only in its earliest phases. If these drugs have caused skin, eyelid, corneal (hydroxychloroquine), or hair changes, this may be an indicator of possible drug-induced retinopathy. Since the aminoquinolines are concentrated in pigmented tissue, macular changes have been thought to progress long after the drug is stopped. The bull’s-eye macula is not diagnostic for aminoquinoline-induced disease since a number of other entities can cause this same clinical picture. Although retinal toxicity occurs in patients taking hydroxychloroquine, the incidence is much lower than with chloroquine.
How to detect early toxic changes is still the subject of debate. Easterbrook6,7,8,9 has published extensively on chloroquine and hydroxychloroquine retinal toxicity. His current method of examination includes obtaining best corrected vision, examining the cornea with the pupil dilated with retroillumination, and performing an Amsler examination. (He has his patients test themselves every few weeks at home with an Amsler grid.) If the results of the Amsler grid examination are abnormal, a Humphrey field with the 10-2 red and white program is performed. If color vision is deficient on Ishihara testing or if there is any question of a patient’s reliability in terms of visual field assessment, fluorescein angiography is done as well. According to Easterbrook, electroretinographic and electro-oculogram studies are either too variable or are abnormal only in late signs of chloroquine retinopathy, so their usefulness is suspect. Color testing is more useful in elderly patients where coincidental age-related macular changes occur. It is also stated that early retinopathy (i.e., small paracentral relative scotomas) (Fig. 33.2) does not appear to progress, at least in the short term. Patients who present with absolute scotomas and positive fluorescein angiography should be warned that their retinopathy may progress even if the chloroquine therapy is discontinued. There are numerous instances of progression of macular and optic nerve damage, even years after these drugs are discontinued. This may not be as true for hydroxychloroquine since the progression of the maculopathy may be significantly less than with chloroquine once the drug is stopped.
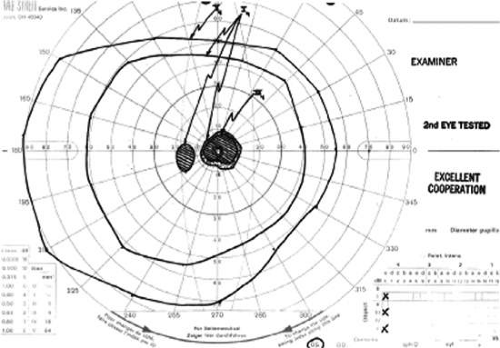 Figure 33.2. Paracentral scotoma secondary to chloroquine toxicity. |
Some patients wish to continue taking these drugs even with the visual side effects because only these drugs improve their quality of life. If reproducible abnormalities of the Amsler grids occur in this group of patients, kinetic and static perimetry are obtained. If field defects are confirmed, consultation with the rheumatologist concerning discontinuation of the drug is advised. If the patient is reluctant, one may consider halving the usual dosages and following the patient every 3 to 4 months even with relative paracentral scotomas with serial fields. If, however, there is any progression, the recommendation is to stop the drug.
Overview
Maculopathy must be bilateral and reproducible by Amsler grid and visual field testing. Transient or unilateral defects are not sufficient reasons to implicate the drug, and are not an indication to stop therapy. Color vision loss is a late change. The goal is to find early changes, such as relative scotomas substantiated by visual fields. Also suspect are patients with retinal changes, color vision loss, absolute scotoma, and decreased vision, since even if the drug is stopped, two thirds of these patients may continue to lose some vision and/or peripheral fields. Patients with early paracentral relative scotomas do not advance when the drug is discontinued.
Guidelines for Following Patients on These Agents
This is controversial. Morsman et al,10 Morand et al,2 and Levy5 question the need to screen patients on hydroxychloroquine. Spalton11 suggests every 3 years, Levy5 after 10 years, and so on. Blyth and Lane12 suggest ophthalmic examination only after the patient becomes symptomatic. We favor the approach by Easterbrook that is presented here.
Initial examination. We prefer a baseline complete eye exam. This includes visual acuity, Amsler grids, color vision, and corneal retroillumination. If abnormalities are in the Amsler grid, automated perimetry is indicated.
Follow-up examinations. Hydroxychloroquine: Ophthalmic examination, repeating above baseline studies every 12 to 18 months for patients who are taking less than 6.5 mg/kg of ideal body weight with normal kidney and/or liver function. This is in keeping with the American Academy of Ophthalmology’s recommendation for biannual eye exams in normal adults. If taking the drug for more than 6 years, or accumulative dosage of 200 g, patients should be examined at least annually. Warn patients to see you if any change in vision or changes on their home Amsler grid testing. Chloroquine: Perform same tests as above. See patients at least annually if dosage is less than 3.0 mg/kg of ideal body weight. See patients every 6 months if dosage is greater than 3.0 mg/kg body weight, or if they are short, obese, or have renal and/or liver impairment.
American Academy of Ophthalmology recommendations are pending and will be similar to what we have described.
Tests
Amsler grids appear to be the most cost-effective method of following patients. Monthly home testing is essential, especially if the patient is on higher dosages, long-term therapy, or has renal disease.
Routine visual fields are not necessary unless Amsler field defects, abnormal color vision, decreased vision, or abnormal retinal findings are detected. A baseline visual field has been advocated by some.
Retroillumination of the cornea with the slitlamp with dilated pupils looking for enhanced Hudson-Stähli line, or more commonly, whorl-like superficial corneal deposits, which, however faint, are early indicators of possible retinal toxicity in hydroxychloroquine patients.
Caution
To date, there are no data to show hydroxychloroquine toxicity worsening pre-existing macular degeneration. Common sense may make informed consent and explanation of risk/benefit ratios necessary on an individualized basis.
Isotretinoin
Ocular side effects are dose related and probably the most frequent adverse reactions associated with these drugs. Retinal changes are rare compared to reports of blepharoconjunctivitis, subjective complaints of dry eyes, and transient blurred vision. However, there are well-documented cases of decreased ability to see at night in patients after taking these agents. This may occur as early as a few weeks or after having been on the drug for 1 to 2 years. It was previously unrecognized that this may be a permanent effect. Retinal dysfunction is probably owing to the competition for binding sites between retinoic acid and retinol (vitamin A). The risk of a photo-sensitizing drug, such as isotretinoin, enhancing the effects of light on the macula and retina is unclear. Although there are cases in the Registry of retinal pigmentary changes, to date we consider this just background noise. Excessive amounts of retinoids have been implicated in papilledema secondary to pseudotumor cerebri and may suggest hypervitaminosis A.13 This is confusing, in part because other antibiotics may be used concomitantly (tetracycline, minocycline), which may also cause pseudotumor cerebri.
Recommendations for Following Patients on This Agent
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


