Toxic Anterior Segment Syndrome
Nick Mamalis
Henry F. Edelhauser
Toxic anterior segment syndrome (TASS) is an acute, sterile postoperative anterior segment inflammation following any anterior segment surgery. By definition, this entity is sterile or noninfectious. This entity was initially described as sterile postoperative endophthalmitis but in 1992, Monson et al.1 accurately termed this condition “toxic anterior segment syndrome.” In addition, cases of TASS, which are characterized by localized corneal endothelial damage have been termed “toxic endothelial cell destruction syndrome” (TECDS).2,3,4,5,6 This entity has been thoroughly discussed in a review/update paper on toxic anterior segment syndrome and its accompanying editorial.7,8
Toxic anterior segment syndrome most commonly occurs acutely following anterior segment surgery, but in rare instances can have a delayed onset. The postoperative inflammation is sterile or noninfectious and is felt to be secondary to a toxic substance of some kind that enters the anterior segment either during or immediately after anterior segment surgery causing inflammation. The most common symptoms of TASS include blurry vision. Pain is often absent from patients with TASS in distinction to postoperative infectious endophthalmitis. The hallmark of TASS is that the inflammation usually has a relatively immediate onset, certainly within 12 to 48 hours of surgery. The most common clinical findings are a diffuse corneal edema that has been described as “limbus-to-limbus” corneal edema (Fig. 6-4.1). The widespread damage of two corneal endothelial cells will lead to this diffuse edema. This pattern differs significantly from focal corneal edema, which is often seen following cataract surgery.
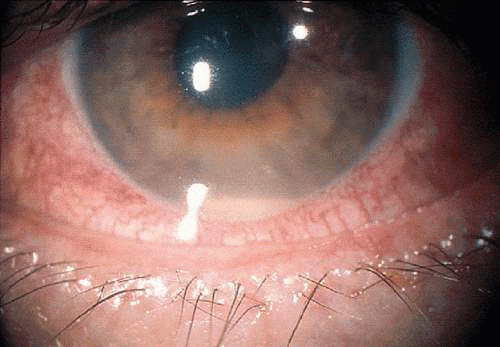 Figure 6-4.1. Diffuse “limbus-to-limbus” corneal edema. (From Review/Update—Toxic anterior segment syndrome. J Cataract Refract Surg 32, 2006, with permission.) |
A second hallmark of this entity is a marked anterior segment inflammation (Fig. 6-4.2). This is characterized by a diffuse breakdown of the blood aqueous barrier with increased inflammatory cells in the anterior chamber that may lead to hypopyon formation. In addition, fibrin may form across the pupil, iris, and surface of the intraocular lens. Lastly, this syndrome can result in damage to the iris, which can cause a permanently dilated or irregular pupil as well as possible trabecular meshwork damage leading to a difficult to control glaucoma (Fig. 6-4.3).
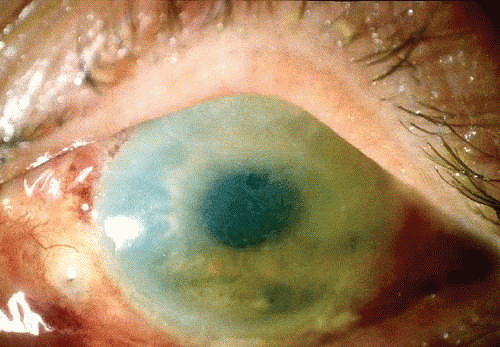 Figure 6-4.2. Anterior segment inflammation with hypopyon formation. (From Review/Update—Toxic anterior segment syndrome. J Cataract Refract Surg 32, 2006, with permission.) |
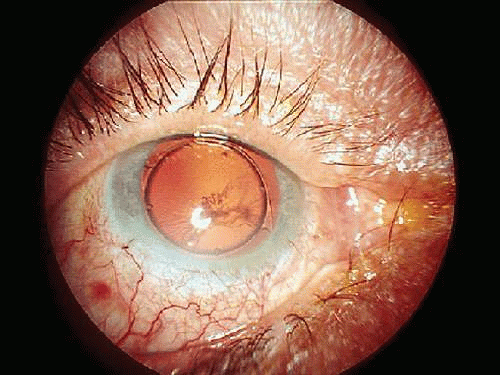 Figure 6-4.3. Dilated, atrophic iris with irregular pupil. (From Review/Update—Toxic anterior segment syndrome. J Cataract Refract Surg 32, 2006, with permission.) |
It is important to differentiate the sterile inflammation seen in TASS from an infectious postoperative endophthalmitis. One of the signs that is most helpful in differentiating these two entities is that TASS occurs acutely in most cases with signs appearing within the first 24 to 48 hours. In bacterial endophthalmitis, the typical signs do not often appear from 4 to 7 days postoperatively. The symptoms in these entities are different in that greater than 75% of patients who have an infectious endophthalmitis will often have pain. Most cases of TASS are pain free. The anterior segment inflammatory changes in both of these entities are often very similar with significant inflammation and hypopyon formation. The diffuse corneal edema seen in TASS, however, is often not noted in an infectious endophthalmitis. With any question of an infectious etiology, the anterior chamber and vitreous samples be taken for staining and culture.
Etiology of TASS
Any substance used during or immediately after cataract surgery that can obtain access to the anterior segment of the eye can cause TASS. This includes medications, anesthetics, antibiotics, and solutions that are used in general. TASS is characterized by a toxic reaction that causes damage to the anterior segment of the eye. The corneal endothelium is especially sensitive to any toxins.
The etiology of TASS is broad and may include problems with the irrigating solutions such as balanced saline solution.9,10,11,12,13 Any ophthalmic solutions that contain preservative or stabilizing agents of any kind can be toxic to the corneal endothelium and may cause TASS problems.13,14,15 Intraocular medications, such as antibiotics and anesthetics, are a potential source of TASS. Additionally, residues of ophthalmic viscosurgical devices (OVD) can cause significant postoperative inflammation.16 Lastly, it is important to remember that any enzymes or detergents that are used in the sterilization of instruments used in anterior segment surgery can leave a residue that could cause TASS.17,18,19
Intraocular Irrigating Solutions
Intraocular irrigating solutions, such as balanced saline solution (BSS), have the potential to cause problems with TASS if problems exist with the composition of the BSS with incorrect ionic composition, osmolarity, or pH.9,10,11,12,13
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


