FIGURE 26.1 The total and near-total defect of the maxilla is typically approached through a Weber-Ferguson incision (inset). The maxillectomy defect can easily be accessed through this approach.

FIGURE 26.2 The fibular free flap provides a cylindrical bone graft The peroneal artery and vein run parallel to the bone graft. The vessels can be dissected from the graft to gain length on the vascular pedicle.
The defect is then carefully analyzed. The contouring of the maxilla is created using a template fashioned to the resection specimen. The length of the fibular bone and appropriate closed osteotomies are determined based on this template.
To achieve appropriate length, the proximal periosteum is dissected to allow for the longest pedicle length possible. Using a sagittal saw, the bone is then contoured to the appropriate length (Fig. 26.3). The previously determined closed osteotomies are then performed to create the contour of the maxilla. Using 2.0 miniplates, the bone is then fashioned in place. Anteriorly, the bone is secured to the remnant maxilla. Laterally, the bone is secured to the remnant zygoma (Fig. 26.4).
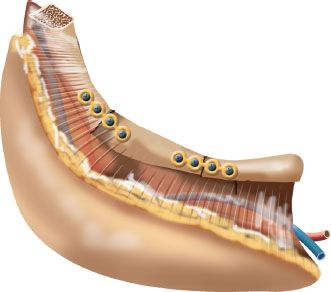
FIGURE 26.3 Multiple osteotomies can be made in the bone to provide the contour required for reconstruction of the maxilla.
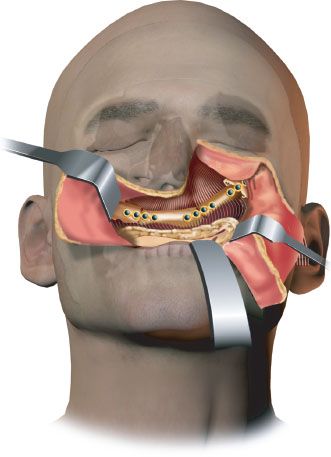
FIGURE 26.4 The bone graft is fixated to the native bone using miniplates. The soft tissue and skin paddle are used to line the palatal mucosal defect.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


