FIGURE 21.1 Schematic showing the key landmarks of the anterior abdominal wall and boundaries of the rectus sheath; the linea alba, the linea semilunaris, and the arcuate line.
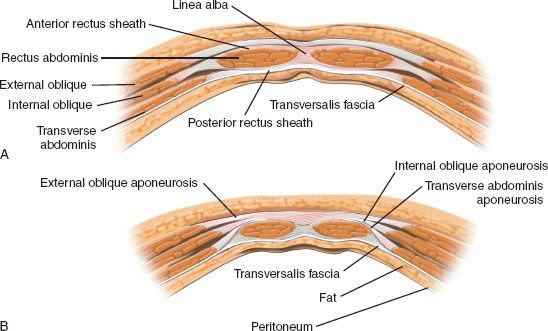
FIGURE 21.2 Diagram showing the contents of the rectus sheath and the layers of the sheath above and below the arcuate line. A. Relationships of the aponeuroses of the muscles of the anterior abdominal wall above the arcuate line. Note that the middle layer splits to surround the rectus muscles. B. The anatomy of the rectus sheath below the arcuate line. Note that all 3 aponeuroses pass anterior to the rectus muscles and only the travsversalis fascia is found posterior to the rectus muscles.
It is important to palpate the femoral pulse prior to harvesting the flap. Just proximal to the femoral pulse will be the external iliac artery and vein. The deep inferior epigastric artery and vein take origin from the external iliac artery and vein to run on the deep surface of the rectus abdominis muscle. These vessels run the entire vertical length of the muscle and anastomose with the superior epigastric vessels, which are the terminal branches of the internal mammary artery.
The major musculocutaneous perforators that supply the skin overlying the rectus abdominis muscle are found in the periumbilical area. They radiate from the umbilical area, but the dominant vessels run in a posterior, lateral and superior direction toward the ipsilateral tip of the scapula. Any rectus musculocutaneous free flap must be harvested with preservation of these perforating vessels remaining in continuity as they pass out from the muscle through the anterior rectus sheath to supply the overlying skin and subcutaneous tissues (Fig. 21.3).
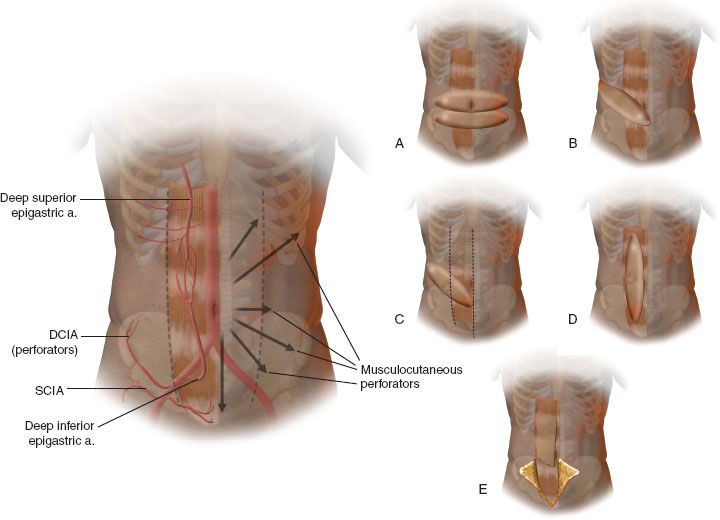
FIGURE 21.3 A. Diagram showing the primary vascular supply to the rectus muscle, the radiating periumbilical perforators, with the dominant vessels traveling in a trajectory toward the ipsilateral tip of the scapula. B–F. Options for the design of the skin paddle of the rectus abdominis myocutaneous flap.
When harvesting the rectus abdominis free flap as a musculocutaneous flap, the flap elevation proceeds as follows: The desired dimensions of the cutaneous paddle are outlined again in the area of the densest musculocutaneous perforators in the periumbilical area (Fig. 21.3A–F). The skin paddle may be used to replace palatal mucosa or facial skin or obliterate the orbit. Often, multiple cutaneous paddles may be created to reconstruct different aspects of the defect. If a desired dimension of the skin paddle is such that its length exceeds the width of the rectus muscle (as determined by the width of the defect), thereby requiring a portion of the flap that is not directly overlying muscle, this extension of the flap is drawn out in the direction of the vector from the umbilicus to the scapular tip. This allows capture of the axial vessels that penetrate through the anterior rectus sheath and travel in a plexus in this posterior, superior, and lateral direction.
As the dissection begins, the incision is made circumferentially around the skin paddle to the level of the anterior layer of the rectus sheath. For those cutaneous paddles that extend lateral to the linea semilunaris because of the need for a paddle wider than the width of the rectus sheath, the initial incision to the depth of the deep fascia begins medial to the linea semilunaris and extends to the level of the anterior layer of the rectus sheath and lateral to this line, to the aponeurosis of the external oblique muscle. Elevation of the most lateral portion of the component can proceed from lateral to medial taking the cutaneous portion directly off of the aponeurosis of the external oblique muscle. Upon reaching the linea semilunaris, the anterior layer of rectus sheath that will support the cutaneous paddle can be outlined circumferentially and incised. Laterally, this incision is made just medial to the linea semilunaris. This requires that the fasciocutaneous extension that was mobilized lateral to this line be dissected just medial to this lateral anterior sheath incision. Following the anterior sheath incision around the proposed skin paddle, a vertical incision can be made from the midportion of the inferior edge of the skin paddle inferiorly toward the expected origin of the deep inferior epigastric vessels. This incision is made through the skin and subcutaneous tissue and to the anterior layer of the rectus sheath. The anterior layer of the rectus sheath is incised and opened exposing the entire rectus muscle on the ipsilateral side. The rectus muscle superior to the skin paddle can be identified through this opening in the anterior rectus sheath. The muscle at this point superiorly can be transected, and the muscle and attached skin paddle can then be mobilized out of the rectus sheath from superior to inferior.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


