FIGURE 23.1 Squamous cell carcinoma of the maxilla requiring hemimaxillectomy and reconstruction.
PHYSICAL EXAMINATION
The physical examination of patients presenting with malignant tumors of the maxilla is relatively straightforward. The extent of the lesion should be evaluated intraorally to determine the size of the lesion and structures involved such as the maxillary alveolus, soft palate, buccal mucosa, and/or pharynx. Evaluation of the patient’s dentition for resection and reconstructive planning is paramount. The donor site must be examined to evaluate for signs of trauma or prior surgery. Flexible fiberoptic examination should be performed to evaluate the involvement of the floor of the nose as well as the nasal cavity and middle meatus.
INDICATIONS
Indications for maxillary reconstruction are listed below. The most common indications are malignant lesions of the maxilla, usually squamous cell carcinoma. Additional malignant or benign lesions are common indications for maxillectomy. Congenital anomalies requiring free tissue transfer are relatively rare.
• Malignant lesions of the maxilla (squamous cell carcinoma [SCCA], cancers of minor salivary gland origin, osteosarcoma)
• Benign lesions of the maxilla (ameloblastoma, giant cell tumors, meningioma)
• Traumatic avulsion/gunshot injuries
• Congenital anomalies
CONTRAINDICATIONS
There are no specific contraindications to maxillary reconstruction with the scapular osteomyogenous free tissue transfer. General medical conditions may prohibit complex reconstructive efforts, and a discussion with the patient regarding the use of an obturator should be undertaken in these cases. The selection of a reconstructive approach versus obturation requires a careful evaluation of the benefits of reconstruction versus the benefits of obturation. In general terms, the more extensive the defect, the more likely I am to recommend reconstruction given the low probability of satisfactory retention of a denture or an obturator. In smaller defects, reconstruction may be considered by patients who have the resources to consider osseointegrated implants for dental rehabilitation. In the rare event that the scapular donor site is contraindicated by previous trauma or surgery, other osseous reconstructive options may be entertained.
PREOPERATIVE PLANNING
The preoperative planning for maxillectomy and reconstruction is relatively standard. Nevertheless, several considerations merit mention.
Anatomy
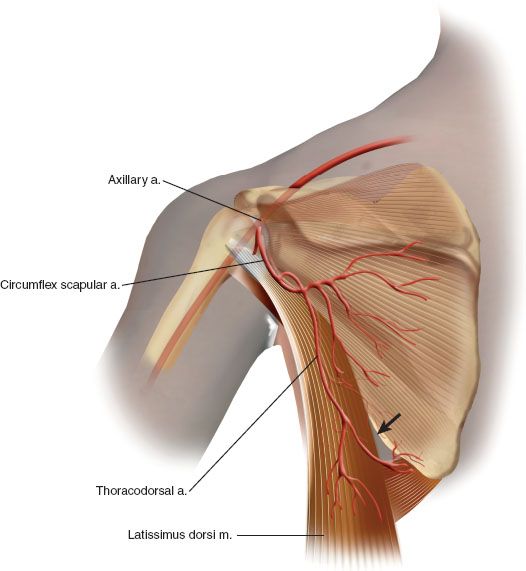
The circumflex scapular arterial system provides the vascular supply to a number of reconstructive options related to the donor site (Fig. 23.2). The circumflex artery arises from the subscapular artery, which is a branch of the axillary artery in the upper thorax. The scapula and surrounding muscle are supplied by the distal muscular and periosteal branches of the circumflex scapular artery. The cutaneous territories overlying the scapula receive blood supply via the transverse and descending cutaneous branches. The blood supply of the latissimus dorsi muscle is derived from the thoracodorsal artery, which arises from the circumflex scapular artery. Distal angular branches of the thoracodorsal artery supply the tip of scapula, and these form the basis of the scapular tip free tissue transfer.
Imaging Studies
The imaging studies required for successful maxillary reconstruction will vary depending on the situation; however, in general, computed tomography with contrast enhancement is relatively standard. The preoperative imaging required is usually driven by the ablative surgical plan, as imaging of the scapular donor site vascular anatomy is unnecessary.
SURGICAL TECHNIQUE
Flap Harvest
The patient is placed on a suction bean bag positioner prior to induction of anesthesia. After induction of anesthesia, the torso is turned approximately 45 degrees and the pelvis to 30 degrees. Access is sufficient when the tip of the scapula can be palpated easily, as shown in Figure 23.3. The contralateral arm is cradled without pressure on the shoulder, and all pressure points are padded. A pillow is placed between the knees and padding placed circumferentially around the feet and ankles. The patient is then secured with straps and wide tape to the operating table so that the table can be rotated without patient movement. Surgical technique starts with the incision design. If there is no plan for harvesting the skin, the incision is placed along the posterior axillary line. The anterior border of latissimus dorsi is identified, and the dorsal surface of the latissimus is mobilized to allow retraction if necessary (Fig. 23.4
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


