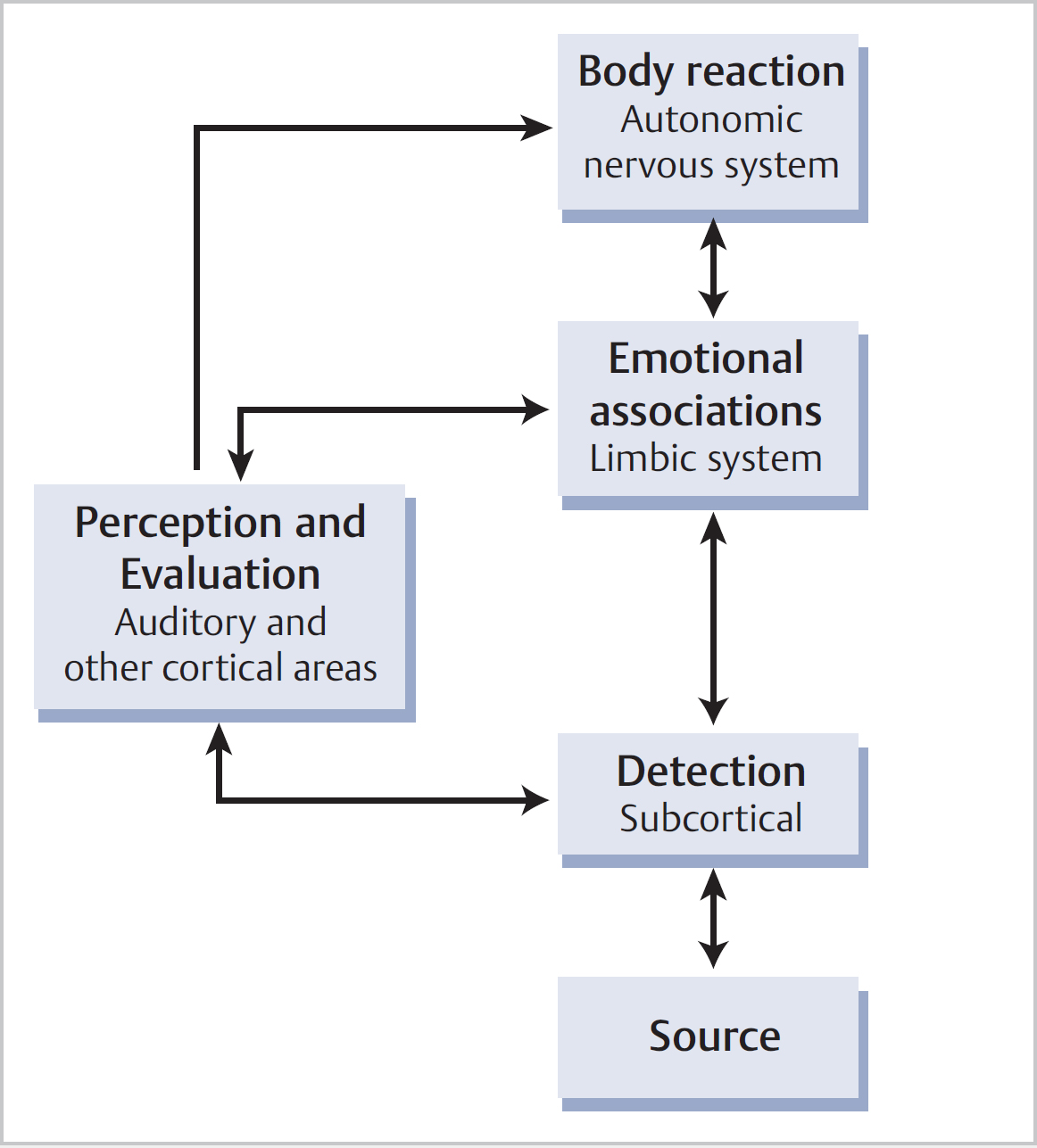
9 Tinnitus • Tinnitus is a symptom, not a disease • It is the sensation of sound not brought about by simultaneously externally applied mechanoacoustic or electrical signals—the perception of sound generated involuntarily within the head of an individual • Suggests problem between cochlea and auditory cortex • Central auditory system plays vital and critical role in experience of tinnitus • Somatosounds: – Muscular [eustachian tube (ET) function, stapedial, tensor tympani or palatal myoclonus] – Vascular (internal carotid artery or ICA)—pulsatile – Crepitus (temporomandibular joint) – Respiratory (patulous eustachian tube) • Subjective tinnitus: • Non-organic tinnitus: little known, and no definitive test • 94% of normal-hearing subjects placed in a soundproof room for up to 5 min have tinnitus-like experiences • 10% of adults have experienced tinnitus for >5 min • 4% have tinnitus causing sleep disturbance • 0.5% severely disabled by tinnitus • Some patients may have normal audiometry—but there may be subtle auditory dysfunction not identified by pure tone audiogram • 27% of cochlear implant patients experience no tinnitus, so tinnitus not ubiquitous in profound sensorineural hearing loss • Risk factors: • Emotional distress, insomnia, concentration, depression, potential self-harm • When silence is present there is random neural activity—if this is altered it may result in TRNA • Discordant damage between OHCs and IHCs can produce abnormalities of auditory nerve patterning resulting in further TRNA • TRNA detected at brainstem level, and perceived as intrusive/threat • Instigates sympathetic autonomic nervous system arousal—agitation, irritability, and limbic system (emotional) response—fear, anxiety • TRNA undergoes considerable processing in subcortical auditory pathways to finally be perceived at a conscious level as sound • Emotional distress instigated by conditioned response to TRNA • Problems with Jastreboff neurophysiological model (JNM): simplistic (but this helps with distressed patients); insists that conditioned responses involved—but no empirical evidence, and humans more complex than that implies; thus minimizes role of personality, experience, social context
9.1 Definition
9.2 Classification
 Cochlear—spontaneous otoacoustic emissions
Cochlear—spontaneous otoacoustic emissions
 Extracochlear
Extracochlear
 May arise from a source/trigger = tinnitus-related neural activity (TRNA) in cochlea, brainstem or higher centres (neurophysiological)
May arise from a source/trigger = tinnitus-related neural activity (TRNA) in cochlea, brainstem or higher centres (neurophysiological)
 Usually unable to determine the source clinically
Usually unable to determine the source clinically
 May be facilitated and sustained by hearing loss (HL)—reduced perception of external environmental sounds leading to increased central gain
May be facilitated and sustained by hearing loss (HL)—reduced perception of external environmental sounds leading to increased central gain
9.3 Incidence and Epidemiology
 Noise exposure
Noise exposure
 Hearing loss
Hearing loss
 Increasing age
Increasing age
 Pre-existing anxiety/depression
Pre-existing anxiety/depression
 Association with ear pathology (e.g., otosclerosis, Ménière, tympanic membrane perforation, vestibular schwannoma)
Association with ear pathology (e.g., otosclerosis, Ménière, tympanic membrane perforation, vestibular schwannoma)
 Ototoxic medication (e.g., salicylates, aminoglycosides, loop diuretics)
Ototoxic medication (e.g., salicylates, aminoglycosides, loop diuretics)
9.4 Impact
9.5 Jastreboff Neurophysiological Model of Tinnitus (Fig. 9.1)
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


