Thyroid Orbitopathy
Susan M. Tucker
Nancy A. Tucker
John V. Linberg
Thyroid orbitopathy represents an organ-specific autoimmune process that is usually associated with thyroid disease. Although Parry, Graves, and von Basedow are all credited with reporting the association between toxic goiter and ophthalmopathy in 1825, 1835, and 1840, respectively,1,2,3 a much earlier description of goiter with exophthalmos exists from 12th century Persian writings.4 A variety of terms have been used to describe the constellation of eye findings that can occur in patients with thyroid disease: thyroid orbitopathy, dysthyroid orbitopathy, thyroid ophthalmopathy, Graves’ ophthalmopathy, infiltrative ophthalmopathy, thyroid eye disease, endocrine ophthalmopathy, endocrine exo-phthalmos, and malignant exophthalmos. We prefer the term thyroid orbitopathy (TO) because the disease is known to occur in conditions other than Graves’ disease, and the orbit is the primary site of involvement.
Graves’ disease is the most common thyroid abnormality associated with TO, but other disorders of the thyroid can have similar ocular manifestations. These include Hashimoto’s thyroiditis, thyroid carcinoma, primary hyperthyroidism, and primary hypothyroidism.5,6,7 Approximately 25% to 50% of patients with Graves’ disease have or will develop clinically apparent TO,8,9 although fewer than 5% of patients with Graves’ disease have severe ophthalmopathy.10 However, subclinical orbital alterations can be detected on ultrasonography or computed tomography (CT) in the majority of patients.11,12 Of those patients with TO, approximately 10% are clinically euthyroid,13 but the majority of these patients have laboratory evidence of thyroid autoimmune disease, including TSH receptor antibodies (TRAb), antithyroglobulin, and/or antimicrosomal (also called antithyroid peroxidase) antibodies, negative TRH test, or negative T3 suppression test.6,13,14 Of patients with euthyroid orbitopathy, approximately 25% will develop thyroid dysfunction at 1 year and 50% at 5 years.7 In general, patients with euthyroid Graves’ disease tend to have less severe orbitopathy.15
In 70% to 85% of patients, eye signs develop within 18 months of the detection of the thyroid disease.13,16 The onset of TO is, however, unpredictable and can precede or occur many years after the diagnosis of Graves’ disease.17 Thyroid orbitopathy is usually a slow, progressive disease that may have a fluctuating course over months to several years before undergoing a gradual and often incomplete regression.18
EPIDEMIOLOGY
Overall, TO has an incidence rate of 16 females and 2.9 males per 100,000 population per year.7 Bimodal peak incidence rates for women occur from ages 40 to 44 years and 60 to 64 years; for men from ages 45 to 49 years and 65 to 69 years.7 There appears to be an increased prevalence of thyroid disease in smokers, for whom the relative risk of developing TO is twice as high as it is for nonsmokers.19 The reason for this difference is not known, but one possibility is that the decreased immunosuppression in smokers may allow greater expression of autoimmune processes. Other theories, which have been postulated to explain this association include orbital hypoxia, the effects of thiocyanate, increased circulating thyroglobulin levels leading to higher levels of thyroid antigen release, nicotine leading to adrenergic stimulation of the thyroid gland, direct irritative effects, and localized changes in the orbital circulation.20,21
There is some genetic predisposition; the concordance level is 50% in identical twins and 30% in nonidentical twins. Also, there is an increased prevalence of HLA-B8 and HLA-DR3 in Caucasians,22 HLA-DRW6 in African Americans,23 and HLA-B35 in Japanese patients with Graves’ disease.24 These HLA associations, however, are of no predictive value for the development of orbitopathy in patients with Graves’ disease. In keeping with its probable underlying autoimmune nature, patients with TO may have other organ-specific or generalized autoimmune disorders, such as diabetes mellitus, Addison’s disease, vitiligo, pernicious anemia, or myasthenia gravis.25
ETIOLOGY
Although a number of important details in the complex pathogenesis of TO have been clarified in recent years, the precise nature of this autoimmune process and the source of the offending antibodies are still poorly understood and largely speculative.
Current understanding of this autoimmune process in the pathogenesis of thyroid orbitopathy is the result of developments that have occurred over the past 50 years. Historically, before an underlying autoimmune etiology was suspected, overactivity of the thyroid gland was thought to be due to increased thyroid-stimulating hormone (TSH, thyrotropin). Once assays were available for TSH, however, TSH was found to be low in most patients with Graves’ disease. In 1956, Adams and Purves26 isolated a factor in the serum of patients with Graves’ hyperthyroidism that caused stimulation of the animal thyroid gland. This factor was very similar to TSH but had a longer half-life, and was therefore called long-acting thyroid stimulator (LATS). In 1964, Kriss et al.27 showed that LATS had the structure of an IgG immunoglobulin, and its action could be neutralized by thyroid tissue, indicating that it was an antibody. Further experiments have shown that hyperthyroidism in Graves’ disease is due to the binding of stimulatory autoantibodies to the TSH receptor (TSAb) on thyroid follicular cells.8
In contrast, the pathophysiology of TO is less well understood. Circulating antibodies against proteins contained in eye muscle (63 kDa and 64 kDa) and retro-orbital fibroblasts (23 kD) are frequently detected in sera of patients with TO, but they lack tissue and disease specificity.28 Most investigators agree that these antibodies are produced secondary to the disease process and are probably not involved as primary autoimmune targets. Several investigators have examined the TSH receptor as a possible orbital autoantigen, however, there currently exists little evidence to directly link this receptor in the pathogenesis of TO. Although in several studies the level of TSH receptor antibodies (TSAb) has been correlated with the degree of ophthalmopathy (eyelid swelling, proptosis, and extraocular muscle involvement),29,30 other studies have found no such association.31,32 Insulin-like growth factor 1 (IGF-1) receptor, which is highly expressed in Graves’ fibroblasts, may be another possible autoantigen.33 However, the identity of the relevant self-antigen remains to be determined.
Although the relative contribution of cellular and humoral immunity to the pathogenesis of TO remains uncertain, it is likely that both are important for full clinical expression and propagation of the autoimmune process within the orbit.34 Orbital fibroblasts appear to have a central role in the pathogenesis of TO through mechanisms that are not completely understood but which are likely mediated by cytokines.8,34,35 Orbital fibroblasts have been shown to have distinct phenotypic properties, with the ability to activate a diverse array of immunocompetent cells with the release of such chemoattractants as the cytokine IL-16 and the chemokine RANTES.36 These chemoattractants may orchestrate T lymphocyte infiltration of many tissues, including the thyroid.36 Activated endomysial fibroblasts also then produce glycosaminoglycans (mostly hyaluronan) and collagen, causing edema and fibrosis.8 Additionally, a subpopulation of orbital fibroblasts appears capable of undergoing adipocyte differentiation in vitro, which contributes to the orbital volume augmentation.37
PATHOLOGY
The predominant orbital pathology is inflammation of the orbital soft tissues and the interstitial connective tissue of the extraocular muscles. This immune-mediated inflammation consists mostly of lymphocytes, plasma cells, and a scattering of mast cells.38,39 These inflammatory changes differ from the more exuberant lymphocytic infiltration of the orbital fat, extraocular muscles, and their tendinous insertions seen in idiopathic orbital inflammatory disease.40 Also, eosinophils and germinal centers with follicles, such as may be found in other noninfectious orbital inflammations, are typically absent in thyroid orbitopathy.38 In the latter stages of TO, interstitial fibrosis results in muscle atrophy and degeneration.41
The inflammatory process involves the endomysial connective tissue, and other orbital structures are affected to a lesser extent. The lacrimal gland typically shows a mild mononuclear cell infiltration and interstitial edema, with mild fibrosis and atrophy of acinar structures.41 Similarly, in the contiguous orbital fat, there is only a small amount of inflammation.41 The tendinous insertions onto the globe and the optic nerve meninges generally show no inflammation at all.
The increased orbital volume is due to the accumulation of glycosaminoglycan, in which hyaluronan predominates, and collagen in the connective tissues of the extraocular muscles (not the myocytes themselves) and the orbital fat compartments, and de novo adipogenesis in these tissues.8 The hydrophilic glycosaminoglycan macromolecules result in an osmotic accumulation of water within the perimysial and retro-ocular connective tissues. Impaired venous drainage from the orbit may also contribute to the increased orbital volume. In particular, enlargement of the superior rectus muscle may reduce venous outflow by compressing the superior ophthalmic vein.
CLASSIFICATION
Attempts have been made to classify the various manifestations of thyroid orbitopathy. Werner42 introduced the NOSPECS classification system in 1963. The first version did not allow for quantitation of the severity of ophthalmopathy and was therefore updated by the American Thyroid Association in 1977 by devising an ophthalmopathy index scoring system to allow improved evaluation of the severity of the ophthalmopathy within each class (Table 1).43 In 1989 Bartalena et al.44 proposed a newer classification system in which the index scoring system was modified to place more significance on the vision-threatening manifestations of thyroid orbitopathy. Bartalena et al. proposed that the scores in each class could be mathematically added to arrive at a final ophthalmopathy score for each patient.
TABLE 1. Classification and Grading of Thyroid Orbitopathy | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
We believe that the NOSPECS classification is a helpful mnemonic for medical students and beginning ophthalmology residents as a reminder of the various manifestations of thyroid orbitopathy. Otherwise, classification systems should be discouraged because patients usually do not fit into a single class; there is often not an orderly progression from one class to the next; the use of Snellen visual acuity alone to assess optic nerve involvement is inadequate; the classification is not helpful in making treatment decisions, and the classification has almost no prognostic value. Even as a means of standardizing the results of clinical trials, comparing the final ophthalmopathy score of one patient with that of another is difficult to interpret. We believe it is better to carefully document and follow each manifestation of a given patient’s thyroid orbitopathy and base treatment decisions, accordingly.
CLINICAL MANIFESTATIONS
The clinical manifestations of thyroid orbitopathy are due to inflammation, edema, and fibrotic changes within the soft tissues of the orbit, resulting in enlargement of retrobulbar tissues and restriction of extraocular muscle motion45 (Figs. 1 and 2). Although asymmetric eye involvement is quite common, unilateral eye disease occurs in only 5% to 14% of patients with TO.11,46
 Fig. 1 Typical clinical presentation of moderate thyroid orbitopathy, showing axial proptosis, eyelid retraction, prolapse of orbital fat, conjunctival chemosis, and prominent vessels over the horizontal rectus muscle insertions. |
 Fig. 2 Patient with severe thyroid orbitopathy, showing marked eyelid retraction, strabismus, conjunctival chemosis, injected vessels, and exophthalmos. |
EXOPHTHALMOS
Thyroid orbitopathy is the most common cause of both unilateral and bilateral proptosis in adults. Exophthalmos, defined as measurement of 2 mm or more above normal limit (upper normal limit of globe protrusion in Caucasians is 20 mm; African Americans, 22 mm; and individuals of Japanese descent, 18 mm),43,47,48 occurs in 20% to 30% of patients with Graves’ disease and in 40% to 70% of patients with TO.46 The proptosis is bilateral in 80% to 90% of affected individuals,46 but it may be asymmetric (Fig. 3). Thyroid orbitopathy results in an axial proptosis as the muscle and connective tissue volume behind the eye increases; displacement of the globe in any other direction is suggestive of another diagnosis. When the pressure within the retrobulbar tissues exceeds the forces counteracting proptosis, the rare complication of subluxation of the globe anterior to the eyelid may occur.
 Fig. 3 Patient with very asymmetric thyroid orbitopathy. Left eye shows proptosis and marked inferior rectus restriction, while right eye demonstrates normal motility on upgaze. |
The increased orbital volume is usually due to both extraocular muscle and orbital fat expansion; however, patients younger than 40 years of age are more likely to exhibit orbital fat enlargement in the absence of muscle enlargement, whereas patients over 70 years are more prone to severe, fusiform muscle enlargement without significant changes in orbital adipose tissue volume.49 Forbes et al.11 reported enlargement of the fat compartment in 46% of patients with TO, whereas 8% had increased fat compartments with normal muscle volumes (Fig. 4).
 Fig. 4 Axial CT scan of patient with thyroid orbitopathy, extreme proptosis, and no clinical evidence of optic neuropathy. Note the increase in orbital fat volume without significant extraocular muscle enlargement. In this case axial proptosis has allowed spontaneous decompression of increased orbital volume. |
EYELID CHANGES
In the inflammatory stage, careful examination of these patients may reveal eyelid edema or a fine tremor of gently closed eyelids. Von Graefe’s sign is the lag of the downward movement of the upper eyelid on slow downgaze. Early eyelid lag is best detected by having the patient hold a fixation target at arm’s length high above the head; the patient maintains fixation as he or she slowly lowers the target.
Thyroid orbitopathy is the most common cause of upper eyelid retraction, which may be accentuated by the coexistence of exophthalmos. Eyelid retraction is the most common sign of TO, present in 75% of patients at diagnosis and occurring at some point in the clinical course in more than 90% of patients.7 Upper eyelid retraction may be due to adrenergic overaction of the Müller’s muscle, fibrosis and functional shortening of the levator muscle, and/or overaction of levator-superior rectus muscle complex, secondary to fibrosis of the inferior rectus muscle.50 With minimal eyelid retraction, a misdiagnosis of ptosis of the opposite eyelid can be made. The upper eyelid retraction in Graves’ disease has a characteristic temporal flare, with a greater amount of sclera visible laterally as compared with medially. This may occur, in part, because the eye in primary position looks away from the orbital axis and projects more lateral sclera.51 The lower eyelid retraction may result from similar changes in the capsulopalpebral fascia (Fig. 2).
EXTRAOCULAR MUSCLE INVOLVEMENT
Thyroid disease should be considered in all cases of adult-onset strabismus. Using sensitive measurement techniques, such as ultrasound, CT, and MRI, extraocular muscle enlargement has been noted in 60% to 98% of patients with Graves’ disease,46 and restrictive extraocular myopathy occurs in approximately 42% of patients with TO.52 The most common motility abnormality is limitation of elevation owing to fibrosis of the inferior rectus muscle, which results in diplopia on upgaze (Fig. 3). The second most common muscle to be involved clinically is the medial rectus, followed by the superior rectus/levator complex, and finally the lateral rectus.53,54 Some studies have found the medial rectus muscle to be more frequently involved than the inferior rectus,12,55 and one study found the superior rectus muscle to be most frequently involved.56 Isolated muscle enlargement usually involving the inferior rectus muscle may occur in a small percentage of patients and often remains monomuscular.57 This differs from monomuscular myositis, which most commonly involves the medial rectus.58 The mechanisms underlying disproportionate involvement of the extraocular muscles are poorly understood. It may, in part, be due to the well-developed connective tissue system around the inferior oblique and inferior rectus muscles, which also have the greatest number of septal connections with the adjacent periorbit.59
The increased intraocular pressure measured during upgaze in patients with thyroid orbitopathy is a normal phenomenon exaggerated by thyroid orbitopathy and other infiltrative and congestive orbital processes.60 When restriction of the inferior rectus muscle occurs, the intraocular pressure may increase by 6 mm Hg or more in upgaze as compared with primary gaze. It is often not an indicator of early disease because it occurs infrequently in patients with minimal eye findings.60 Significant reduction in intraocular pressure has been reported following decompression surgery and botulinum A toxin injections into the inferior rectus muscle.61,62
LACRIMAL GLAND
Although still speculative, a primary lacrimal gland dysfunction with an altered rate of tear production or a change in the protein composition of tears may be present in patients with thyroid orbitopathy.63
CORNEAL AND CONJUNCTIVAL INVOLVEMENT
Corneal involvement due to exposure keratitis may result from proptosis, upper eyelid retraction, lower eyelid retraction, lagophthalmos, or a combination of these. Exposure keratitis may range from minimal staining of the lower cornea to severe keratitis and even corneal ulceration. Superior limbic keratitis (SLK) may exist, especially when upper eyelid retraction is present. SLK may be a prognostic marker for severe TO: in a study of 57 patients with SLK by Kadrmas et al.,64 16/33 (48.5%) had severe enough orbitopathy to require orbital decompression.
Conjunctival chemosis and injection of the conjunctival and episcleral vessels overlying the insertions of the extraocular muscles can be seen in the inflammatory stage of TO.
OPTIC NEUROPATHY
The prevalence of optic neuropathy with visual loss in patients with thyroid orbitopathy is less than 5%.65 Optic neuropathy is, however, the most common cause of blindness secondary to thyroid orbitopathy. Left untreated, as many as 21% of patients develop an irreversible deficit in visual acuity.65,66,67 Its onset is often insidious and may be masked by other symptoms. These patients are usually older (ages 50 to 70), have a later onset of thyroid disease, and more often have diabetes.65,68 The ratio of women to men is widely variable among reported series; in a large retrospective study of 215 patients with optic neuropathy, the ratio of women to men was 2.4:1.69 Optic neuropathy is usually bilateral, but up to one-third of cases may be unilateral.65,68
Most cases of optic neuropathy are due to compression of the optic nerve by the enlarged extraocular muscles at the orbital apex (Fig. 5). Patients with compressive optic neuropathy have a more symmetric involvement of the extraocular muscles as compared with most patients with thyroid disease.65 Although patients with optic neuropathy usually have proptosis, optic neuropathy can occur without significant proptosis in patients whose orbital septum efficiently limits anterior globe displacement, despite increased retrobulbar pressure. Very rarely, optic neuropathy can occur without significant muscle enlargement. In these cases, it is postulated that a short optic nerve is being stretched or the optic nerve is being compressed by surrounding orbital fat.49 These cases are so rare that optic neuropathy in the absence of muscle enlargement or proptosis should be investigated thoroughly to rule out other etiologies.
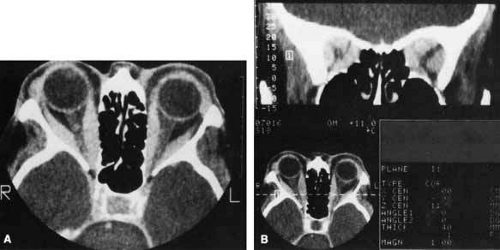 Fig. 5 A. Axial CT scan of a patient with compressive optic neuropathy. Note that position of globe shows only mild proptosis, and orbital fat is not increased in volume. The posterior portion of the extraocular muscles is markedly enlarged, compressing the optic nerve. B. Coronal CT scan of the orbital apex in the same patient clearly shows displacement of orbital fat by enlarged muscles. The apex is “crowded,” consistent with clinical findings of optic neuropathy. |
Although a history of decreased vision should be carefully sought, it is important to realize that optic neuropathy can occur in a significant number (18%) of patients with visual acuities in the range of 20/20 to 20/25 6/6 to 6/7.5 [Metric equivalent given in parentheses after Snellen notation]).68 An afferent pupillary defect is present in 35%.68 An abnormal disc (either swollen or pale) is seen in only 53%. Visual field defects are present in 66%.68 In a large retrospective study of 291 eyes with visual field defects from optic neuropathy, 49% were inferior, 37% were central or cecocentral, 12% showed generalized depression, 1% had superior depression, and 1% had bitemporal depression.69 The Farnsworth-Munsell 100-hue color vision test is a sensitive indicator of optic nerve dysfunction, but pseudoisochromatic screening procedures (e.g., Ishihara plates) rarely identify an acquired color defect, unless optic neuropathy is severe.68 The pattern reversal VEP is very sensitive at detecting early optic neuropathy and may be a useful means of following patients after treatment.
DIAGNOSTIC TOOLS
When the ophthalmologic signs and symptoms raise a suspicion of underlying thyroid disease, the systemic thyroid status should be assessed. This includes a history pertaining to weight loss, increased appetite, heat intolerance, difficulty sleeping, weakness of the limb girdle muscles, and mood changes. The thyroid gland should be palpated to detect an enlargement. Less commonly, infiltrative dermopathy characterized by pretibial myxedema and thyroid acropathy characterized by clubbing and subcutaneous fibrosis of the fingers may be seen. Laboratory tests should be ordered to confirm a suspected thyroid abnormality. All patients with newly diagnosed thyroid disease should be referred to an endocrinologist or internist for management and follow-up of the systemic thyroid status.
Some patients with thyroid orbitopathy may initially present with nonspecific complaints, such as eyelid fullness, ocular irritation, or lacrimation and the diagnosis of thyroid orbitopathy may not be suspected. These clinical presentations are most often not thyroid related and may be caused by dry eye, lacrimal outflow obstruction, or a variety of primary abnormalities of the eyelid, conjunctiva, or cornea. In these situations a high index of suspicion is required to search for clinical evidence of thyroid disease, followed by appropriate laboratory investigations. The ophthalmologist’s examination must be directed toward the detection of subtle signs of thyroid orbitopathy.
LABORATORY INVESTIGATION
In patients with suspected Graves’ disease, laboratory tests can be used to detect hyperthyroidism. Thyroid stimulating hormone immunoradiometric assay (TSH-IRMA, sensitive TSH, sTSH) reliably separates normal from hyperthyroid states. It is the most useful first-line test of thyroid function in patients with thyroid disease. It is so consistent, sensitive, and reliable that it renders the TRH stimulation test almost obsolete in the diagnosis of hyperthyroidism.70 One of the few remaining indications for the TRH stimulation test is in the detection of hyperthyroidism in hospitalized patients with severe thyroidal illness.71 A general strategy for laboratory testing is to first obtain results of the TSH-IRMA. If this is normal, then the patient is said to be euthyroid. In patients with suspected thyroid orbitopathy, further testing for antibodies is then indicated. If the TSH-IRMA value is elevated, or undetectable, then overt hypothyroidism or hyperthyroidism can be distinguished from subclinical disease by measuring the free T4. Some clinicians, therefore, routinely initially order the free T4 test along with the TSH-IRMA to avoid the delay and inconvenience of the stepwise approach to diagnosis.
Three antibodies can currently be measured using standard techniques: thyrotropin receptor antibodies, antimicrosomal antibodies, and antithyroglobulin antibodies. In Graves’ disease, thyrotropin receptor antibodies are present in 85% to 95% of patients with untreated Graves’ hyperthyroidism and in approximately 50% of patients with euthyroid Graves’ disease. Antimicrosomal antibodies are found in 60% of patients, and antithyroglobulin antibodies are present in approximately 30% of patients.70,72 When these tests are positive they help support a diagnosis of autoimmune thyroid disease. Thyrotropin receptor antibody levels are also helpful in pregnant women because of the predictive value of an increased thyrotropin receptor antibodies for neonatal Graves’ disease in the infant, irrespective of the mother’s thyroid status.72
ULTRASONOGRAPHY
Ultrasonography can detect early thyroid disease in patients with equivocal laboratory tests; however, its usefulness depends on the skills and experience of the ultrasonographer. Most patients with Graves’ disease, even those without overt eye findings, have ultrasonographic evidence of extraocular muscle involvement.73 This test may also be helpful in distinguishing between active and inactive disease; there is a lower internal reflectivity of the extraocular muscles in active as compared with inactive disease.74 Ultrasonography is, however, less suited than CT to assessing muscle thickness at the orbital apex.
COMPUTED TOMOGRAPHY (CT)
CT is not necessary in most patients who present with a clinical picture and supporting laboratory evidence of Graves’ disease. It is, however, indicated when optic neuropathy is suspected, before orbital decompression, to examine the anatomic relationship of the orbit to both the sinus cavities and the cribriform plate, in patients with atypical proptosis or motility disturbances; or instead of ultrasonography to detect early thyroid orbitopathy in patients with equivocal results of laboratory tests. Like ultrasonography, CT allows reliable identification of even minimal enlargement of the recti muscles.40 Of those patients with clinical unilateral thyroid orbitopathy, CT will detect subclinical enlargement of the extraocular muscles on the contralateral side in 50%.75
The most characteristic CT finding in thyroid orbitopathy is enlargement of the extraocular muscles, which is usually bilateral and symmetric and has a fusiform configuration, with sharply defined borders and sparing of the tendinous insertions. Atypical cases with tendon involvement and blurred muscle margins have been described.75
The pattern of muscle enlargement on CT parallels that seen clinically. The inferior rectus is the most commonly involved, followed by the medial rectus, superior rectus, and lateral rectus. Other findings include proptosis and anterior prolapse of the orbital septum due to excessive orbital fat and muscle swelling (see Fig. 4).76 Also, lacrimal gland enlargement and bone remodeling without erosion can occur.75 Patients at risk for developing optic neuropathy may also have severe apical crowding, a dilated superior ophthalmic vein, and anterior displacement of the lacrimal gland.68 Of these, apical crowding is the most sensitive indicator for the presence of optic neuropathy (Fig. 5A).56 Both axial and coronal CT cuts should be obtained; the coronal plane is needed to assess the enlargement of the extraocular muscles at the apex (see Fig. 5B).
MAGNETIC RESONANCE IMAGING (MRI)
Although more expensive than CT, magnetic resonance imaging (MRI) is the preferred imaging modality for delineating subtle compressive optic neuropathy. MRI using 1.5 tesla units and orbital surface coils provides optimal spatial resolution of the orbit. MRI may also be useful in distinguishing between active and inactive disease by recognizing the increased fluid associated with inflammation: extraocular muscles that have acute inflammation have longer T2 relaxation times owing to the higher water content.77,78,79 However, this is not widely used because it is difficult to perform and time-consuming and may be of limited use in the decision of whether or not to apply immunosuppression therapy.77,78
VISUAL FIELD
A visual field should be performed in all patients suspected to have optic neuropathy and is useful when following patients after initiation of treatment.
DIFFERENTIAL DIAGNOSIS
Most patients with thyroid orbitopathy present with typical signs and symptoms of bilateral eyelid retraction and proptosis that are almost pathognomonic of thyroid orbitopathy. In these patients the diagnosis is easily made and confirmed through laboratory testing. Occasionally, however, a patient with thyroid orbitopathy may be misdiagnosed.
Clinical presentations in which the possibility of thyroid orbitopathy is often overlooked include ocular irritation, lacrimation, and minimal eyelid retraction in early thyroid orbitopathy. Thyroid orbitopathy may also mask as a superior oblique palsy or be confused with the motility disturbances seen in myasthenia gravis. When thyroid orbitopathy presents as an acute orbital inflammation, it must be distinguished from myositis, orbital cellulitis, or scleritis. Myositis is more likely to be unilateral, involving a single muscle, with tendon involvement revealed by ultrasonography or CT. The differentiation between myositis and thyroid muscle enlargement on CT may, however, be difficult because the tendon swelling in myositis is not a consistent finding and because multiple muscles may be affected.75 Unlike thyroid orbitopathy, myositis most commonly involves the medial rectus (57%), followed by the lateral rectus (36%).80
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


