Therapeutic Uses of Prism for Binocular Vision Disorders
Susan A. Cotter
Kelly A. Frantz
Introduction
Indications for a Prism Prescription
A number of binocular vision anomalies can be addressed with the prescription of spectacle prism. Prism is particularly useful for alleviating diplopia in patients with recent-onset strabismus or decompensated phorias. Prism can also relieve asthenopia in patients who have long-standing difficulty compensating for a high phoria. The effect of a prism correction is to reduce or eliminate the demand on the patient’s fusional vergence system, allowing more comfortable fusion. It is necessary for the patient to be capable of sensory fusion (the ability to blend the two eyes’ images cortically) to benefit from the reduction in motor fusion (vergence) demand that prism affords. Thus, prism is not indicated for patients with significant suppression or for those with anomalous correspondence.
Disadvantages of a Prism Prescription
Some practitioners are hesitant to prescribe prism because of its known or perceived disadvantages. These drawbacks can be grouped into three major categories: subjective factors, patient “dependence” on prism, and prism adaptation.
Subjective Factors
Subjective factors include cosmetic appearance of the prism spectacles owing to thickness and reflections, spectacle weight, and image aberrations or distortions. These factors are not an issue with small amounts of prism. When larger prism values are needed, many of these factors can be addressed readily using spectacle frames with a small eye size and lens materials with a high index of refraction (to reduce edge thickness and weight of the lenses). Antireflective coatings eliminate most reflections. Spectacle prisms can produce chromatic aberration, which causes the patient to perceive colored fringes at the edges of objects. This is particularly noticeable with Fresnel membrane prism powers >15 prism diopters (Δ).1 In addition, distortions increase with increasing prism power. Thus, it is wise to prescribe the minimal prism needed, and to split the prism power equally between the two eyes (except in some cases of paretic deviations). Patients also may need to adapt to the appearance of curving and slanting of lines viewed through their prism spectacles.2 Whereas some patients may find unwanted distortions too great a challenge to accept, other patients will gladly accept some distortion in exchange for relief of their asthenopia or diplopia.
Dependence on Prism
Practitioners are concerned that a patient may become “dependent” on prism to achieve comfortable binocular vision. Indeed, some patients may continue to require prism spectacles for many years, although they may prefer prism wear to asthenopia. Other patients may find that after some time wearing prisms, it is possible to have the prism power cut back slowly as fusional vergence improves passively.3,4 Prism power also can be decreased following improvement in fusional vergence amplitudes by means of vision therapy or orthoptics.
Prism Adaptation
Prism adaptation refers to an increase in the angle of deviation (strabismus or phoria) resulting from wear of prism that fully or partially compensates for the deviation. The angle can increase by an amount up to the full magnitude of the prism correction. For example, if a patient with an initial angle of 20Δ of exophoria is prescribed 5Δ base-in (BI), the expected exophoria measured though the prism spectacles should be 15Δ. If the patient adapts fully to the prism, however, the angle measured through the prism would increase to 20Δ, and the angle immediately on removal of the prism would be 25Δ. This process can occur in as little as 15 minutes.5 If prism wear is discontinued, the angle should return to its original magnitude within minutes to hours (or occasionally, weeks).6 If a patient exhibits prism adaptation, prism wear is not helpful and alternative treatments should be explored.
It is common for patients with normal sensory and motor fusion to show prism adaptation.5,7 However, prism generally would not be considered for such individuals, because it is unlikely they would experience symptoms. Patients capable of sensory fusion, but having a high phoria or intermittent strabismus, are much less likely to show prism adaptation and, therefore, can often benefit from a prism correction.8 It is possible, however, for some patients with strabismus to show prism adaptation if they have deep suppression or anomalous correspondence,9 so evaluation for these conditions is necessary before prescribing prism. Because prism adaptation often occurs quickly, it is possible to evaluate a tentative prism prescription in the office and, if prism adaptation occurs, to pursue alternative treatment. If a question remains regarding whether prism adaptation will occur, it is also possible to prescribe a Fresnel membrane prism (Fresnel prism) (Fresnel Press-On; Fresnel Prism and Lens Co., Eden Prairie, MN; fresnelprism.com) for a 1- to 2-week trial period; if the patient’s ocular deviation increases, wearing of the prism can be discontinued.
Types of Prism Prescriptions
Prisms can be used for disorders of binocular vision in various ways. The most common forms of prism are prescribed with the intent of restoring or maintaining binocular vision by optically reducing or eliminating the demand on the patient’s fusional vergence system or by directing the patient’s eyes into a position of gaze where fusion is possible. Other uses include improving the cosmetic appearance of certain strabismic deviations and disrupting anomalous correspondence.
Neutralizing or corrective prisms are equal in magnitude to the ocular deviation measured on the alternate cover and prism test. Because these prisms optically neutralize the deviation, the demand on controlling fusional vergence is eliminated completely. This type of prism prescription provides bifoveal stimulation and is typically reserved for patients with constant strabismus who have extremely limited or absent compensating fusional vergence ability, but who are capable of sensory fusion.
Relieving prisms are prisms of a lesser magnitude than the ocular deviation as measured by the alternate cover and prism test. These prisms optically reduce the demand on the patient’s fusional vergence system by partially correcting the angle of deviation. To maintain fusion, the patient must use some of his or her own fusional vergence. Relieving prisms are the most commonly prescribed type of prism and are typically provided to patients with normal sensory fusion but reduced compensating vergence ability.
Inverse or reverse prism refers to prisms prescribed such that the bases are in the direction opposite to that used to elicit fusion; thus, this type of prism optically increases the demand on the patient’s fusional vergence system. The most common use of inverse prism is as a vision therapy or orthoptics training procedure designed to increase vergence amplitudes. Inverse prism can also be prescribed in a spectacle lens to make certain types of cosmetically apparent strabismic deviations less noticeable to the casual observer.
Yoked or version prisms are a pair of prisms placed with their bases in the same direction before each eye. For example, prisms might be base-down (BD) before both eyes, or BI right eye and base-out (BO) left eye (also referred to as “base-left,” as in Figure 57.1). The prisms create an apparent displacement of viewed objects in a parallel direction toward the apices of the prisms causing the eyes to move into that position of gaze. Typically, yoked prisms are used to direct the patient’s eyes into the gaze position where the deviation is smaller and the patient has the potential for comfortable fusion. Yoked prisms are an option for many patients with noncomitant strabismus including those with AV patterns.
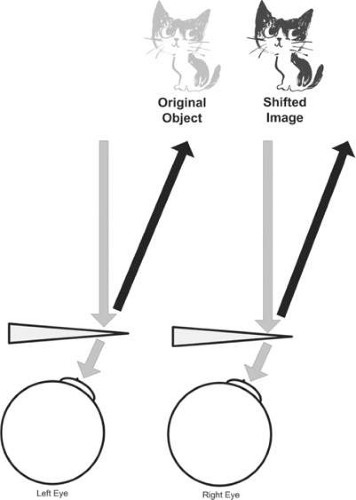 Figure 57.1. Yoked base-left prisms (base-out before the left eye and base-in before the right eye) create an apparent displacement of viewed object (cat) toward the apices of the prisms (i.e., to the right), which will cause the eyes to move to the right. |
Sector or regional prism refers to a prism that is placed on only a portion of a patient’s spectacles so that the prism is used for distance or near fixation only, or for a specific field of gaze. Prescribed as either relieving or neutralizing prism, the prism either reduces or eliminates the patient’s fusional vergence demand at a particular distance or field of gaze. For example, sector BO prism can be prescribed on only the top half of the spectacle lenses for a patient with a divergence insufficiency who has an intermittent esotropia at distance and a smaller-sized and asymptomatic esophoria at near (Fig. 57.2)
 Figure 57.2. Sector Fresnel prism placed on top half of spectacles for a patient requiring prism for distance viewing only. |
Overcorrecting prisms are those whose magnitude is larger than the ocular deviation as measured by the alternate cover and prism test. These prisms optically change the direction of the deviation and thus optically reverse the demand on the patient’s fusional vergence system. The main use of overcorrecting prisms is for the treatment of anomalous correspondence,10 which is beyond the scope of this chapter.
Prism Prescription for Patients with Nonstrabismic or Low-Frequency Strabismic Deviations
General Considerations
Nonstrabismic binocular vision disorders generally are long-standing conditions that may slowly deteriorate over time, sometimes leading to intermittent strabismus. Whether the patient remains phoric or develops low-frequency, intermittent strabismus, the symptoms may respond to spectacle prism. In contrast, conditions that appear to be of recent onset, often accompanied by neurologic signs or symptoms, obviously require appropriate medical evaluation. Common symptoms of long-standing binocular vision disorders include eyestrain, intermittently blurred or double vision, loss of place when reading, words appearing to move on the page when reading, headaches associated with visual tasks, and inability to perform sustained near work. Symptoms often increase with fatigue or following prolonged periods of demanding visual tasks, such as reading and computer work.11 Whereas many of these conditions can be treated with vision therapy or orthoptics, prism spectacles can provide rapid relief of symptoms for certain patients. It is important to keep in mind that a prismatic prescription will yield the greatest benefit for symptomatic patients with little or no suppression.
Conditions for Which Prism Can be Useful
Prismatic prescriptions are particularly useful for patients with horizontal or vertical deviations having similar magnitude when measured with both distance and near fixation, because one prism power can be used for all distances. However, prism can also be prescribed successfully for patients with a distance esodeviation and for some patients with a near point exodeviation (i.e., convergence insufficiency). In contrast, an esodeviation occurring only at near point is best managed with a plus addition, often in bifocal or multifocal form.
Basic Exodeviation
Patients with a basic exodeviation have an exophoria or intermittent exotropia of similar magnitude when measured with distance and near point fixation. Those with inadequate compensating convergence ability can experience uncomfortable, blurred, or double vision at all working distances. Vision therapy or orthoptics is recommended to treat this condition; however, for large exodeviations, BI prism can be helpful.11
Basic Esodeviation
Patients with a basic esodeviation have esophoria or intermittent esotropia of similar magnitude when measured with distance and near point fixation. If these patients have inadequate divergence ranges, they can experience uncomfortable, blurred, or double vision at all working distances. Prescribing BO prism is an appropriate method of treating this condition.11
Divergence Insufficiency
Patients with divergence insufficiency (i.e., primary, without underlying neurologic pathology) have esophoria or intermittent esotropia with distance fixation, and minimal deviation at near point (ranging from esophoria to exophoria). Inadequate divergence ability to compensate for the distance esodeviation generally results in long-standing complaints of intermittently blurred vision or diplopia.11 Unless neurologic signs or symptoms are present, these patients can be treated with BO prism spectacles, and further medical evaluation typically is unnecessary.12
Convergence Insufficiency
Patients with convergence insufficiency have a greater magnitude of exodeviation with near point fixation compared with distance (where orthophoria or a smaller exodeviation is usually present). Convergence skills at near point are inadequate, including a receded near point of convergence. Symptoms, including asthenopia, headaches, blurred vision, and diplopia, are often associated with near point tasks.13 Patients with convergence insufficiency are commonly treated with vision therapy or orthoptics, with office-based vergence/accommodative vision therapy shown to be more effective than either placebo therapy or home-based therapies using pencil push-ups or computerized therapy.14,15 Some patients with convergence insufficiency may however, prefer a more passive type of treatment, such as prism glasses. In a randomized clinical trial, reading glasses with BI prism were compared with placebo reading glasses in a group of 72 children ages 9 to <18 years who were diagnosed with symptomatic convergence insufficiency.16 No difference in the patients’ symptoms scores between the prism and placebo groups were found after 6 weeks of wearing the glasses. In contrast, BI prism glasses have been shown to decrease symptoms significantly in cases of presbyopia in which the patient has convergence insufficiency.17 Thus, there is support for the use of BI prism glasses for patients with presbyopia who have convergence insufficiency. It is unknown, however, whether adult patients who are pre-presbyopic with convergence insufficiency benefit from a BI prism prescription.
Vertical Deviations
Patients with a hyperphoria or intermittent hypertropia often have inadequate vertical vergence capability. However, vertical fusional vergence ability may be greater than normal if the patient has been compensating adequately for the deviation for a long time. Patients with a hyperdeviation often demonstrate a head tilt, which can assist them in compensating for the deviation. In addition to the commonly experienced symptoms of binocular vision disorders listed above, patients with a vertical deviation may complain of car or motion sickness.18 Patients with a primary vertical deviation (i.e., one that exists even under fused conditions, as a fixation disparity, defined below) can benefit from prescription of vertical prism. A primary vertical deviation can be differentiated from a secondary one by means of associated phoria testing (described below).
Methods of Determining a Prism Prescription
Sheard’s Criterion for Exodeviations
When prescribing prism for patients having a basic exodeviation or convergence insufficiency, use of Sheard’s criterion has been recommended.19 Sheard’s criterion specifies that the opposing vergence range (convergence or BO amplitude in the case of exophoria) should be at least twice the amount of the phoria.20 For example, a patient with a 10Δ exophoria would need at least 20Δ of convergence, measured at the same working distance, to fulfill Sheard’s criterion. Research by Sheedy and Saladin.21 found that Sheard’s criterion was the best discriminator between their symptomatic and asymptomatic subjects with exophoria. Calculation of Sheard’s criterion ideally should use the convergence amplitude blur value, rather than the break value.21 However, if the patient has no blur point during convergence amplitude testing, the break value can be used. A convenient formula for calculating how much BI prism is needed for a patient with exophoria is: [2(exophoria) – BO blur value]/3.22 For example, if a patient has 10Δ exophoria at distance and a BO vergence range at distance of 14/16/4 (blur/break/recovery), the above formula suggests a prism prescription of [2(10) – 14]/3 = 2Δ. Lenses containing a total of 2Δ BI should then enable the patient to meet Sheard’s criterion, because the phoria measured through the prism would be 8Δ and the BO blur value should increase to 16Δ.
Saladin’s 1:1 Rule for Esodeviations
Saladin proposed the 1:1 rule for determining a BO prism prescription for patients with esophoria.19 This guideline applies to patients either with an esodeviation at distance only, or an esodeviation at both distance and near point. The rule states that the patient’s BI vergence recovery value should be at least equal to his or her esophoria. Prism can be prescribed to equalize these values.19 The formula to determine prism amount is: BO prism = (esophoria – BI recovery)/2.23 If the patient demonstrates a negative recovery (i.e., on BI vergence testing, fusion is not regained as the BI prism power is reduced, until some amount of BO prism is introduced), a negative number must be used in the equation. For example, if the patient has 6Δ esophoria at distance and the BI vergence range at distance is ×/2/ – 2 (blur/break/recovery), the 1:1 formula suggests a prism prescription of [6-(-2)]/2 = 4Δ. Thus, lenses containing a total of 4Δ BO should reduce this patient’s phoria measured through them to 2Δ eso and the recovery value should become 2Δ BI.
Associated Phoria – for Vertical Deviations
Associated phoria refers to the amount of prism that eliminates a patient’s fixation disparity. Fixation disparity is a slight misalignment of the visual axes (generally <0.25Δ) existing under fused conditions. Measurement of such a small misalignment cannot be done by cover testing, but requires a special device. Mallett24,25 developed one of the first measuring devices for associated phoria, in which there is a central fused target with two adjacent polarized targets. One polarized target is seen by each eye when viewed through polarized filters, enabling detection of fixation disparity.24,25 If a patient manifesting a vertical phoria or intermittent vertical strabismus (e.g., on cover testing) observes misalignment (one line higher than the other) of the horizontally oriented polarized lines on the fixation disparity testing device, the patient is manifesting a primary vertical deviation and is likely to benefit from a prism correction. Eskridge and Rutstein26 have demonstrated that the vertical associated phoria (the prism that reduces fixation disparity to zero) is an appropriate value to prescribe for patients with a symptomatic vertical deviation.
In clinical practice, if a patient has a vertical deviation with both distance and near fixation, the associated phoria should be evaluated at both distances. Commercially available testing devices include the Wesson Card (near only), Bernell Near Point Analysis Slide, and Bernell Fixation Disparity at Far Slide (all available from Bernell, Mishawaka, IN; www.bernell.com) (Figs. 3, 4 and 5). The latter two slides should be presented to the patient on an illuminated Bernell Test Lantern. To begin the test, the patient should wear polarized filters over his or her habitual (or proposed) lens correction. The patient is then asked to focus on the physically aligned polarized targets (arrows or thin lines) and make sure both are seen. Absence of one eye’s line indicates suppression, and the test cannot be completed unless the suppression can be broken by having the patient blink or tap the target. If the patient sees the targets aligned (i.e., no fixation disparity), no prism correction is indicated. If, however, the patient observes a misalignment of the horizontally oriented lines, prism of the appropriate base is placed before one eye to produce alignment. For example, if the right eye’s polarized line appears to be lower, the patient is manifesting right hyper fixation disparity, and BD prism is needed before the right eye. Starting with 0.5Δ or 1Δ, gradually increase prism powers (in 1-Δ increments) until the patient perceives the polarized lines to be aligned and stable (i.e., consistent alignment can be maintained both while the eyes remain open and immediately following a blink).27 The prism power that produced this alignment can then be prescribed for the patient.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


