Orbital Anatomy and Its Clinical Applications
Deborah D. Sherman
Cat N. Burkat
Bradley N. Lemke
The clinician must have a detailed knowledge of orbital anatomy to understand the structural disarrangements in orbital disease and to employ appropriate medical and surgical procedures. This chapter discusses orbital anatomy with emphasis on those aspects that are important in orbital disease.
DIMENSIONS
The bony orbit is a pear-shaped structure closely resembling a four-sided pyramid that becomes three-sided near the apex (Fig. 1). The bony orbit has a volume of approximately 30 cc. The adult orbital margin is approximately rectangular with a horizontal dimension of 40 mm and a vertical dimension of 35 mm. The widest dimension of the orbit is 1 cm behind the anterior orbital rim. The medial walls are separated by 25 mm in the average adult and are roughly parallel.1 The length of the medial orbital wall from the anterior lacrimal crest is 45 to 50 mm, whereas the lateral wall from the rim to the superior orbital fissure measures 40 mm. The adult lateral orbital walls are angled 90 degrees from each other, or 45 degrees in the anteroposterior direction. The divergent axis of each orbit thus becomes half of 45 degrees or 22.5 degrees (Fig. 2). The eyes tend to diverge in accordance with their bony surroundings, as seen in persons with acquired visual loss, under general anesthesia, or in death. Because of the continuous need for torsion of the globe away from the orbital axis, it is not surprising to find that the medial is the thickest of the rectus muscles. The lateral orbital rim is approximately at the level of the equator of the globe.
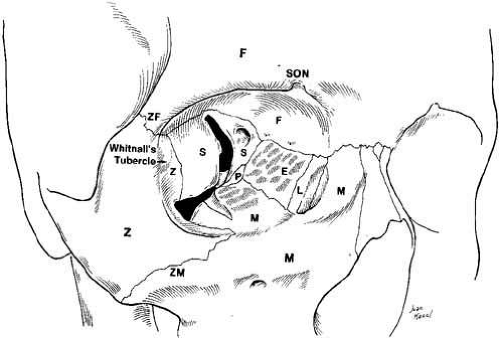 Fig. 1 Anterior view of the orbit. The walls are made up of seven bones; the roof consists of the sphenoid (S) and the frontal bone (F); the lateral wall consists of the sphenoid (S) and zygomatic bones (Z); the floor consists of the maxilla (M), the palatine (P), and zygomatic bones (Z); the medial wall consists of the sphenoid (S), maxilla (M), ethmoid (E), lacrimal bones (L), and supraorbital notch (SON). |
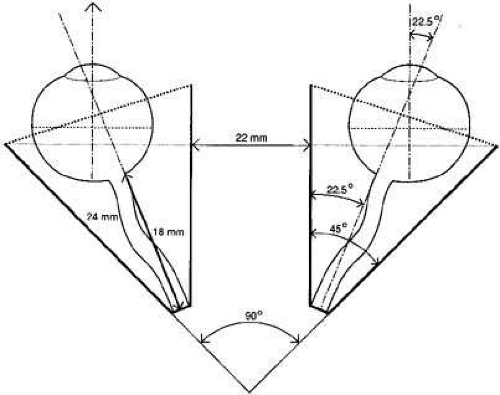 Fig. 2 Diagram of horizontal section through orbits. Medial walls are roughly parallel and lateral walls diverge 45 degrees. Thus, the orbital axis diverges 22.5 degrees away from midline. |
The intraorbital optic nerve measures 25 mm, on the average, between the back of the globe and the entrance into the optic foramen, but the distance between these structures is only 18 mm. This 7 mm of slack in the optic nerve results in a gentle curve with a convexity directed inferotemporally in the orbit. This degree of play in the nerve allows free eye movement and affords a margin of safety in proptotic states. Approximate measurements of the adult orbit are outlined in Table 1.
TABLE 1. Adult Orbital Dimensions | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
ORBITAL RIM
The zygomatic bone forms the lateral orbital margin. It serves as an orbital protector or “facial buttress” that can withstand significant trauma without fracturing. When fractured, steps may be palpable inferiorly at the zygomaticomaxillary suture and superolaterally at the zygomaticofrontal suture. The frontal bone comprises the superior orbital margin and extends both laterally and medially to form portions of those borders (see Fig. 1). In the newborn, the supraorbital rim is sharp; it remains so in the female but becomes rounded with development in the male. In most skulls, the superior rim at the junction of its medial one-third is indented by a supraorbital notch, where the supraorbital nerve and artery pass to innervate the forehead and frontal sinus. In approximately 25% of skulls, the frontal bone covers these structures, forming a foramen.
The medial orbital rim is formed anteriorly by the maxillary bone rising to meet the maxillary process of the frontal bone. The lacrimal sac fossa complicates the medial rim by indenting the bone and forming anterior (maxillary bone) and posterior (lacrimal bone) crests. Thus, Whitnall2 likened the definable orbital rim to a single coil of an undulating spiral. The inferior orbital rim is comprised of the maxillary and zygomatic bones, and inferior to the rim exits the infraorbital nerve and artery.
ORBITAL WALLS
The orbital walls are embryologically derived from neural crest cells. Ossification of the orbital walls is completed by birth, except at the orbital apex. The lesser wing of the sphenoid is initially cartilaginous, unlike the greater wing of the sphenoid and other orbital intramembranous bones.
The walls are made up of seven bones (see Fig. 1).
The orbital roof is principally comprised of the frontal bone. Its progressive concavity with growth reflects molding of the globe. Posteriorly, the roof remains flat and receives a 1.5-cm contribution from the lesser wing of the sphenoid bone as the roof tapers into the anterior clinoid process of the lesser sphenoid. At an angle of about 45 degrees from the midline, the optic nerve enters the optic foramen located in the lesser wing of the sphenoid at the orbital apex. Anteromedially, the small trochlear fossa is found, and the large lacrimal gland fossa is seen laterally. The roof is usually strong, and only rarely will blunt ocular trauma disrupt it, in contrast to the commonly seen orbital floor fracture.
The lateral orbital wall is bordered by the superior and inferior orbital fissures. The anterior borders are formed by the frontozygomatic and the zygomaticomaxillary sutures. Posteriorly, the greater wing of the sphenoid is alone in forming the lateral wall but is met anteriorly by the zygoma and the lateral angular (zygomatic) process of the frontal bone. Near the suture between the frontal and sphenoid bones, a meningeal foramen conducting the recurrent meningeal artery off the middle meningeal artery may be found. This artery anastomoses the external carotid circulation with the internal carotid system via the lacrimal artery from the ophthalmic artery. Approximately 4 to 5 mm behind the lateral orbital rim at its midpoint, approximately 1cm inferior to the frontozygomatic suture, is the lateral orbital tubercle of Whitnall.3 The lateral canthal ligament, the lateral rectus check ligament, the lateral horn of the levator aponeurosis, the suspensory ligament of the lower lid (Lockwood’s ligament), the orbital septum, and the lacrimal gland fascia attach at Whitnall’s tubercle. Whitnall’s tubercle is usually the location for reattachment during the lateral tarsal strip or other lateral canthal procedures. The zygoma thickens inferiorly and forms the anterior loop of the inferior orbital fissure. This thicker zygoma also separates the orbit from the buccal fat-pad.
Posterior and lateral to the lateral orbital wall lies the temporalis muscle, which is firmly adherent to the bony temporal fossa. The frontal process of the zygomatic bone and the zygomatic process of the frontal bone are quite thick and protect the globe from lateral trauma. Behind this facial buttress area, the posterior zygomatic bone and the orbital plate of the greater wing of the sphenoid is thinner, making the zygomaticosphenoid suture a convenient breaking point for bone removal during lateral orbitotomy. The zygomaticofacial and the zygomaticotemporal canals transmit like-named branches of the zygomatic nerve and vessels through the lateral orbital wall to terminate in the cheek and temporalis region, respectively. These vessels are often encountered as the surgeon dissects the temporalis muscle during a lateral orbitotomy. Posterior to the thin zygomaticosphenoid suture the lateral orbital wall again begins to thicken. At this point it meets the temporal bone, which forms the lateral wall of the cranium (Fig. 3). When performing a lateral orbitotomy, the surgeon must be aware that a distance of approximately 12 to 13 mm separates the posterior aspect of the osteotomy from the middle cranial fossa. In females, however, this distance may be 5 to 6 mm shorter.4
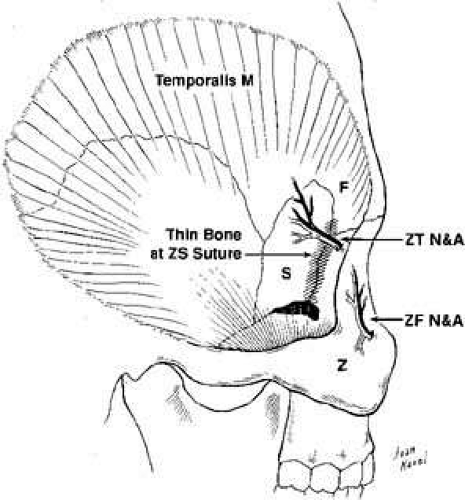 Fig. 3 Posterior lateral view of temporalis fossa showing the thin zygomaticosphenoid suture, which is a convenient breaking point in a lateral orbitotomy. Also shown are the zygomaticofacial (ZF) and the zygomaticotemporal (ZT) canals, which transmit like-named branches of the zygomatic nerve and vessels. |
The floor is the shortest of the orbital walls and is shaped like an equilateral triangle. A line passing through the axis of the inferior orbital fissure forms the lateral border (see Fig. 1). The medial border can be defined with anterior and posterior extensions of the maxillary-ethmoidal suture. The orbital plate of the maxillary bone comprises nearly the entire floor with small contributions from the palatine bone posteriorly and from the zygoma anterolaterally. The posterior infraorbital groove becomes a canal anteriorly as the nerve passes through the infraorbital foramen (see Fig. 1). In childhood the infraorbital foramen is found immediately below the orbital margin, but as the face grows into adult size, the foramen migrates 6 to 10 mm below the orbital rim. The floor remains strong lateral to the infraorbital nerve but becomes thin medially with maxillary sinus expansion. This unsupported dome of maxillary sinus is where the floor usually fractures with trauma, often causing hypesthesia of the infraorbital skin, the lateral tip of the nose, and the anterior superior gingiva. The nasolacrimal duct lies at the anteromedial orbital floor and travels inferiorly and posteriorly 2 cm along the lateral wall of the nose before exiting into the inferior meatus.
The medial orbital wall is composed, from anterior to posterior, by the frontal process of the maxilla, the lacrimal bone, the ethmoid bone, and the lesser wing of the sphenoid bone. The thinnest portion of the medial wall is the lamina papyracea, which covers the ethmoid sinuses posterior to the maxillary bone (see Fig. 1). It can be breached by inflammatory and neoplastic disease that originates in the ethmoid air cells as well as by dissection during surgery. In children, infections of the ethmoid sinuses commonly extend through the lamina papyracea as a result of dehiscences or venous channels to cause orbital cellulitis and proptosis. The medial wall becomes thicker posteriorly at the body of the sphenoid and again anteriorly at both the posterior lacrimal crest of the lacrimal bone and the anterior lacrimal crest of the maxillary bone. The many bullae of ethmoid pneumatization appears as a honeycomb pattern beneath the ethmoidal orbital plate. This supportive structure, in part, explains why the medial wall fractures less often than the thicker orbital floor. The frontoethmoidal suture is important in orbital bony decompression or medial exploration because it marks the roof of the ethmoid sinus, and bony dissection superior to this suture line may expose the dura of the frontal lobe. The anterior and posterior ethmoidal foramina conveying branches of the ophthalmic artery and the nasociliary nerve are located at the frontoethmoidal suture 24 mm and 35 mm posterior to the anterior lacrimal crest, respectively (see Fig. 1). The location of these foramina is important when the surgeon gives an anterior ethmoidal nerve block for local anesthesia during medial orbitotomy.
NASAL AND PARANASAL SINUSES
Knowledge of nasal and paranasal sinus anatomy improves our understanding of surgical relationships to the orbit, as well as endonasal anatomy. Furthermore, when lacrimal surgery is performed using the endonasal approach, the surgeon must be familiar with this anatomy.
Each paranasal sinus is named for the bone into which it originally invaginates during fetal life. The bones forming the orbital floor, roof, and medial wall are pneumatized by air sinuses arising from and maintaining communication with the nasal cavity. Ethmoid bullae are particularly exuberant in their expansion and may pneumatize the orbital plate of the frontal bone, and even develop as frontal sinuses. The maxillary processes contribute the maxillary bone portion of the lateral nasal wall and the majority of the nasal floor, the posterior or secondary palate. The ethmoid box, derived from the embryologic nasal frontal process, spans the roof of the nasal cavity, arching from the superior lateral nasal walls (see Fig. 4).
 Fig. 4 Axial computed tomography demonstrating the ethmoid (E) and sphenoid (S) sinuses. (Courtesy of June M. Unger, MD, University of Wisconsin.) |
The nasal cavity is bisected anteriorly by the cartilage and septum, which joins the vomer, a bony vertical plate of ethmoid, posteriorly. Laterally, the nasal wall is thrown into three or more horizontal ridges termed turbinates, with spaces below each with corresponding names (Fig. 5). The inferior turbinate is the largest ridge, whereas the progressively smaller and more posterior middle, superior, and supreme turbinates (sometimes present) are outcroppings of the ethmoid bone. The large cartilaginous anterior dilatation of the nose is the nasal vestibule. When the exterior nares are dilated by a nasal speculum, the inferior turbinate and inferior meatus can be seen by tilting the blades to look along the nasal floor. The middle turbinate and nasal atrium are seen, if the examiner does not forcibly rotate the blades. Because the atrium wall is convex medially, an external dacryocystorhinostomy site located at the anterior or inferior tip of the middle turbinate may not be directly visualized. A dacryocystorhinostomy achieved by the endoscopic laser–assisted approach is usually more inferior and posterior to the routine external site.5 The nasolacrimal duct drains under the inferior turbinate, whereas the frontonasal duct from the frontal sinus drains into the anterior middle meatus. Within the middle meatus posterior to the atrium lies a curvilinear ridge, the uncinate process, with the hiatus semilunaris depression behind, which houses the ostium of the maxillary sinus (see Fig. 5).6
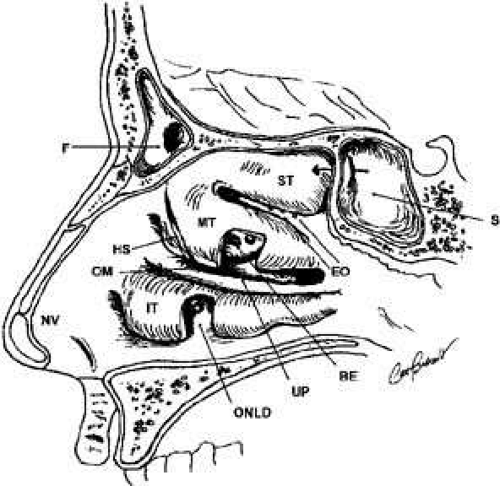 Fig. 5 Endonasal sagittal view. Each meatal space is named for the turbinate that lies immediately above. (ST, superior turbinate; OM, ostium of maxillary sinus; MT, middle turbinate; NV, nasal vestibule; IT, inferior turbinate; ONLD, ostium of nasal lacrimal duct; BE, bulla ethmoidalis; S, sphenoid sinus; HS, hiatus semilunaris; F, frontal sinus; UP, uncinate process; EO, ethmoid ostia) |
The paranasal sinuses more than double the nasal chamber volume. The vascular mucoperiosteum of the nose is carried into the sinuses, where densely populated cilia rhythmically beat mucus toward the ostium. Acute inflammation of the nasal and paranasal mucoperiosteum can result in swelling severe enough to occlude the sinus ostia, and thus purulent sinusitis may result. Chronic sinusitis may lead to permanent occlusion of the ostia, which can result in mucocele formation.
The maxillary sinus is the largest of the paranasal sinuses (15 cc). This sinus roof is the orbital floor that declines from the medial wall to the lateral wall at an angle of approximately 30 degrees. Like the medial sinus roof, the lateral wall of the sinus is also thin and subject to fracture with zygomatic displacement. The maxillary sinus drains into the middle meatus through an ostium located near the level of the orbital floor, thus orbital tissues that are displaced in surgery or trauma may obstruct the ostium. The pterygoid-palatine space lies posterior to the maxillary sinus with the internal maxillary artery intimately related to the posterior sinus wall.
As mentioned previously, the ethmoidals are the most exuberant growing sinuses and may pneumatize the frontal, sphenoid, palatine, and lacrimal bones. The ethmoid sinuses are shaped like a box slightly wider posteriorly where it articulates with the sphenoid (see Fig. 4). The anterior and middle ethmoidals drain into the middle meatus, whereas the posterior cells may drain into the superior meatus. The roof of the orbit slopes down as it travels medially, and this slope continues at the frontoethmoidal suture to become the ethmoid roof (fovea ethmoidalis), and finally to overlie the nasal cavity as the cribriform plate. The crista galli bisects the cribriform plate above and continues below as the vertical nasal plate (vomer). Three to fifteen air cells expand from each lateral border to the cribriform plate, and the air cell masses convolute medially to form the middle, superior, and supreme (if present) turbinates. The surgeon should be aware of the anatomic relationship of anterior ethmoid air cells to the lacrimal sac fossa when performing external dacryocystorhinostomy. Blaylock7 evaluated computed tomographic scans of 190 orbits with normal ethmoid anatomy and found that in 93% of the orbits, the cells extended anterior to the posterior lacrimal crest, with 40% entering the frontal process of the maxilla.
The frontal sinus is not well developed or radiographically evident until about the 6th year of life. Frontal sinus expansion continues until early adulthood and attains greater proportions in the male. The frontal sinus lies deep to the superior orbital rim and drains into the middle meatus via the frontonasal duct. Each sinus is a single chamber with intrasinus septae, which give it a scalloped appearance radiologically. The frontal sinus is a common site for mucocele development.
The sphenoid sinus also continues to grow until adulthood with varying degrees of pneumatization. It drains into the sphenoethmoid recess under the superior turbinate. In the instance where the sphenoid body is fully pneumatized, only sinus mucoperiosteum, a thin layer of bone, and periosteum separate the respiratory tract from the overlying internal carotid artery, the cavernous sinus, and branches of the trigeminal nerve.
ORBITAL APEX: SUPERIOR ORBITAL FISSURE, INFERIOR ORBITAL FISSURE
The orbital apex contains a plethora of vital structures. A large number of arteries, veins, and nerves pass through several significant foramina. The superior orbital fissure is a transverse notch between the greater and lesser wings of the sphenoid bone that descends medially (see Fig. 1). Although the shape of the superior orbital fissure is variable, the superior portion is usually narrower where the lacrimal, frontal, and trochlear nerves pass (Fig. 6). The middle meningeal artery anastomosis with the ophthalmic artery may enter here, if not through its own foramen, more anteriorly in the roof. Most of the venous drainage from the orbit and the globe flow through the superior orbital fissure to the cavernous sinus. Other structures passing through the superior orbital fissure within the annulus of Zinn include the superior and inferior divisions of the third cranial nerve, the sixth cranial nerve, and the nasociliary branch of the ophthalmic trigeminal nerve (Fig. 6).
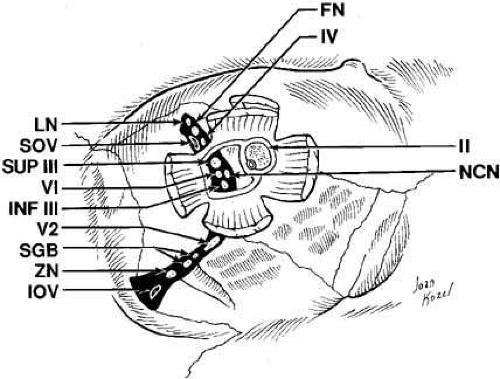 Fig. 6 Orbital apex with nerves coursing through foramina. (LN, lacrimal nerve; NCN, nasociliary nerve; FN, frontal nerve; VI, abducens nerve; IV, trochlear nerve; INF III, inferior division of cranial nerve III; SOV, superior ophthalmic vein; II, cranial nerve II; SUP III, superior division of cranial nerve III; IOV, inferior ophthalmic vein; ZN, zygomatic nerve; V2, V2 nerve; SGB, sphenopalatine ganglion branches) |
Radiographic enlargement of the superior orbital fissure may accompany pathologic processes, such as aneurysm, meningioma, chordoma, pituitary adenoma, or tumors of the orbital apex.8 When idiopathic inflammation preferentially involves the superior orbital fissure, the Tolosa-Hunt syndrome (painful ophthalmoplegia) results. The nerves to the extraocular muscles may be affected by the inflammation as they pass through the superior orbital fissure. The pain in this syndrome results from the inflammatory involvement of the first division of the trigeminal nerve. Interference with venous drainage through the inflamed fissure can cause stasis edema of the lids and orbits.
Medial to the superior orbital fissure lies the optic foramen (see Fig. 1) within the lesser wing of the sphenoid, which conveys the optic nerve and the ophthalmic artery. The optic canal attains adult dimensions by age 3 and is symmetric in most persons. Because of the shift in the position of the ophthalmic artery relative to the optic nerve, the canal is horizontally oval posteriorly and more vertically oval anteriorly. In the adult the optic canal is 8 to 10 mm long and 5 to 7 mm wide, and the optic foramen normally measures 6.5 mm in diameter. Optic foramen enlargement is commonly seen with optic nerve gliomas. A foramen that measures 7 mm in diameter is usually abnormal. Among young children whose optic canals have not yet reached adult dimensions, the size of both foramina should be compared. In these patients, a foramen that is 6.5 mm in diameter and at least 1 mm larger than the contralateral foramen is considered abnormal. The optic canal is separated from the superior orbital fissure by the bony optic strut, the inferior root of the lesser wing of the sphenoid bone (see Fig. 1). It joins the body of the sphenoid to its lesser wing and separates the optic foramen from the superior orbital fissure. This thin optic strut forming the lateral and inferior borders of the optic canal is subject to deformation by optic nerve gliomas, infraclinoid aneurysms, or intracanalicular spread of an intracranial chiasmal tumor.9 An “optic neuritis” that is progressive over months or years should suggest an intracanalicular meningioma.10
Other orbital diseases may cause enlargement of the optic canal. Benign arachnoidal hyperplasia extending beyond the tumoral glial tissue can enlarge the optic foramen. Rarely, a fungal infection, such as aspergilloma, or a bacterial infection, such as a syphilitic gumma or tuberculoma, can settle in the optic canal and mimic a neoplasm. Enlargement of the canal can also occur in sarcoidosis, neurofibroma, arachnoidal cyst, and chronic hydrocephalus. Fibrous dysplasia and ossifying fibromas of the sphenoid bone can involve the canal and narrow its dimensions.10
The infraorbital fissure is a 20-mm bony defect bounded by the sphenoid, zygomatic, maxillary, and palatine bones, and lies between the lateral orbital wall and orbital floor (see Fig. 1). It transmits the second (maxillary) division of the fifth cranial nerve, the zygomatic nerve, small branches from the sphenopalatine ganglion, and branches of the inferior ophthalmic vein leading to the pterygoid plexus (see Figs. 1, 6, and 19). Posterior to the inferior orbital fissure, the foramen rotundum pierces the greater sphenoid wing carrying the maxillary division of the trigeminal nerve forward to the orbit. Arriving with the maxillary nerve is the terminal branch of the internal maxillary artery. The structures enter the infraorbital sulcus to become the infraorbital nerve and artery, which then traverse the infraorbital canal and foramen to carry sensation to the lower lid, cheek, upper lip, and upper anterior gingiva. It is important to identify this neurovascular bundle during midface suborbicularis oculi fat lifts to avoid inadvertent injury.
The inferior orbital fissure extends more anteriorly than the superior orbital fissure, ending about 20 mm from the anterior orbital rim. This structure serves as a posterior landmark in the surgical subperiosteal dissection along the orbital floor. Immediately beneath the infraorbital fissure lies the pterygoid space with the temporalis fossa laterally; blunt trauma to the temporalis muscle can result in orbital hemorrhage via this connection (see Fig. 3).
Orbital Soft Tissues
The soft tissues contained within the bony walls of the orbit and limited anteriorly by the orbital septum are discussed in this section in the following order: orbital septum, periorbita, orbital fascia, orbital fat, lacrimal gland, extraocular muscles, levator palpebrae superioris, Müller’s muscle, optic nerve and meninges, globe, orbital nerves, orbital vessels, and orbital lymphatic drainage.
Orbital Septum
The orbital septum is the anterior soft tissue boundary of the orbit and acts as a physical barrier against pathogens and maintains the normal posterior position of the orbital fat-pads. It is a thin, multilayered sheet of fibrous tissue derived from the mesodermal layer of the embryonic eyelid. The septum is covered by a thin layer of preseptal orbicularis and skin and originates from the superior and inferior orbital rims at a thick, white fibrous line called the arcus marginalis to insert onto the eyelid retractors. Medially, the septum covers the posterior aspect of Horner’s muscle as it inserts along the posterior lacrimal crest. Laterally, the septum fuses with the lateral canthal tendon and lateral horn of the levator aponeurosis to attach to the lateral orbital rim11 (see Fig. 7).
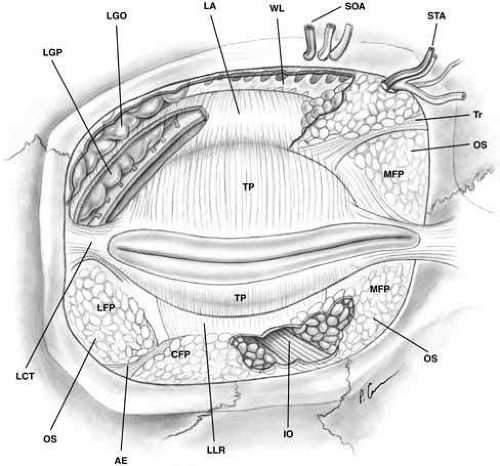 Fig. 7 Anterior view of orbital septum and related structures. The medial deep orbital insertion of the orbicularis muscle carries the orbital septum behind it. The septal attachments to the levator aponeurosis in the upper lid and inferior tarsus in the lower lid are also demonstrated, as well as the anatomic relationships to the structures of the upper lid. (AE, arcuate expansion of the inferior oblique; CFP, central fat-pad; IO, inferior oblique muscle; LA, levator aponeurosis; LCT, lateral canthal tendon; LFP, lateral fat-pad; LGO, lacrimal gland orbital lobe; LGP, lacrimal gland palpebral lobe; LLR, lower lid retractors; MCT, medial canthal tendon; MFP, medial fat-pad; OS, orbital septum; STA, supratrochlear artery, nerve, vein; SOA, supraorbital artery, nerve, vein; TP, tarsal plate; Tr, trochlea; WL, Whitnall’s ligament) |
In the lower eyelid, the septum inserts onto the inferior border of tarsus after joining with the lower lid retractors 4 to 5 mm below the tarsus. The superior orbital septum does not insert onto the superior tarsal plate because of the intervening levator aponeurosis; rather it inserts on the aponeurosis about 10 mm above the superior eyelid margin, or 2 to 5 mm above the superior tarsal border in non-Asians11 (see Fig. 8). In Asian lids, the orbital septum fuses to the levator aponeurosis at a level below the superior tarsus, allowing preaponeurotic fat to prolapse inferior and anterior to tarsus; in the lower lid, it may fuse directly to the inferior tarsal border rather than joining with the retractors. An absent or lower lid crease in Asian eyelids may be due to this fat protrusion and other subcutaneous fat tissue that inhibits levator fibers from inserting into the subdermal skin.12
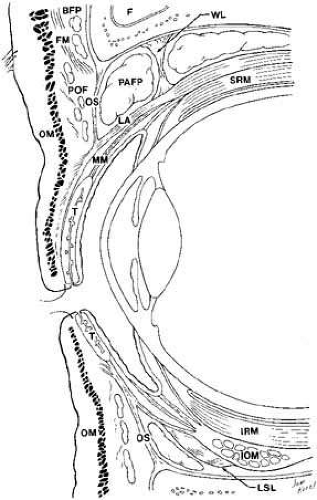 Fig. 8 Parasagittal section to show anterior orbital structures. (F, frontal sinus; SRM, superior rectus muscle; FM, frontalis muscle; MM, Müller’s muscle; BFP, brow fat-pad; T, tarsus: POF, postorbicularis fascia; OM, orbicularis muscle; OS, orbital septum; LSL, Lockwood’s suspensory ligament; PAFP, preaponeurotic fat-pad; IOM, inferior oblique muscle; WL, Whitnall’s ligament; IRM, inferior rectus muscle; LA, levator aponeurosis) |
The septum may attenuate with age allowing orbital fat to herniate forward, requiring blepharoplasty. In performing levator surgery or blepharoplasty the preaponeurotic fat is encountered just posterior to the septum. Loose areolar tissue, termed the suborbicularis fascia, lies immediately anterior to the septum13 and shares the same plane as the eyebrow retro-orbicularis oculi fat and malar fat-pads further from the eyelid margins.
Periorbita
The periorbita is the periosteal covering of the orbital bones. The periorbita is firmly attached at the suture lines, the foramina, the fissures, the arcus marginalis, and at the posterior lacrimal crest. Elsewhere, it is loosely adherent to the bone and may be easily separated from the bone by the surgeon or by accumulations of blood or pus. Posteriorly, the periorbita is continuous with the dura of the optic nerve, where the dura is fused to the optic canal. Likewise, the superior orbital fissure is bound by thickened periorbita, which also blends with intracranial dura. Anteriorly, the periorbita is continuous with the orbital septum, which partitions the lids from the anterior orbital tissues. The periorbita is continuous with the frontal, zygomatic, malar, and nasal periostea, and is also continuous with the bones of the sphenopalatine and temporal fossa through the inferior orbital fissure. The periorbita lines the lacrimal fossa, and an extension—the lacrimal fascia—covers the lacrimal sac between the anterior and posterior lacrimal crest (Fig. 9).
 Fig. 9 Shaded areas demonstrate dense attachment sites for the periorbita. |
The periorbita is extensively vascularized on both its bone and soft tissue sides. These vessels are interconnected so that the periosteum does not serve as a vascular barrier area.14 It is supplied by twigs from regional branches of the sensory intraorbital trigeminal nerve. The periorbita has a dense layer adjacent to bone and a more loosely packed layer next to the orbital contents. It serves as a membrane that can restrain periosteal hematomas and temporally provide resistance to the spread of infections and tumors from the sinuses and bones into the orbit. However, the periorbita can be eventually dissolved by these processes. In children, granulocytic sarcoma has a predilection for the periosteum and bones of the orbit.10 The periorbita can often be the only separation between the orbital contents and dermoids or mucoceles. The potential space between the periorbita and orbital bones provides a convenient plane of dissection to many orbital tumors or for removal of soft tissues in an exenteration.
Orbital Fascia
The fibrous tissue organization within the orbit may be divided into three parts: the fascia covering the globe, the coverings of the extraocular muscles, and the check ligament extensions of the extraocular muscle fascia that extend to the surrounding bone and eyelids. Extensive work by Koornneef,15 using a thick serial section technique has shown the orbital fascia to be complex and highly organized.
Tenon’s capsule, the fascia bulbi, is a fibrous membrane that extends from the posterior aspect of the globe to fuse anteriorly with the conjunctiva slightly posterior to the corneoscleral junction. It is thinnest at the entrance of the optic nerve. It is closely applied to the globe but may be lifted some distance from it to reveal a fine netlike character. The resultant space between these structures is termed Tenon’s space. Externally, Tenon’s capsule is joined to the network of fibrous septa dividing the lobules of orbital fat. Thus, the globe is loosely related to the surrounding orbital fat, and freedom of movement is afforded by elasticity in the septa and fat. Tunnel-like openings in Tenon’s fascia allow the extraocular muscles to pass from the orbital fat into the Tenon’s space to insert onto the sclera (see Fig. 10). In the areas of these openings, Tenon’s capsule fuses with the intermuscular septal fascia. Orbital implants used after enucleation are placed either within this fibrous Tenon’s capsule or posterior to it within the muscle cone. Inflammatory pseudotumor may involve Tenon’s capsule and cause a tenonitis that can produce proptosis. B-scan ultrasonography can help identify this type of periocular inflammation. Posterior geographic scleritis and intense choroiditis may also cause secondary inflammations of Tenon’s capsule.10
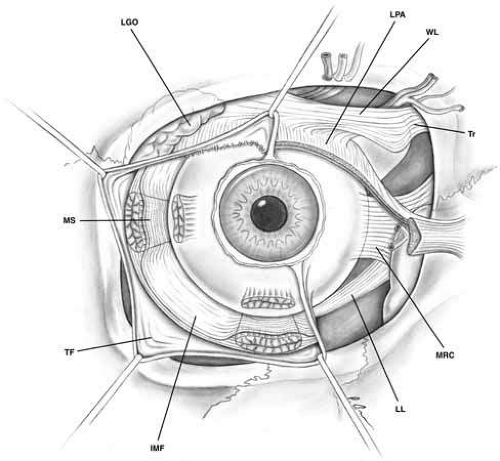 Fig. 10 Tenon’s fascia, anterior view. Tenon’s capsule covers the globe and extends onto the muscular fascia. Tenon’s fascia is denser between the muscles and thinner toward the posterior aspect of the globe. The intermuscular septal fascia connecting the muscular sheaths is demonstrated beneath the reflected Tenon’s fascia. (IMF, intermuscular fascia; LGO, lacrimal gland orbital lobe; LL, Lockwood’s ligament; LPA, levator palpebrae aponeurosis; MRC, medial rectus check ligament; MS, muscular sheath; TF, Tenon’s fascia; Tr, trochlea; WL, Whitnall’s ligament) |
The muscular fascia ensheathes the extraocular muscles and extends between them. These muscle fascial sheaths are thin posteriorly but become much denser anteriorly. The muscular sheaths connect from their extraconal surface to the orbital walls and from their intraconal surface to the fibrous septae dividing the intraconal fat lobules.16 The bulbar side of the muscular sheath is thinner than the external aspect that forms the check ligaments, yet it is thicker than the posterior portion of Tenon’s capsule.17 Smooth muscle fibers are scattered throughout the membrane and are innervated by the sympathetic nervous system.2
The muscles are connected to the surrounding fascia throughout the anterior one-third of their lengths, especially where they insert onto the globe, which prevents their retraction far posteriorly in the orbit if lost during strabismus operation (unless the muscle has been dissected free). These attachments account, in part, for the persistent movement of the eye socket after enucleation when muscles have not been specifically sewn to the implant. As noted above, each extraocular muscle sheath sends extensions to the orbital walls. Anteriorly, they are especially prominent and are called check ligaments. The most developed check ligaments are those of the medial and lateral rectus muscles (see Figs. 10 and 11). The lateral check ligament is the strongest and inserts primarily on the posterior aspect of Whitnall’s lateral orbital tubercle with lesser extensions to the lateral conjunctival fornix and lateral orbital septum. The medial check ligament inserts on the bone behind the posterior lacrimal crest and to the medial orbital septum, caruncle, and plica semilunaris. The superior rectus muscle sheath is joined anteriorly with that of the levator palpebrae superioris by means of an intermuscular fascia.18 The superior transverse Whitnall’s ligament may serve as a superior check ligament to limit elevation by the upper eyelid19 (see Figs. 10 and 11). The fused inferior rectus and inferior oblique muscle sheaths send fascial connections to the inferior periorbita, which may also have some checking function.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


