Chapter 9 The Surgical Management of Hyperthyroidism
Introduction
Primary hyperthyroidism is a syndrome manifested by signs and symptoms of hypermetabolism and excess sympathetic nervous system activity that results from excess synthesis and secretion of thyroid hormone by the thyroid gland. The overall prevalence of hyperthyroidism is 1.3% in the U.S. population. It occurs in 2% of women and 0.5% of men, and its prevalence can be as high as 5% in older women.1 The term hyperthyroidism is distinct from thyrotoxicosis, which is a syndrome that results from excessive thyroid hormone that may come from other sources in addition to the thyroid gland. Patients with subacute, painless, or radiation-induced thyroiditis; excess thyroid hormone ingestion; struma ovarii; and functional metastatic thyroid cancer are examples of those who have thyrotoxicosis that is not attributed to hyperthyroidism. This chapter focuses on the clinical presentation, diagnosis, and surgical management of hyperthyroidism from Graves’ disease, toxic multinodular goiter, and a solitary toxic nodule (see also Chapter 3, Thyroid Physiology and Thyroid Function Testing).
The excess synthesis and secretion of thyroid hormone that occur in patients with hyperthyroidism may produce a variety of clinical manifestations and findings on physical examination (Boxes 9-1 and 9-2). Elderly patients are more likely to present with subtle symptoms of thyrotoxicosis such as asthenia, fatigue, and weakness, a syndrome referred to as apathetic hyperthyroidism. Elderly patients are also more likely to have cardiovascular manifestations of hyperthyroidism such as atrial fibrillation, ischemic heart disease, and congestive heart failure.
Box 9-1 Symptoms and Manifestations of Hyperthyroidism
The best screening test for hyperthyroidism is a serum thyrotropin (TSH) level (see Chapter 3, Thyroid Physiology and Thyroid Function Testing). With the rare exception of a TSH-secreting pituitary tumor, patients with hyperthyroidism will have a decreased serum TSH level. Patients with a low serum TSH level should have a free T4 (FT4) and a free T3 (FT3) level measured to help determine the degree of hyperthyroidism. Patients with a low serum TSH level and normal FT4 and FT3 levels are defined as having subclinical hyperthyroidism. A FT3 level is important to make a diagnosis of “T3 thyrotoxicosis” in a patient with a suppressed serum TSH level and a normal FT4 level. In most patients, T3 thyrotoxicosis is an early manifestation of Graves’ disease (see also Chapter 5, Hyperthyroidism: Toxic Nodular Goiter and Graves’ Disease).
Graves’ Disease
Pathogenesis
Graves’ disease is an autoimmune disorder with familial predisposition. It is characterized by lymphocytic infiltration of the thyroid gland and antithyroid antibodies directed against the TSH receptor. The specific cause of Graves’ is unknown. Thyroid receptor antibodies are primarily thyroid stimulating immunoglobulins, which activate TSH receptors in the membrane of the follicular epithelial cells of the thyroid gland, resulting in excess synthesis and secretion of thyroid hormone and growth of the thyroid gland (see Chapter 5, Hyperthyroidism: Toxic Nodular Goiter and Graves’ Disease).
Historical Perspective
The syndrome known in the Western world as Graves’ disease was independently described by Dr. Caleb Hillier Parry in 1786, Sir Robert James Graves’ in 1835, and Dr. Carl A. Basedow in 1840.2–6 Caleb Hillier Parry, an English physician and descendant from a Welsh pedigree, first described a patient with diffuse goiter and hyperthyroidism in 1786. In 1825, after Parry’s death, his report of eight patients with exophthalmic goiter and hyperthyroidism was published by his son Charles.2 Sir Robert James Graves’ a physician from Dublin, Ireland, published a monograph in 1835 titled “Newly Observed Affection of the Thyroid Gland in Females,” describing six patients with thyrotoxicosis, exophthalmos, and enlargement of the thyroid gland.3 The first description of toxic goiter in Europe was in 1840 by Carl A. von Basedow, a German private practitioner.4 He described exophthalmos, struma (goiter) and palpitations of the heart in three women.
Graves’ disease, Parry’s disease, and Basedow’s disease have all been used to describe the syndrome of thyrotoxicosis, exophthalmos, and diffuse symmetric goiter. It was Armand Trousseau, professor of medicine at the Hotel-Dieu in Paris and author of the foreword of Robert Graves’ book of clinical lectures, who proposed that the syndrome of exophthalmic goiter be named “Maladie de Graves.”7 It has been suggested that the attachment of Graves’ name to the syndrome is the result of Trousseau’s influence.6 A strong case can be made for renaming the syndrome “Parry’s disease,” a proposal that was made by Sir William Osler.6
Epidemiology
The annual incidence of Graves’ disease in the United States is approximately 0.4%.8 It occurs four to six times more commonly in women and usually presents between the ages of 20 and 50 years.8 It is the most common cause of hyperthyroidism, accounting for 50% to 80% of all cases.9 It occurs in association with other autoimmune diseases such as rheumatoid arthritis, systemic lupus erythematosus, chronic lymphocytic thyroiditis, Sjögren’s syndrome, vitiligo, pernicious anemia, type 1 diabetes mellitus, Addison disease, myasthenia gravis, and idiopathic thrombocytopenic purpura.10
Clinical Presentation
The clinical manifestations of Graves’ disease include symptoms and signs of thyrotoxicosis (see Boxes 9-1 and 9-2), a diffuse symmetric goiter often with a palpable thrill or an audible bruit, and a variable degree of presence of extrathyroidal manifestations including ophthalmopathy, pretibial myxedema, and acropachy. Extrathyroidal manifestations occur as a result of cellular infiltration and glycosaminoglycan deposition in the soft tissues in response to antibody reaction to tissue antigens, which cross-react with the TSH receptor in the thyroid gland.
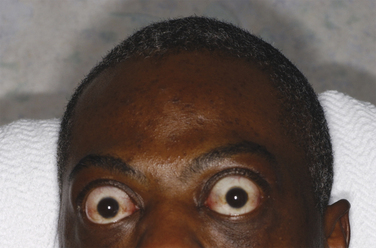
Clinically relevant ophthalmopathy occurs in 20% to 30% of patients with Graves’ disease and is vision-threatening in 3% to 5%.11 It is more common in cigarette smokers and patients with higher levels of thyrotropin receptor antibodies (Figure 9-1). It occurs as a result of antibody-mediated inflammation of the extraocular muscles, retroorbital fat and connective tissue, and the optic nerve. Stare, lid lag, and eyelid retraction are due to excess sympathetic nervous system stimulation of the levator palpebrae superioris muscles and may occur in all patients with hyperthyroidism, but only patients with Graves’ disease have ophthalmopathy. Periorbital edema, chemosis, exophthalmos, and extraocular muscle weakness are more specific manifestations of Graves’ ophthalmopathy. Patients may experience a gritty feeling in the eyes, eye pain, photophobia, tearing, diplopia, and decreased visual acuity. Patients may develop corneal ulcerations as a result of proptosis and lid retraction. Severe proptosis can cause optic neuropathy and blindness.
Diagnosis and Evaluation
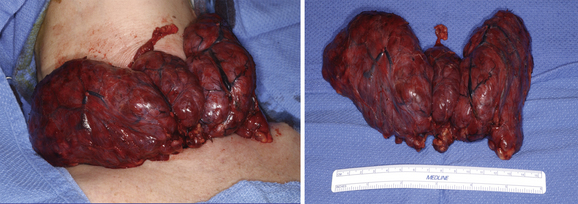
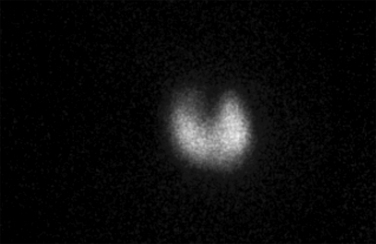
The diagnosis of Graves’ disease is established by the association of hyperthyroidism, a diffuse symmetric goiter (Figure 9-2) and increased radioiodine uptake. Iodine-123 thyroid scintigraphy demonstrates diffuse symmetric uptake in the thyroid gland (Figure 9-3); however, it is not routinely necessary to make a diagnosis of Graves’ disease. Measurement of radioiodine uptake and thyroid scintigraphy are primarily of value in helping to differentiate thyrotoxicosis caused by Graves’ disease from toxic multinodular goiter, a solitary toxic adenoma or thyroiditis. In rare circumstances, documentation of elevated thyroid stimulating immunoglobulins, because of their high sensitivity and specificity, may be helpful in establishing or excluding a diagnosis of Graves’ disease.
Treatment
The goals of therapy for Graves’ disease are rapid amelioration of symptoms and prevention of recurrent hyperthyroidism. There are three therapeutic alternatives for Graves’ disease: antithyroid drugs, radioiodine ablation, and thyroidectomy. Each alternative has its own advantages and disadvantages. Patient, physician, institutional, or geographic preferences often influence the choice of therapy. In the United States, radioiodine ablation is most commonly used.12 In Europe, Japan, and South America, prolonged antithyroid drug therapy is the preferred option13,14 (see Chapter 5, Hyperthyroidism: Toxic Nodular Goiter and Graves’ Disease).
Antithyroid Drugs
Most patients with Graves’ disease are initially treated with an antithyroid drug. The antithyroid drugs that are used are the thionamide agents, propylthiouracil and methimazole. Both agents decrease thyroid hormone synthesis and re-establish a euthyroid state in 3 to 8 weeks. A beta-blocker is often added for the rapid amelioration of symptoms attributable to excess sympathetic nervous system activity such as palpitations, tachycardia, tremor, heat intolerance, diaphoresis, and anxiety. Permanent remission of Graves’ disease occurs in 20% to 50% of patients after 12 to 18 months of therapy, typically in patients with smaller goiters and with less severe hyperthyroidism.13
Lifelong antithyroid drug therapy is one option for the management of patients with Graves’ disease who relapse after discontinuation of antithyroid drugs therapy. However, in the United States, lifelong administration of antithyroid drug is seldom used for definitive therapy for Graves’ disease. Antithyroid drugs are routinely used for preoperative preparation, and propylthiouracil is preferred for the management of Graves’ disease during pregnancy. Minor adverse reactions to antithyroid drugs occur in approximately 5% of patients and include rash, urticaria, arthralgia, fever, anorexia, nausea, and abnormalities of taste and smell. Major adverse effects include agranulocytosis, which occurs in approximately 0.1% to 0.3% of patients, and hepatotoxicity, an even rarer complication, which may be fatal.9,15
Radioiodine
Radioiodine was introduced for treatment of hyperthyroidism in the 1940s.16 Prior to the 1940s, subtotal thyroidectomy was the standard therapy for Graves’ disease. Iodine-131 gradually became the first-line treatment for Graves’ disease in the United States. Iodine-131 admits beta particles, which destroy the follicular cells of the thyroid gland. At most centers, the goal of radioiodine therapy is to induce hypothyroidism in order to prevent recurrence of Graves’ disease.9 This is achieved in approximately 80% of patients with either a calculated or fixed dosage regimen.17
Radioiodine ablation therapy takes a median of 3 months and sometimes multiple doses before hyperthyroidism is corrected.18 Radioiodine therapy is contraindicated in women who are pregnant or who are breast-feeding. A pregnancy test should be obtained prior to radioiodine administration in all women of reproductive age. Radioiodine is excreted in the urine, exposing the pelvic viscera to radiation. Radioiodine also crosses the placenta where it can be taken up by the fetal thyroid gland. It is generally recommended that women do not become pregnant for 6 to 12 months after radioiodine treatment.9 Side affects of radioiodine ablation include neck pain and tenderness from radiation-induced thyroiditis, transient increase in thyroid hormone levels, and worsening of Graves’ ophthalmopathy.9
Surgery
Surgical treatment of Graves’ disease is indicated for (1) pregnant patients requiring high doses of an antithyroid drug or who are intolerant to antithyroid drugs, (2) patients with a concomitant thyroid nodule that is malignant or suspicious for malignancy, (3) failure of radioiodine therapy, (4) massive thyroid enlargement (see Figure 9-2) with compressive symptoms, (5) severe ophthalmopathy, and (6) patient preference. Patient preference is often related to the desire for the most rapid amelioration of symptoms, a reluctance to receive radioiodine because of having young children, a desire to become pregnant, and a fear of exposure to radiation. The advantages of surgical therapy are that patients experience immediate symptomatic improvement and, with total thyroidectomy, the risk of recurrent hyperthyroidism is eliminated. It also allows for treatment of concomitant thyroid nodules and incidental thyroid carcinoma. Incidental carcinoma has been reported to occur in 2.3% of patients with Graves’ disease.19 In addition, total thyroidectomy is effective in improving the eye manifestations attributable to excess adrenergic activity.20
The disadvantage of surgical treatment of Graves’ disease is the risk of complications from thyroidectomy, which include recurrent laryngeal nerve injury, hypoparathyroidism, neck hematoma, and thyroid storm. Hypothyroidism is an intended consequence of total thyroidectomy and requires lifelong thyroid hormone replacement. When total thyroidectomy is performed by a skilled surgeon, the incidence of recurrent laryngeal nerve injury and hypoparathyroidism is approximately 1% to 2%, and neck hematoma is 1% or less.20–23
Thyroid storm is a life-threatening condition that can be precipitated by surgery in a patient with poorly treated hyperthyroidism. It is characterized by severe manifestations of hyperthyroidism along with fever, nausea, vomiting, diarrhea, tachyarrhythmias, congestive heart failure, agitation, and delirium. The risk of thyroid storm can be eliminated by adequate preoperative preparation.21,22 An antithyroid drug is used to normalize free T4 and free T3 levels prior to the operation. A beta-blocker is used for symptomatic treatment of adrenergic symptoms and tachycardia. Once the patient’s free T4 and free T3 levels are normalized, a saturated solution of potassium iodide (50 mg mixed in an 8-oz glass of water daily) is administered for 10 days prior to surgery (Box 9-3). Iodide treatment preoperatively reduces the rate of blood flow, thyroid vascularity, and intraoperative blood loss during thyroidectomy for Graves’ disease.24 In patients who are noncompliant or intolerant to antithyroid drugs, thyroidectomy can be performed safely using adequate beta-blockade alone.25
In the past, bilateral subtotal thyroidectomy was the standard treatment for Graves’ disease in the United States. This most often consisted of leaving a 3-gram remnant of thyroid tissue on either side of the trachea in an attempt to establish and maintain a euthyroid state, reduce the risk of recurrent laryngeal nerve injury and hypoparathyroidism, and minimize the risk of persistent or recurrent hyperthyroidism. The problem with subtotal thyroidectomy is that it is difficult to standardize remnant sizes and to establish a reproducible relationship between remnant size and a euthyroid state postoperatively.26 Forty percent to 60% of patients with Graves’ disease treated with bilateral subtotal thyroidectomy become hypothyroid within 20 years of operation.27 As a result, diligent long-term follow-up is necessary to prevent delay in diagnosis and treatment of hypothyroidism and development of untoward sequelae. Bilateral subtotal thyroidectomy is also associated with an approximate 8% rate of persistent or recurrent hyperthyroidism and is even as high 28% depending on the size of thyroid remnants.28,29
Total thyroidectomy is the preferred surgical option for treatment of Graves’ disease when thyroid hormone replacement therapy is readily available. Removal of all thyroid tissue eliminates the potential for persistent or recurrent hyperthyroidism. Persistent or recurrent hyperthyroidism is a particularly bad outcome because it may subject patients to radioiodine therapy, which they may have initially declined, or reoperative surgery, which has an increased risk of morbidity. Total thyroidectomy simplifies the postoperative follow-up because all patients are started on a replacement dose of thyroid hormone. In addition, total thyroidectomy eliminates the antigen that is the source for the TSH receptor antibodies and other antibodies that cross-react with antigens in the extraocular muscles, the retroorbital connective tissue, and the optic nerve.30
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


