Chapter 37 Central Neck Dissection
Indications
Introduction
In 2010 there were an estimated 44,670 new cases of thyroid cancer despite only 1690 deaths resulting from the disease.1 Differentiated thyroid cancer accounts for the majority of these new cases, of which 85% are papillary thyroid cancers.2 Death results predominately from more aggressive histologic variants, poorly differentiated, or anaplastic thyroid cancers. From 1973 to 2002, the incidence of thyroid cancer increased from 3.6 per 100,000 to 8.7 per 100,000. This is almost entirely due to an increase in papillary thyroid cancer likely influenced by detection of smaller cancers. Papillary thyroid cancer has increased by 5 per 100,000.3 The mainstay of the therapy for papillary thyroid cancer is resection consisting of thyroidectomy with or without lymphadenectomy.
Preoperative evaluation of cervical lymph nodes for staging and surgical planning is necessary to determine the extent of surgery (see Chapter 14, Preoperative Radiographic Mapping of the Nodal Disease for Papillary Thyroid Carcinoma).2 Up to 50% of patients with papillary thyroid cancer have clinically detectable lymph node metastases at initial diagnosis.2,4,5 Occult or micrometastases may be present in up to 90% of cases.6,7 “Skip” metastases to the lateral neck compartments may occur, especially with superior pole primary tumors, but, more typically, initial nodal involvement is in the central compartment.8,9 There is a clear consensus supporting therapeutic central lymph node dissection for clinically apparent nodal disease and increased recognition of the importance of identifying these patients preoperatively and intraoperatively to avoid unnecessary reoperation for disease that went undertreated initially.2
The role for prophylactic central lymph node dissection is less clearly defined. In this chapter we review the ongoing debate regarding the need for prophylactic central lymph node dissection.10,11 To review specifics regarding the technical aspects of primary or revision central neck dissection, please see Chapters 38, Central Neck Dissection: Technique, and 53, Reoperative Thyroid Surgery. To date, there has been no prospective randomized trial to evaluate how prophylactic central neck dissection affects the outcome of papillary thyroid cancer. However, a recent meta-analysis of the available retrospective studies involving 1264 patients found no significant difference in locoregional recurrence rates overall (2% versus 3.9%) or within the central (1.9% versus 1.7%) or lateral (3.7% versus 3.8%) neck compartment with or without prophylactic central neck dissection.12
Definition
The recent consensus statement on the terminology and classification of central neck dissection recommends the use of consistent terminology when describing central nodal dissection. This includes defining the indication for dissection as therapeutic versus prophylactic. The term routine is not a specific descriptor regarding indication; rather it relates to the frequency with which the procedure is utilized. Therapeutic dissection involves removal of nodal metastases identified preoperatively or intraoperatively as containing metastases (clinically N1). Prophylactic dissection involves removal of lymph nodes that do not appear to contain metastases (clinically N0). Prophylactic dissection may also be called elective lymph node dissection. Furthermore, the extent of central neck dissection should be described as unilateral or bilateral (relative to its paratracheal component) and should indicate which side the dissection was performed unilaterally. Unilateral central neck dissection involves comprehensive removal of pretracheal and prelaryngeal node-bearing tissue along with unilateral paratracheal node removal. Bilateral dissection includes removal of pretracheal and prelaryngeal, as well as bilateral paratracheal, node bearing tissue.13 Lastly, comprehensive central neck dissection, either unilateral or bilateral, is a compartmental dissection and is distinguished from node plucking or “berry picking” of only the clinically involved nodes, which is associated with increased rates of recurrence and strongly discouraged.
Therapeutic Lymph Node Dissection
The 2009 American Thyroid Association (ATA) guidelines recommend therapeutic central neck dissection (level VI) at the time of thyroidectomy for all patients with clinically involved lymph nodes.2 Vigilance is required pre- and intraoperatively to accurately detect clinically evident nodal metastasis requiring dissection. The rationale for therapeutic central neck dissection at the time of thyroidectomy is relatively straightforward—namely to comprehensively remove all grossly evident nodal disease, along with any adjacent subclinical disease, to minimize risk of morbidity from reoperation for clinically evident disease initially undertreated.
The extent of therapeutic central neck dissection can be either unilateral or bilateral. Bilateral dissection is clearly required when clinically evident disease is present in both paratracheal regions. Bilateral central node dissection is recommended at the time of initial surgery when clinically detectable nodes are present within the central compartment. The number of lymph nodes removed is inversely related to thyroglobulin level as well with greater rates of athyroglobulinemia achieved with more complete node dissection.14 A more selective, therapeutic unilateral central neck dissection may be preferred in cases of recurrent/persistent disease confined to only one paratracheal region to minimize risk to both recurrent laryngeal nerves.
A recent review of the Surveillance, Epidemiology, and End Results (SEER) registry revealed that there is an increased risk of death in patients with papillary thyroid cancer age 45 or older with nodal metastasis after adjusting for the effects of age, gender, race, ethnicity, radiotherapy, tumor size, tumor extent, and type of surgery. There was no difference in survival in patients younger than 45 with or without nodal metastasis.15 Podnos et al. reviewed SEER data finding that 22% of patients with papillary or follicular thyroid cancer were staged as clinically N1 at presentation. Survival at 14 years was 82% for node-negative patients and 79% for node-positive patients (p < 0.0001). In this same study, patients age 45 or younger who were clinically N1 also had reduced survival (96% N0 versus 90% N1).16 Goals of resection of clinically evident nodal metastases include reducing the development of recurrent disease and increasing survival. Multiple series have demonstrated a correlation with nodal metastases and increased rates of persistent or recurrent disease.4,5,17,18
Surgical planning for management of papillary thyroid cancer involves preoperative evaluation of cervical lymph nodes. Preoperative neck ultrasound for cervical lymph nodes is recommended for all patients undergoing thyroidectomy for malignancy2 and may reduce rates of recurrent or persistent disease by allowing adequate initial surgical treatment.19 Cervical ultrasound is an accurate, noninvasive exam that can be performed by the operating surgeon, or by another practitioner with a specific interest in node mapping, as part of a patient’s initial evaluation and is the primary preoperative imaging modality. Neck computed tomography (CT) or magnetic resonance imaging (MRI) may be appropriate for the assessment of cervical nodal status in centers, especially where experience with neck ultrasound for nodal disease is lacking. When used prior to initial operation, ultrasound has an 83.5% sensitivity and 97.7% specificity for nodal metastases20 and may identify abnormal nodes not found on physical exam in up to 20% of patients.21 Unfortunately, ultrasound before thyroidectomy misses 50% to 90% of level VI lymph node metastases, either because they are obscured by overlying thyroid or are microscopic.22,23 A recent review illustrated the importance of preoperatively performed ultrasound by a provider focused on accurate mapping to permit lymph node dissection of the compartment containing the affected nodes.24
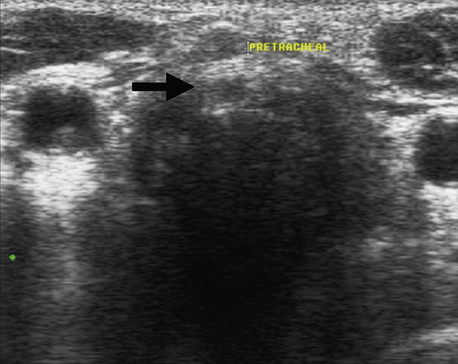
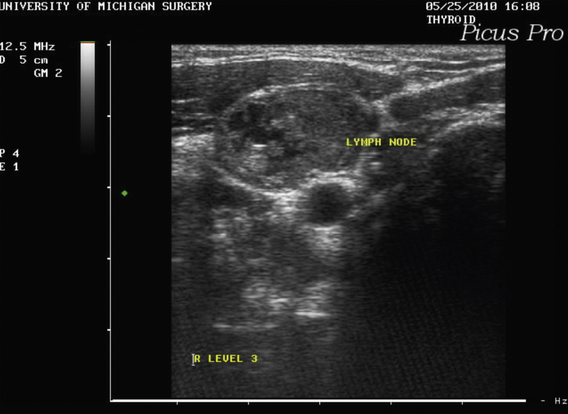
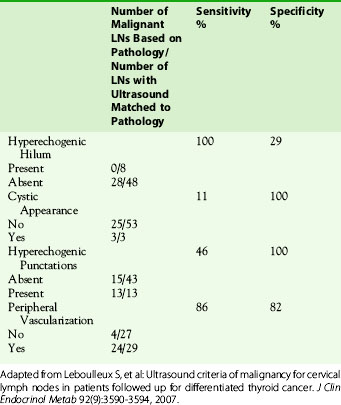
Ultrasound features of malignant lymph nodes include hypoechogenicity, hypervascularization, and loss of hilar architecture (hilar stripe). They tend to be large, round, and may demonstrate a cystic appearance or microcalcifications (Figures 37-1 and 37-2). Cystic appearance, microcalcifications, absence of a hilum, and peripheral vascularization are considered major ultrasound criteria of lymph node malignancy (Figure 37-3). These findings were based on ultrasound done 4 days prior to surgery and correlated with surgical findings after lymph node dissection25 (Table 37-1).

Intraoperative inspection of central compartment lymph nodes is another technique to detect clinically involved nodes requiring therapeutic central neck dissection. Although it is well accepted that intraoperative inspection underestimates the presence of pathologically detected nodal metastases,39 especially microscopic, a recent study documented the reliability of the surgeon to accurately determine the need for therapeutic central neck dissection based on a combination of preoperative ultrasound and intraoperative node inspection.26 Clinically, lymph nodes with papillary thyroid carcinoma metastasis often appear to have a dark blue or black appearance. Further, central lymph nodes larger than 1 cm are significantly more likely to contain metastasis. The role for other adjunctive techniques such as sentinel node biopsy or frozen section evaluation of randomly sampled central neck nodes to identify metastatic nodes requiring therapeutic dissection remains uncertain.
Prophylactic Neck Dissection
Because occult lymph node metastases are common in papillary thyroid cancer, there is an ongoing debate regarding surgical management for clinically node-negative disease. Clinically detectable nodal metastases are known to correlate with higher rates of persistent or recurrent disease during postoperative surveillance.5 There is no reliable noninvasive method for the preoperative detection of lymph node involvement. As a result, some have advocated prophylactic level VI lymph node dissection as part of routine surgery for differentiated thyroid cancer. However, no consensus exists yet regarding the addition of level VI lymph node dissection for clinically node-negative patients with well-differentiated papillary carcinoma. To date, no study has demonstrated significantly reduced recurrence or mortality rates with prophylactic central node dissection, and a recent meta-analysis found no significant difference in recurrence rates between those treated with or without prophylactic central neck dissection at the time of thyroidectomy (2% versus 3.9%, OR 1.05, CI 95% 0.48-2.31).12 Therefore, the rationale for elective central neck dissection performed routinely as preventative or prophylactic for either recurrence or death is questionable in well-differentiated papillary carcinoma. However, there are other strategic uses for elective central node dissection that may have justification, primarily to permit accurate patient staging and more selective subsequent adjunctive therapy with radioiodine in patients with low-risk primary tumors (T1 or T2). Further, there may be a prophylactic role for elective central dissection when used selectively in patients with higher-risk primary tumors, such as those with extrathyroidal extension (T3 or T4), mutations such as BRAF, or more aggressive histologies such as diffuse sclerosing, insular, or poorly differentiated. Elective central neck dissection is recommended for medullary thyroid carcinoma.27 The advantages and disadvantages of central neck dissection are outlined in Table 37-2.
Table 37-2 Pros and Cons of Central Neck Dissection
| Pros | Cons | |
|---|---|---|
| Therapeutic CND | Reduces disease recurrence Improves survival May reduce need for reoperation | Postoperative hypocalcemia Postoperative RLN palsy, permanent or transient |
| Prophylactic CND | May improve survival May reduce disease recurrence Accurate staging may eliminate need for postoperative RAI ablation Reoperative surgery more complicated | Increases postoperative hypocalcemia Increased rates of RLN palsy, transient and permanent Survival, recurrence benefit unproven in randomized trials |
Prophylactic level VI lymph node dissection may be included as part of the initial surgical management for thyroid cancer.2 Some studies demonstrate increased rates of locoregional recurrence in patients who have lymph node metastases.18,28 Though regional nodal metastases increase local recurrence rates, they may not ultimately affect survival.11 Other data, however, have demonstrated increased mortality in patients with lymph node metastases.29 One Swedish study provides data supporting routine central neck dissection but failed to distinguish between therapeutic and elective/prophylactic intent and may suffer from selection bias.30 Data from an endocrine surgical group at one hospital were reviewed from 1970 to 1989, and 195 patients were identified with papillary thyroid cancer. All patients had compartment-oriented level VI lymph node dissections. Mean follow-up was 13 years, and patients were compared to two other cohorts of patients from other Scandinavian countries. Death from thyroid cancer occurred in 1.6% of the Swedish patients compared with 8.4% to 11.1% in the comparison groups; however, the Swedish cohort excluded patients who had distant metastasis at time of presentation, whereas the other cohorts included all patients, even those deemed unresectable at time of surgery. Other studies have reported improved outcome with node dissection.4,31
Sywak et al. used thyroglobulin as a surrogate outcome measure to support prophylactic central neck dissection.32 This study included 447 patients treated surgically for papillary thyroid cancer who were clinically node negative. They were divided into two groups based on surgical procedure: total thyroidectomy alone (391 patients) or total thyroidectomy plus level VI lymph node dissection (56 patients). Both groups were treated using a similar algorithm with radioactive iodine (RAI). Postablation serum thyroglobulin levels were significantly lower in the node-dissection group. Furthermore, more patients had an undetectable serum thyroglobulin level in the node-dissection group (72% versus 43%, p < 0.001). However, no significant differences were reported in locoregional recurrence rates (3.6% versus 5.6%) or disease-specific mortality rates (0% versus 0%), despite significantly shorter median follow-up duration (25 versus 70 months) in the prophylactic central neck dissection group.32 Further, a subsequent study from the University of Michigan failed to support the finding of improved biochemical evidence of disease with prophylactic central neck dissection compared to thyroidectomy alone.33
A more recent series demonstrated no significant difference in recurrence rates in the central neck following thyroidectomy plus level VI lymph node dissection compared with thyroidectomy alone (4.4% versus 16.7%, p = 0.13). Both groups were treated with RAI ablation postoperatively, although the mean radioiodine dose was significantly higher and the mean tumor size significantly smaller in the central neck dissection group.34 Another recent study also found no significant difference in recurrence rates among patients with papillary thyroid carcinoma, clinically N0, undergoing total thyroidectomy with prophylactic central neck dissection compared with thyroidectomy alone (6.3% versus 7.7%) despite longer follow-up in the thyroidectomy alone group.35 An additional recent study of clinically node-negative patients failed to demonstrate any significant difference in 5-year disease-free survival following thyroidectomy with prophylactic central node dissection compared with thyroidectomy alone (88% versus 86%, p = 0.72).36
Other groups have evaluated outcomes comparing total thyroidectomy alone with total thyroidectomy plus central lymph node dissection and have demonstrated no difference in recurrence rate and no survival benefit. In one study, there was no significant difference in recurrence rate if patients underwent prophylactic lymph node dissection.37 Another group demonstrated no significant difference in lymph node recurrence rates in patients with micrometastases,38 a finding which has been shown in other series as well.23 A survival benefit after central lymph node dissection was not demonstrated in another series of patients with papillary thyroid cancer.39 Of 97 patients with papillary thyroid cancer, 53 also had a level VI lymph node dissection. The overall survival of all patients in the series with papillary thyroid cancer was 92% and 89% after 5 and 10 years, respectively. Patients who had a thyroidectomy plus level VI lymph node dissection had a 10-year survival of 88%, a difference not statistically significant.
Arguments against prophylactic level VI lymph node dissection focus on unproved advantages with regard to recurrence and survival and the potential for increased morbidity with the addition of central lymph node dissection. Other arguments against routine prophylactic central lymph node dissection relate to increased rates of complications following the addition of level VI lymph node dissection. Without the addition of central lymph node dissection, total thyroidectomy results in permanent hypoparathyroidism in 1% to 2% of patients and permanent laryngeal nerve injury in 1% to 2% of patients.41 No prospective randomized data exist to evaluate thyroidectomy plus level VI lymph node dissection compared to total thyroidectomy alone. Therefore, no concrete recommendation can be made regarding the risk of injury to nerves or creating permanent hypoparathyroidism; however, the literature consistently demonstrates statistically significant higher rates of transient hypocalcemia with central neck dissection compared to thyroidectomy alone.9,30,32,39,42,43 A recent meta-analysis demonstrated significantly higher rates of transient hypocalcemia with thyroidectomy plus central neck dissection versus thyroidectomy alone; however, no significant difference was noted for rates of permanent parathyroid morbidity or for recurrent laryngeal nerve injury. The number needed to harm was calculated at 7.7 such that for every eight cases where central node dissection is electively performed, one additional patient can be expected to experience hypocalcemia.40 Whether the published results from high-volume centers are applicable to surgeons who perform central neck dissection less commonly remains a valid question. Recent guidelines suggest that if the appropriate surgical expertise is available, central lymph node dissection may be added to total thyroidectomy, especially for higher-risk primary tumors with similar long-term complication rates.2
The risk of injury to the recurrent nerves and parathyroid glands may be greater if the intended lymph node dissection is therapeutic rather than prophylactic because of the extent of disease. In one series, 159 patients were treated for papillary thyroid cancer by a single surgeon.44 All patients had a thyroidectomy at the initial operation. Forty-two patients had a therapeutic lymphadenectomy, 29 patients had a prophylactic lymphadenectomy, and 88 patients had no lymphadenectomy. No patients with either thyroidectomy alone or prophylactic lymph node dissection had permanent complications. Four patients who had a therapeutic lymph node dissection had permanent recurrent laryngeal nerve injuries believed to be related to the excision of extensive nodal metastases. In one case, the recurrent nerve was sacrificed because of the extent of disease.
Despite possible increased complication rates with central lymph node dissection, it has been proposed by some at initial operation in an attempt to reduce further morbidity from reoperation in the minority of patients who recur. Reoperative surgery for recurrent papillary thyroid cancer in central compartment nodes generally leads to greater morbidity to parathyroid glands and to recurrent laryngeal nerves compared with initial surgery.45–47 Other studies from experienced centers, however, have shown low complication rates with reoperative central compartment dissection that were similar or lower than complication rates with initial dissection.48 Reoperative surgery involves the removal of persistent or recurrent nodal disease in a compartment-oriented fashion as outlined by recent guidelines.13 Patients may present for surgery with preexisting hypoparathyroidism or recurrent laryngeal nerve injury, which creates additional challenges for reoperation.49 The series by Simon et al. reviewed records of 252 patients treated surgically for differentiated thyroid cancer.46 One hundred seventeen patients had a single operation, and 77 underwent reoperation for recurrent disease. The incidence of recurrent laryngeal nerve palsy and hypoparathyroidism was 6.8% and 1.7%, respectively, after initial operation and 2.6 and 3.9%, respectively, after reoperation. Other series report rates of postoperative permanent hypocalcemia as high as 9% with permanent recurrent laryngeal nerve palsy of 25%.50 The potential risks of central neck dissection are outlined in Table 37-3.
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


