Chapter 56 Primary Hyperparathyroidism
Pathophysiology, Surgical Indications, and Preoperative Workup
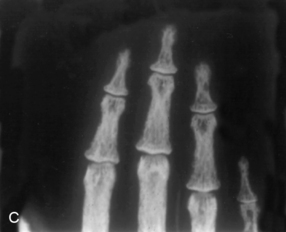
Primary hyperparathyroidism is characterized by hypercalcemia and elevated parathyroid hormone levels. Patients with the disease today in the United States bear little resemblance to those with the severe disorder of “stones, bones, and groans” described by Fuller Albright and others in the 1930s.1–4 Then, patients presented with osteitis fibrosa cystica, characterized by brown tumors of the long bones, subperiosteal bone resorption, distal tapering of the clavicles and phalanges, and salt-and-pepper–appearing erosions of the skull on radiograph (Figure 56-1). Nephrocalcinosis was present in 80% of patients, and neuromuscular dysfunction with muscle weakness was common. With the advent of the automated serum chemistry autoanalyzer in the 1970s, the diagnosis of primary hyperparathyroidism became more common, and an asymptomatic version of the disorder was recognized with increasing frequency. In the United States, more than three quarters of modern primary hyperparathyroid patients lack these classical symptoms of primary hyperparathyroidism. Nephrolithiasis is still seen, although much less frequently than in the past. Radiologically evident bone disease is rare, although bone involvement is readily detected by bone densitometry.



Little controversy existed concerning appropriate therapy for primary hyperparathyroidism in its classic presentation. Surgery was indicated in all patients for this disorder that was virtually always symptomatic. This is no longer the case. With clear-cut symptoms absent in most patients, the need for parathyroidectomy in all patients has been questioned. Guidelines for surgery in asymptomatic primary hyperparathyroidism have existed since the 1990 National Institutes of Health Consensus Development Conference on Asymptomatic Primary Hyperparathyroidism. Since that time, new data have become available on the long-term follow-up of asymptomatic patients with and without parathyroidectomy that have led to two revisions of these guidelines. The most recent guidelines, issued in 2009 after the 2008 International Conference on the Management of Asymptomatic Primary Hyperparathyroidism, continues to refine which patients can be followed safely without surgical intervention.5
Bone Densitometry
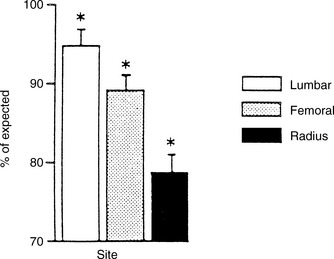
The advent of bone mineral densitometry as a major diagnostic tool for osteoporosis occurred at a time when the clinical profile of primary hyperparathyroidism was changing from a symptomatic to an asymptomatic disease. Questions about skeletal involvement in primary hyperparathyroidism could be addressed despite the absence of overt radiologic features of the disease. Dual energy x-ray absorptiometry (DXA) in primary hyperparathyroidism has provided insight in this regard. Three-site densitometry (lumbar spine, hip, and distal 1/3 radius) has been particularly informative because of the proclivity of PTH to be catabolic at cortical sites (e.g., distal 1/3 radius) and anabolic at cancellous sites (e.g., lumbar spine). In primary hyperparathyroidism, bone density at the distal third of the radius is diminished.6,7 Bone density at the lumbar spine is only minimally reduced, typically within 5% of age-matched mean values. The hip region, containing a relatively equal mixture of cortical and cancellous elements, shows a densitometric value that is intermediate between the cortical and cancellous sites (Figure 56-2). The results of studies of these sites support not only the notion that PTH is catabolic in cortical bone but also the view that PTH is anabolic in cancellous bone.8,9 In postmenopausal women with primary hyperparathyroidism, the same pattern was observed.6 Thus, postmenopausal women with primary hyperparathyroidism show a reversal of the pattern typically associated with postmenopausal estrogen deficiency—namely, preferential loss of cancellous bone. These observations suggest that primary hyperparathyroidism may help to protect postmenopausal women from cancellous bone loss due to estrogen deficiency.
The bone density profile in which skeletal mass is relatively preserved at the vertebrae and diminished at the more cortical distal radius is not always seen in primary hyperparathyroidism. A small group of hyperparathyroid patients have evidence of vertebral osteopenia at the time of presentation. In our natural history study, approximately 15% of patients had a lumbar spine Z score (number of standard deviations away from age and sex-matched mean) of less than 1.5 at the time of diagnosis.10 In addition, patients with primary hyperparathyroidism can show uniform reductions in bone mineral density at all sites, whereas others, although rare, have normal bone density at all sites.
Bone Histomorphometry
Analyses of percutaneous bone biopsies from patients with primary hyperparathyroidism have provided a picture of cortical thinning, maintenance of cancellous bone volume, and a very dynamic process associated with high turnover and accelerated bone remodeling. As suggested by results of bone densitometry, cancellous bone volume is clearly well preserved in primary hyperparathyroidism. Several studies have shown that cancellous bone is actually increased in primary hyperparathyroidism compared with normal subjects.11–13
Preservation of cancellous bone volume even extends to comparisons with the expected losses associated with the effects of aging on cancellous bone physiology. In patients with primary hyperparathyroidism, no relationship between trabecular number or separation and age exists, suggesting that the actual trabeculae and their connections have been maintained over time more effectively than in normal aging individuals. Therefore, primary hyperparathyroidism seems to retard the normal age-related processes associated with trabecular loss.14 Trabecular strut analysis has in fact demonstrated that cancellous bone is preserved in primary hyperparathyroidism through the maintenance of well connected trabecular plates.14 Using more advanced technology, a recent three-dimensional analysis of trans-iliac bone biopsies using microCT technology15 confirmed that postmenopausal women with primary hyperparathyroidism (PHPT) had higher bone volume (BV/TV), higher bone surface area (BS/TV), higher connectivity density (Conn.D), and lower trabecular separation (Tb.Sp.). There were also less marked age-related declines in BV/TV and Conn.D as compared to controls, with no decline in BS/TV.
Fractures
Data on fracture incidence in primary hyperparathyroidism remain controversial. An early paper by Dauphine et al. reported an increased prevalence of vertebral fractures in patients with mild primary hyperparathyroidism, but several more recent studies have failed to confirm this observation.16–20 Data are not sufficient for one to form any valid conclusions about a relationship between PTH-mediated cortical bone loss and an increased occurrence of long-bone or proximal femur fractures. It would seem logical to anticipate this consequence of cortical bone loss, but primary hyperparathyroidism is not a dominant feature in any series of hip fracture patients, and hip fractures are not a dominant feature in any series of elderly patients with primary hyperparathyroidism. In a study that considered hip fracture, a population-based prospective analysis (mean of 17 years duration, 23,341 person years) showed women with primary hyperparathyroidism in Sweden not to be at increased risk.18 This observation strongly suggests that, as is the case with primary hyperparathyroidism and vertebral fractures, long-bone and proximal femur fractures are not seen commonly in untreated primary hyperparathyroidism.
A population-based study reported an increased incidence of vertebral, Colles’ rib, and pelvic (but not hip) fractures in patients with primary hyperparathyroidism who were being followed in Rochester, Minnesota.20 The result with respect to vertebral fractures is somewhat unexpected, given the relative preservation of bone density at this site by densitometry testing. Selection bias in the determination of vertebral fractures could explain these findings. The skeleton of patients who carry the diagnosis of primary hyperparathyroidism is typically monitored more carefully than most, and vertebral fractures might be diagnosed with increased frequency in this more closely monitored population, in whom back pain is more likely to lead to a radiograph. On the other hand, it is unlikely that a Colles’ fracture, a more expected consequence of the hyperparathyroid process in bone, would be asymptomatic. Thus, the increased incidence of forearm fractures, at a site containing more cortical bone, is consistent with expectations in those patients with untreated hyperparathyroidism. In a more recent study, Vignali et al. assessed vertebral fractures in primary hyperparathyroidism as determined by DXA-based vertebral fracture assessment21 and found vertebral fractures more frequently in subjects with PHPT (24.6%) than in the control subjects (4.0%; p < 0.001). Among asymptomatic PHPT patients, only those who met surgical guidelines showed a higher incidence of vertebral fractures compared with controls. We still lack prospective, controlled studies to determine fracture incidence in primary hyperparathyroidism.
Nephrolithiasis
Although classic clinical descriptions of primary hyperparathyroidism emphasized skeletal involvement and kidney stones as principal complications of the disease, kidney stones remain the most common manifestation of the symptomatic disease.22 Estimates in recent studies place the incidence of kidney stones at 15% to 20% of all PHPT patients. Hypercalciuria is seen in approximately 40% of patients with primary hyperparathyroidism. The frequency of nephrocalcinosis is unknown.23
Other Organ Involvement
Over the years, primary hyperparathyroidism has been described as affecting many different organ systems. Perhaps the most common complaints have been those nonspecific descriptions of weakness and easy fatigability. Classic primary hyperparathyroidism has been associated with a distinct neuromuscular syndrome, characterized by type II muscle cell atrophy.24 In the milder, less symptomatic form of the disease that is common today, this disorder is rarely seen.25 The neuropsychiatric abnormalities of primary hyperparathyroidism has long been an area of active interest.26–28 Many patients, families, and physicians comment on features of depression, cognitive difficulties, and anxiety in those with the disease. Furthermore, many of these complaints have been described as being reversible after parathyroidectomy. The surgical literature provides further data supporting postoperative improvements.29–34 Data from Clark’s group reported on 152 patients (thyroid surgery control subjects) found 40% of patients reporting less fatigue after surgical cure.29 Similar findings were reported by Pasieka and Parsons30 and Burney et al.31 However, the three randomized controlled trials of surgery versus observation in mild primary hyperparathyroidism have shown variable effects of surgery on psychiatric and quality-of-life measures.35–37 Interim analysis of the largest trial (Bollerslev et al.) concluded that there was insufficient evidence of predictable improvement in these indices to recommend surgery solely for the purpose of reversing these complaints. A recent case-controlled study suggests that there are also some cognitive deficiencies in postmenopausal women with primary hyperparathyroidism, and that some of these normalize after parathyroidectomy.38
Many other pathologic features have been described in patients with primary hyperparathyroidism. Hypertension has been noted to be present in a higher percentage of patients than expected.39,40 However, the hypertension does not remit with cure of the underlying hyperparathyroid process. The only randomized controlled trial data show improvement in follow-up of blood pressure in both those who had and those who did not have surgery.41 Data on cardiovascular manifestations of mild primary hyperparathyroidism remain incomplete. Recent reports suggest that left ventricular hypertrophy, common in those with more severe disease, is not seen in those with very mild primary hyperparathyroidism, whereas carotid intima medial thickness is increased in this disorder.42,43 The effect of surgery on these indices remains to be seen.
Associations have also been reported between primary hyperparathyroidism and peptic ulcer disease. Today, it is felt that a significant relationship between the two conditions exists only in patients with multiple endocrine neoplasia, type 1. The association of pancreatitis with primary hyperparathyroidism found in patients with marked hypercalcemia is not seen in those with mild elevations in serum calcium. Finally, gout and pseudogout have been described in primary hyperparathyroidism, both in the setting of untreated disease and immediately after surgical cure.44 Again, verifiable etiologic relationships between primary hyperparathyroidism and uric acid or pyrophosphate arthropathy remain to be established.
Pathology
The pathology of primary hyperparathyroidism is discussed in detail in Chapter 70, Surgical Pathology of the Parathyroid Glands. By far the most common lesion found in patients with the disease is the single parathyroid adenoma, occurring in 80% of patients. Risk factors that have been identified for development of primary hyperparathyroidism include a history of neck irradiation45 and prolonged use of lithium therapy for affective disorders.46,47 However, the majority of cases of primary hyperparathyroidism have no defined cause. Molecular abnormalities leading to clonal emergence are discussed elsewhere (see Chapters 58, Principles in Surgical Management of Primary Hyperparathyroidism, 67, Parathyroid Management in the MEN Syndromes, 69, Parathyroid Carcinoma, and 70, Surgical Pathology of the Parathyroid Glands). Although in most cases a single adenoma is found, multiple parathyroid adenomas have been reported in 2% to 4% of cases.48 These may be familial or sporadic. Parathyroid adenomas can be discovered in many unexpected anatomic locations. Embryonal migration patterns of parathyroid tissue account for a plethora of possible sites for ectopic parathyroid adenomas. The most common ectopic sites are within the thyroid gland, the superior mediastinum, and the thymus. Occasionally the adenoma may ultimately be identified in the retroesophageal space, the pharynx, the lateral neck, and even the submucosa of the esophagus (see Chapters 2, Applied Embryology of the Thyroid and Parathyroid Glands, 58, Principles in Surgical Management of Primary Hyperparathyroidism, 59, Standard Bilateral Parathyroid Exploration, 60, Minimally Invasive Single Gland Parathyroid Exploration, 65, Surgical Management of Multiglandular Parathyroid Disease, 66, Surgical Management of Secondary and Tertiary Hyperparathyroidism, and 68, Reoperation for Sporadic Primary Hyperparathyroidism).
In approximately 15% of patients with primary hyperparathyroidism, all four parathyroid glands are involved. No clinical features differentiate single versus multiglandular disease. The etiology of four-gland parathyroid hyperplasia is multifactorial (see Chapter 65, Surgical Management of Multiglandular Parathyroid Disease). It may be associated with a familial hereditary syndrome, such as multiple endocrine neoplasia, types 1 and 2a (see Chapter 67, Parathyroid Management in the MEN Syndromes). Although the pathophysiology of the sporadic cases is unknown, the calcium set point does not seem to be altered. Instead, it seems that the increased number of parathyroid cells in the hyperplastic glands causes the excessive secretion of PTH. As in the case of parathyroid adenomas, underlying molecular mechanisms are heterogeneous.



