Chapter 32 Surgical Anatomy of the Superior Laryngeal Nerve
 Please go to expertconsult.com to view related video Superior Laryngeal Nerve Anatomy and Monitoring.
Please go to expertconsult.com to view related video Superior Laryngeal Nerve Anatomy and Monitoring.
The technical aspects of operations on the thyroid gland have changed very little since the original papers by Kocher.1 Usually the complication rate of thyroidectomy is very low when an experienced surgeon performs the operation. The most common complications include injury of the recurrent nerve and hypoparathyroidism. However, injury to the external branch of the superior laryngeal nerve (EBSLN) can occur during the dissection and clamping of the superior thyroid vessels. This injury causes paralysis of the cricothyroid muscle (CTM), impairing the production of high tones, and altering the voice’s fundamental frequency, especially problematic for women and professional singers. The effects of EBSLN paralysis are difficult to detect during routine postoperative laryngoscopy, yet functional consequences can be disastrous for those people who depend professionally on their voices. Armed with complete knowledge of the anatomic variations of the superior thyroid pole area, and through meticulous dissection of the superior thyroid pedicle, one may avoid such injury.
History
In 1892, Fort reported the anatomic features of the CTM, including its motor supply by the EBSLN.2 Several publications have studied the anatomy of the EBSLN,3–9 generally in cadaver series. The largest report, by Moosman and DeWeese, included 200 fresh cadavers.6
Little attention was paid initially to the surgical anatomy of the EBSLN during the beginning of the 20th century. In fact, even Kocher1 did not specifically mention this nerve in his book, then considered the cornerstone of thyroid surgery, documenting his personal experience in more than 3000 thyroidectomies. The importance of the preservation of the EBSLN was made clear as a result of a thyroidectomy performed in 1935. At that time, Amelita Galli-Curci was the most famous soprano of the world. She underwent a thyroidectomy under local anesthesia (her surgeon asked her to actually speak during the surgery, to be sure that the recurrent nerves suffered no damage) for a 170-g goiter, with careful identification and preservation of the recurrent laryngeal nerves. However, her vocal registry dramatically lowered postoperatively, and her voice became permanently hoarse. She had to give up singing, and the press of the time wrote, “the surprising voice is gone forever; the sad specter of a ghost replaced the velvet softness.”10 Since that time, the EBSLN has been known as “the nerve of Amelita Galli-Curci.” Interestingly enough, some authors have recently questioned the veracity of this event.11
In 1957, Gregg stated that, despite the large experience of his service (8000 thyroidectomies), he was unsure how to prevent or detect damage to the EBSLN.12 Subsequently, several authors proposed that the dissection of the superior thyroid pole should be performed with great care to avoid including the nerve in the ligature of the superior thyroid vessels.13–17
Some reports in the literature have described methods to identify the EBSLN during a thyroidectomy. Some authors have based their identification only upon the anatomic appearance of the nerve.8,10 Others have tried some form of electrical stimulation to aid in identification,18–22 mainly when dealing with a markedly enlarged thyroid gland.23
Anatomy
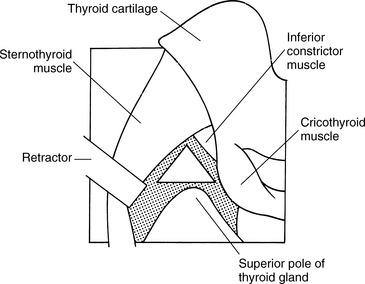
The superior laryngeal nerve (SLN) is one of the first branches of cranial nerve X, the vagus. It usually separates from the vagus at the nodose ganglion, about 4 cm cranially to the carotid artery bifurcation.24 About 1.5 cm inferiorly, the SLN divides in two branches, the internal and the external (EBSLN).7 The EBSLN descends dorsolaterally to the carotid vessels, then crosses them medially, extending to the larynx. The nerve is usually about 0.8 mm wide,25 and its total length varies between 8.0 cm7 and 8.9 cm26 (Figure 32-1). In 1968, Moosman and DeWeese defined the sternothyroid-laryngeal triangle, the limits of which are, medially, the inferior pharyngeal constrictor and the CTM; anteriorly, the sternothyroid muscle; and laterally, the superior thyroid pole6 (Figure 32-2). According to the anatomic study, encompassing 200 cadaver dissections, the EBSLN almost invariably approached the larynx within this triangle.
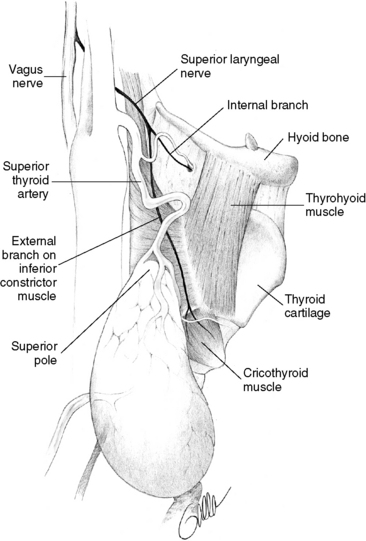
Figure 32-1 EBSLN descends dorsolaterally to carotid vessels, then crosses them medially, routing to the larynx.
The surgical importance of this nerve relates to its proximity to the superior thyroid vessels. In most instances, the EBSLN crosses the superior thyroid artery and vein well above the superior border of the superior thyroid pole, being, at least in theory, protected against surgical injuries. However, Droulias et al. reproduced the surgical conditions of a thyroidectomy in 24 cadavers; they clamped the superior thyroid pedicle adjacently to the superior thyroid pole and found that the nerve was entrapped in most situations.26 Clader, Luter, and Daniels, dissecting 48 cadavers, found that 68% of the EBSLNs were intimately associated with the superior pole vessels and were at risk during thyroidectomy.27 On the other hand, Espinoza, Hamoir, and Dehm28 and Lennquist, Cahlin, and Smeds8 noted lower rates of “at-risk” EBSLNs (15% and 18%, respectively). In addition, Lennquist, Cahlin, and Smeds stated that only 80% of the EBSLN could be identified during a thyroidectomy, because in the remaining 20% the nerve was located within the fibers of the inferior pharyngeal constrictor muscle.8
In 1992, we proposed the following surgical anatomic classification of the EBSLN, based on the relationships among the nerve, the superior thyroid vessels, and the upper border of the superior thyroid pole9:
Type 1. Nerve crossing the superior thyroid vessels 1 or more cm above a horizontal plane passing through the upper border of the superior thyroid pole
Type 2a. Nerve crossing the vessels less than 1 cm above the aforementioned horizontal plane
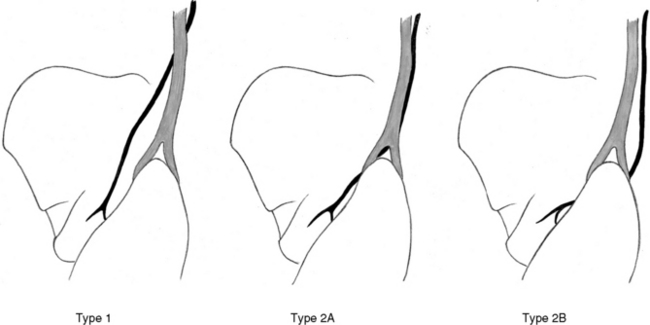
Obviously, type 2b has the highest risk of iatrogenic damage. In our cadaver dissection studies, we found that 20% of the EBSLNs were of this type. In a clinical setting, we have observed 14% of type 2b nerves in a series of normally sized or slightly enlarged thyroid glands.21 Fortunately, type 1 nerves are most common (60% in cadaver anatomic series and 68% in the clinical series).
In 1998, Kierner et al. published a similar classification, adding a fourth category in which the EBSLN runs quite dorsally to the superior thyroid pedicle, making its identification more difficult.29 They observed this anatomic relationship in 13% of their dissections. They observed fewer type 1 nerves (42%) than in our series.
In 2002, Friedman et al. proposed a different classification for the EBSLN, focusing on the relationship between the nerve and the inferior constrictor, at its junction with the CTM. Based on their experience with 1057 nerves, they were able to identify and to classify 900 (85.1%) of the nerves.30
In several recent papers, the anatomic classification we proposed has been widely accepted. Some authors have reported similar proportions of the high-risk type 2b EBSLN as our original results. Ozlugedik et al.31 studied 40 neck halves and observed a 17.5% frequency of type 2b nerves. In a prospective study involving 78 superior thyroid poles in surgical patients, Mishra et al.32 found an even lower percentage of type 2b nerves: 10.25%. In other publications, the frequency of type 2b nerves was significantly higher than our original findings. Pagedar and Freeman33 evaluated 178 EBSLNs in 112 consecutive patients; 48.3% were type 2b. Chuang et al.34 performed an anatomic study of 86 EBSLNs in 43 cadavers; 38.3% were type 2b.
Some authors pointed out that some individual “intrinsic factors” could be related to an increased incidence of type 2b EBSLN. Furlan et al.35 conducted an anatomic study on 36 nonpreserved cadavers. Type 2b nerves were statistically more prevalent among individuals with lesser stature (p = 0.0006) and with increased glandular volume (p = 0.0007).
Morton et al.,36 in a review article, criticized all existing anatomic classifications of the EBSLN. In their view, all classifications failed to establish a reliable anatomic landmark to safely identify and protect the nerve during a thyroidectomy. However, we strongly believe that the way the surgeon approaches the superior thyroid pole is the most important factor concerning the protection of the nerve during a thyroidectomy, especially when dealing with a large goiter.
Physiology and Pathophysiology
The EBSLN is the only motor supply to the CTM. Tschiassny, in 1944,37 and Arnold, in 1961,38 demonstrated the influence of the contraction of this muscle on voice production. The CTM has two bellies, the pars recta and the pars obliqua. The action of each of these two subunits is not fully understood, but the combined contraction of these two components is important in adjusting the vocal fold length and tension.39
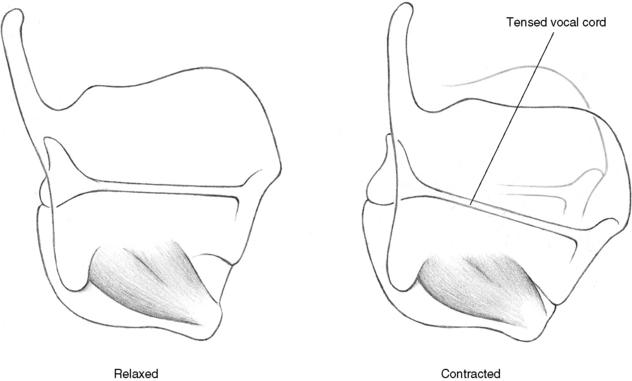
The frequency of vocal fold vibration is influenced by the vocal fold tension, which is controlled in large part by a balance between the actions of two muscles: the thyroarytenoid muscle—which tends to shorten the fold length—and the CTM. The CTM muscle promotes elevation of the cricoid cartilage, shortening the distance with the thyroid cartilage. This motion of the cricoid cartilage increases the vocal fold length and tension (Figure 32-4). Arnold called this CTM-induced vocal cord tension “external tension” of the vocal fold, compared with the more refined increase in “internal tension,” offered by the action of the thyroarytenoid muscle. The CTM-induced vocal cord tension is thought to be of central importance in the production of high-frequency sounds during phonation. Besides this phonatory function of the EBSLN, some authors have suggested a role in respiration, noting respiratory activity, mainly during expiration.40,41
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


