Before discussing the surgical technique for harvesting either of these flaps, the surgeon must have a full understanding of the layers of the scalp and the anatomy of the temporal fossa. Because of the variety of terms applied to the layers of this area, the following is a description using their preferred terminology.
The scalp is a five-layered structure. The most superficial layer is the skin with its hair follicles and sebaceous and sweat glands. The skin is firmly adherent to the underlying subcutaneous tissue that consists of strong collagen bundles and the superficial vessels of the scalp. In the temporal scalp, just deep to this layer is the temporoparietal fascia. Then comes a layer of loose areolar tissue and the superficial layer of the deep temporal fascia, the temporalis muscle, and the deep layer of the deep temporal fascia that is continuous with the pericranium in that region (Fig. 19.1).
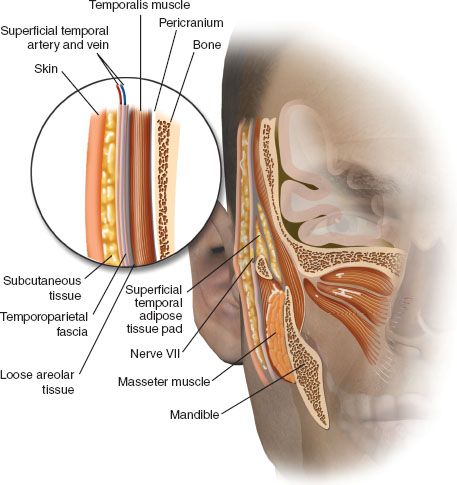
More specifically, immediately deep to the skin and the subcutaneous tissue, just beneath the hair follicles and adipose tissue exists the temporoparietal fascia (sometimes called superficial temporal fascia). This layer is contiguous with the superficial musculoaponeurotic system as it passes over the zygomatic arch into the midface inferiorly. The fascia is contiguous with the galea aponeurotica above the temporal line superiorly and the occipitalis posteriorly. The fascia ranges from 2 to 4 mm in thickness and can be harvested in dimensions up to 17 × 14 cm. Deep to the temporoparietal fascia is a loose areolar and avascular tissue layer that separates the fascia from the temporalis muscular fascia. This areolar layer allows the superficial scalp to move freely over the deeper structures, that is, the more fixed temporalis muscular fascia, that is, the superficial layer of the deep temporal fascia. The temporalis muscle and pericranium are then deep to these fascial layers. Confusing the issue further is the division of the temporalis muscular fascia as it splits into a superficial and deep layer (of the superficial deep temporal fascia) surrounding a pad of adipose tissue at the temporal line of fusion, at about 2 cm above the zygomatic arch (Fig. 19.1). The temporalis muscle fascia is contiguous with the pericranium above the superior temporal line and is contiguous with the masseter muscle fascia deep to the arch of the zygoma.
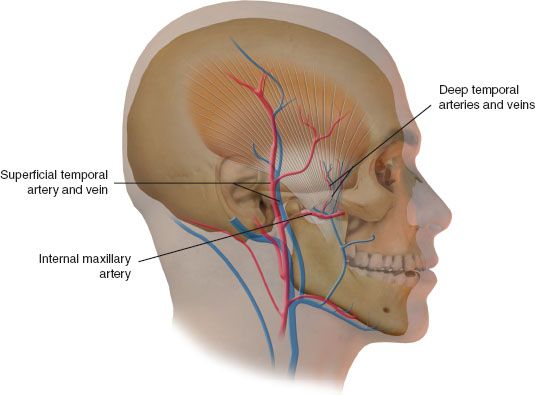
In the lateral aspect of the scalp, the blood supply is by way of the superficial temporal artery, a terminal branch of the external carotid artery that ascends posterior to the ramus of the mandible and becomes superficial 4 to 5 mm anterior to the tragus as it emerges from the parotid tissue. The vasculature fans out in an axial pattern from the inferior aspect of the temporoparietal fascia, giving off the middle temporal artery. Approximately 3 cm above the zygomatic arch, it divides into the terminal frontal and parietal branches (Fig. 19.2). The superficial temporal vein generally runs superficial to and with the artery, but variability, including branching or a posterior course, may be encountered. The auriculotemporal nerve, a sensory branch of the mandibular nerve, lies posterior to the superficial temporal artery within the temporoparietal fascia. The frontal branch of the facial nerve traverses an oblique course over the zygomatic arch, which can be estimated by a line connecting a point 0.5 cm inferior to the tragus to a point 1.5 cm lateral to the superior brow. This nerve also lies within the temporoparietal fascia, and elevation of the flap anterior to the frontal branch of the superficial temporal artery should proceed with caution to avoid injuring this nerve.
SURGICAL TECHNIQUE
Prior to making the incision, a facial nerve monitor is placed in the medial brow to provide continuous monitoring of the frontal branch of the facial nerve. It is secured with a 5-0 silk suture. The incision is then designed as described below. Shaving the hair is avoided by braiding in such a fashion that the incision is clearly demarcated. The patient is then prepped and draped with the patient supine with the head in a lateral position.
Exposure is obtained through a bicoronal incision over the vertex of the cranium in the case of men with hair loss. In women, a curvilinear incision is created beginning from off midline anteriorly on the forehead and then curving in a C-shaped fashion first posteriorly and then anteriorly to the pretragal crease or posttragal region. Inferior extension of the incision is performed as needed. A coronal incision sweeping anteriorly within the hairline is created over a length of approximately 15 cm. (A T-shaped incision over the parietal region has also been described.) A superior–posterior flap just deep to the subcutaneous adipose tissue of the scalp through the dense connective tissue is then elevated. Visualizing and preserving the hair follicles and subcutaneous adipose tissue superficially and the superficial temporal vessels in the flap deep is necessary to prevent alopecia and to maintain the vascular integrity of the scalp and hair follicles as well as those of the flap. One series reported a vessel injury rate of 22.6%. This dissection can be quite tedious. Upon elevation of the scalp, the pericranium is left attached to the lateral skull superiorly in a fan-shaped fashion. The anterior flap is elevated in the same subfollicular plane until the suspected location of the frontal branch of the facial nerve. The location can be estimated by a line from the tragus to the lateral aspect of the eyebrow or by the temporal hairline. The nerve stimulator may be used to assist and to confirm the location of the facial nerve.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


