The Role of Fluorescein Angiography in Diabetic Retinopathy
Omesh P. Gupta MD, MBA
William E. Benson MD
Diabetic retinopathy is the leading cause of visual impairment and blindness among individuals of occupational age.1 Much of this visual loss can be prevented by proper management and treatment. Fluorescein angiography has helped in the diagnosis, management, and study of the pathophysiologic mechanisms of this disease. The specific indications for fluorescein angiography will be described in this chapter, underscoring the established basic guidelines outlined in the recently published Preferred Practice Pattern by the American Academy of Ophthalmology.1,2
Nonproliferative Diabetic Retinopathy
The signs of background diabetic retinopathy include microaneurysms, intraretinal hemorrhages, hard exudates, and macular edema, all of which can be noted clinically.1,3,4 Therefore, fluorescein angiography is not indicated for screening or documentation at this stage. Ophthalmoscopy of a well-dilated fundus performed by trained ophthalmologists and technical personnel has been shown to agree with fundus photography in at least 85% of cases; disagreement occurred in cases of the earliest stages of retinopathy whereby a photographically observable microaneurysm may not be visualized ophthalmoscopically.5,6 The risk of underevaluating retinopathy consistently occurred in eyes with minimal changes. Nonmydriatic fundus photography has been reported to be more sensitive for diabetic screening than mydriatic ophthalmoscopy.7 Clinical identification of more severe changes was almost always consistent and in agreement with the photographic findings.
Stereo fundus photography provides a permanent record of the fundus appearance and can be used to document the severity and progression of disease.1,5,8,9,10 Fundus photography is clearly valuable in documenting rapidly changing retinopathy, or immediately prior to treatment, once the decision to treat has been made on clinical grounds. Large 60° fields will give a more complete view of the midperipheral regions than 30° photography and may be the field of choice for scanning for retinopathy. If the seven-field fundus photography is considered to be 100% sensitive in detecting retinopathy, ophthalmoscopy correlates with retinopathy detected by photography 75% to 86% of the time.5,7 For proliferative diabetic retinopathy, between 79% to 96% agreement was seen between ophthalmoscopic examination and fundus photography.5,10
Given the high specificity and sensitivity of the clinical ophthalmoscopic examination, several screening strategies have been studied.5,6 An annual dilated ophthalmoscopic examination for eyes with no retinopathy has been recommended in several cost-effectiveness models.1,8,11,12 Modifying the screening interval based on hemoglobin A1c may improve the cost-effectiveness of this practice.13 Although in such a cost-effectiveness model photography does not enhance the outcome, fundus photographs are nevertheless medically useful for documenting the course of disease.
Unexplained Visual Loss
Fluorescein angiography can be helpful in determining the cause of unexplained visual loss in an eye with visual complaints out of proportion to the retinal thickening (macular edema).1,6,14,15 An eye may have both minimal peripheral changes and minimal macular edema but visual acuity far worse than the clinical examination. In most cases, the cause is optic neuropathy or macular ischemia, the latter of which can be confirmed by angiography (Figures 113D.1 and 113D.2).
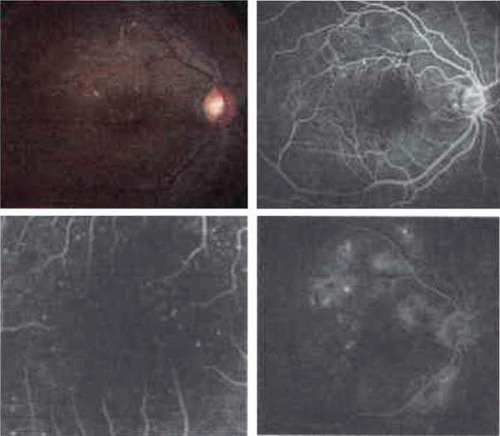 Figure 113D.1. Mild macular ischemia. This was a 46-year-old woman with insulin-dependent diabetes who complained of decreased vision in her right eye. Visual acuity was 20/100. Moderate nonproliferative retinopathy, intraretinal hemorrhages and hard exudates superior to the fovea, and macular thickening were noted on dilated fundus examination with visual loss out of proportion to her clinical examination (A). Fluorescein angiography was therefore obtained, revealing pinpoint areas of hyperfluorescence primarily superior to the fovea and marked irregularity of the foveal avascular zone (B). Higher magnification demonstrated perifoveal nonperfusion and wide intercapillary spaces (C). Angiographic evidence of macular edema was present in the late frame of the angiogram (D). After treatment of the macular edema the visual acuity improved to 20/50. The residual visual loss can be explained by her macular ischemia secondary to diabetic retinopathy. Comment: This is an example of a patient with unexplained visual loss, out of proportion to the clinical examination; a fluorescein angiogram is indicated in this situation. The study is also helpful as a guide to focal laser photocoagulation. |
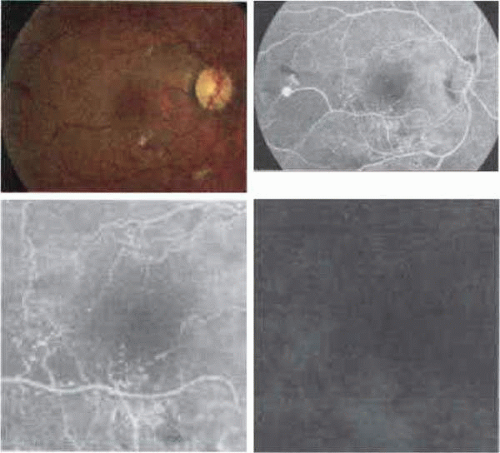 Figure 113D.2. Severe macular ischemia. This was a 57-year-old man with a 15-year history of uncontrolled noninsulin-dependent diabetes who complained of decreased vision in his right eye. Visual acuity was 20/200. Examination revealed proliferative diabetic retinopathy with neovascularization elsewhere and sclerotic vessels along the inferotemporal arcade (A). Microaneurysms, intraretinal hemorrhages, and cotton-wool spots were noted throughout the macula, but primarily inferior to the fovea. Early frame of the angiogram demonstrates pinpoint areas of hyperfluorescence with significant areas of nonperfusion along the distribution of the inferotemporal arcade (B). Severe irregularity to the foveal avascular zone was noted on higher magnification (C). Late frames of the angiogram demonstrated evidence of leakage along the inferotemporal arcade, but minimal leakage was noted from the perifoveal area (D). His visual acuity did not improve from 20/200 with treatment of the macular edema. This can be attributed to severe macular ischemia. |
Occlusion of the perifoveal capillaries is readily shown on angiography4,14,15 as abnormalities of the foveal avascular zone (FAZ). These angiographic characteristics include an irregularity of the margins of the FAZ, budding of capillaries into the FAZ, and the development of wide intercapillary spaces within bridging vessels in the perifoveal capillary bed.4,14 The perifoveal capillaries may actually be more apparent due to both dilation of the remaining capillaries and their contrast to the larger zone of nonperfusion seen angiographically as hypofluorescence. The enlargement of the FAZ is presumed to cause some loss of visual acuity.4,14,15 Depending on the severity, treatment of macular edema in these cases may still improve the visual acuity.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


