14 The Retina: Vascular Diseases I
RETINAL VASCULAR OCCLUSIONS
The posterior ciliary circulation supplies the optic disc and choroid through the short posterior ciliary arteries and the circle of Zinn (see Ch. 17); the central retinal artery leaves the ophthalmic artery in the orbit and only supplies the capillaries on the surface of the optic disc and the retina (see Ch. 20). Retinal vascular occlusions are a common cause of visual loss especially in elderly, hypertensive, diabetic or arteriosclerotic patients. Patients usually present with sudden unilateral visual loss although this might be noticed only coincidentally some time after the initial event particularly in elderly people. All patients need a careful assessment for associated underlying systemic hypertension, diabetes or other atherogenic diseases. Subclinical cardiac and cerebrovascular disease is frequently present and patients should be investigated with these in mind as prophylactic medical or surgical treatment might be indicated to limit or prevent further systemic vascular damage.
ARTERIAL OCCLUSIONS
CENTRAL RETINAL ARTERY OCCLUSION
This is usually a disease of the elderly and is most commonly caused either by thrombosis in the retrobulbar portion of the central retinal artery or blockage of the artery by an embolus which usually originates in the heart or carotid artery. Complete occlusion may be preceded by attacks of amaurosis fugax. All patients should be screened for hypertension, diabetes, cardiac valvular and coronary artery disease and carotid atheromatous disease. Temporal arteritis usually presents as an anterior ischaemic optic neuropathy but occasionally causes a central retinal artery occlusion (CRAO) and needs to be excluded (see Ch. 17). In younger patients, the underlying aetiology is occasionally found to be an inflammatory arteritis of which polyarteritis nodosa, systemic lupus erythematosus and syphilis are perhaps the commonest causes. Spasm of the central retinal artery is an ill-defined and controversial phenomenon that occurs only in exceptional circumstances such as drug toxicity with ergot overdosage or pre-eclamptic toxaemia of pregnancy. CRAO is a rare feature of migraine.
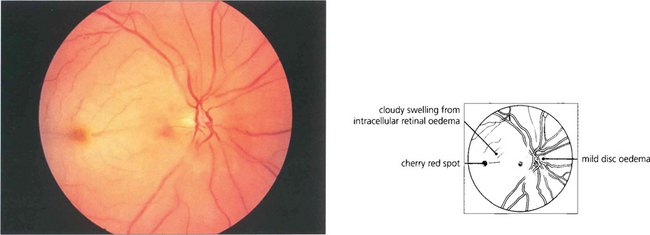
Fig. 14.1 The fundus of a recent CRAO shows a cloudy, opaque and swollen infarcted retina particularly noticeable in the posterior pole where the retina is thickest. The fovea is the thinnest area of the posterior retina and there is little tissue here to infarct so that the underlying redness of the choroid is seen contrasting with the whiteness of the surrounding infarcted retina to give the classical ‘cherry red spot’ appearance. Within a few hours mild swelling of the optic disc often appears due to products of retrograde axoplasmic transport accumulating in the optic nerve head. In the acute stage blood in the retinal arteries is dark from stagnation and the arteries themselves are often attenuated. These acute appearances subside over a period of 2–4 weeks, usually leaving the eye with perception of light. Complete blindness should suggest more extensive vascular occlusion involving the choroidal or optic disc circulation or ophthalmic artery.
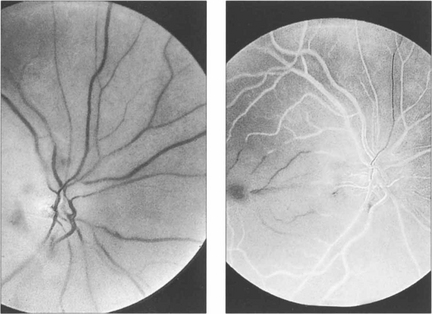
Fig. 14.2 Fluorescein angiography is not usually performed but if it is done in the acute stages there is a considerable delay in filling of the central retinal artery circulation following injection of dye; this is seen as black retinal arteries against the normal background choroidal fluorescence which, of course, is unaffected by the occlusion. The artery fills eventually either directly or by retrograde flow from the venous circulation. The central vessels in the posterior pole fill poorly, possibly due to the retinal oedema increasing external tissue pressure.
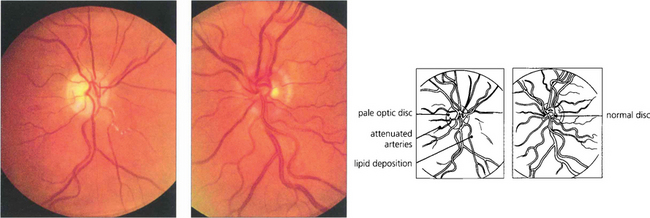
Fig. 14.3 Late changes following CRAO in the right eye. The optic disc is pale and the branches of the central retinal artery are attenuated in contrast to those of the normal left eye. Note the irregular whitish-yellowish deposition in the arterial walls which is probably a mixture of gliosis and lipid deposition from vascular endothelial damage.
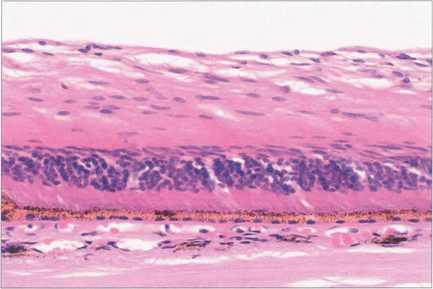
Fig. 14.4 Histology shows atrophy of the inner two-thirds of the retina, (supplied by the retinal circulation), following CRAO. The outer retina is maintained by the choroid (see Ch. 13).
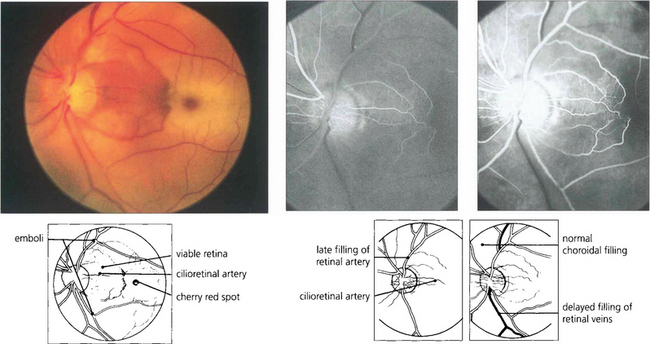
Fig. 14.5 Cilioretinal arteries of varying size are found in about 20 per cent of eyes. These are part of the posterior ciliary circulation and are therefore spared in a CRAO. The patch of retina supplied by the artery is left viable; if the patient is fortunate this will include the macula. A small cilioretinal vessel is seen clearly in this patient supplying an area of retina temporal to the optic disc. Minute cholesterol emboli can be seen in the inferior and superior temporal arteries and also in a small branch artery adjacent to the macula, indicating the aetiology of the occlusion. Fluorescein angiography demonstrates the slow rate of filling of the retinal circulation and the normal filling of the cilioretinal artery and choroid.
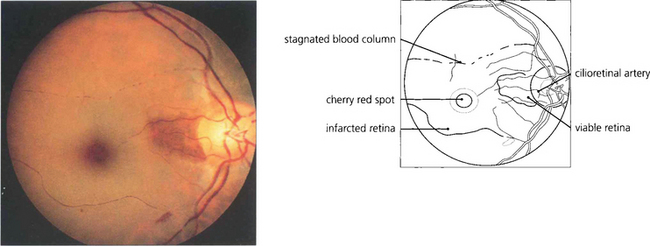
Fig. 14.6 This example of cilioretinal artery sparing in the presence of a CRAO in a pigmented eye demonstrates clumping of the blood column in the inferior temporal branch artery. This characteristic sign of a stagnant retinal circulation is known as ‘cattle trucking’.
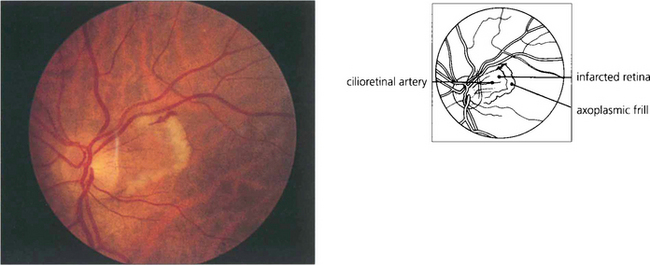
Fig. 14.7 Cilioretinal infarction with central retinal artery sparing is the converse situation to that shown in Fig. 14.5. Here, a small cilioretinal branch is occluded, thus infarcting the retina temporal to the optic disc. A frill of axoplasmic material from the viable retina is seen surrounding the cilioretinal infarct. Cilioretinal infarcts have a similar aetiology to anterior ischaemic optic neuropathy, temporal arteritis, which although it usually presents with more extensive disc infarction, must be excluded as a potential cause.
RETINAL EMBOLI
Embolization of the retinal circulation usually occurs with cholesterol or fibrin and platelet emboli from the carotid arteries, or calcific fragments from a stenosed aortic valve. Occasionally more exotic material such as talcum powder in drug addicts or fat emboli in patients with multiple fractures can be seen. Emboli may produce permanent or transient visual loss; cholesterol emboli are also frequently seen coincidentally on routine examination of an asymptomatic eye. Transient uniocular visual loss is known as amaurosis fugax and is virtually always due to embolization, whether or not emboli are actually seen on examination. Patients typically notice uniocular visual loss starting as a concentric peripheral dimming of vision or a vertical curtain coming over the eye, depending on whether the central retinal artery or a branch retinal artery is affected. Most attacks last for periods of a few minutes but may persist for 2–3 hours before vision quite rapidly returns to normal. Attacks may happen singly or in groups, sometimes occurring in clusters or showers during a day. Patients with retinal embolization have an increased risk of developing a permanent stroke over the next few months and the risk is substantially increased if the amaurosis fugax is accompanied by signs of transient cerebral ischaemia or an embolus is visible in the retina. This means that the ophthalmologist plays an important role in the management of these patients by referring them for prophylactic medical or surgical treatment to forestall the development of permanent neurological sequelae. In young patients, mitral valve prolapse or cardiac septal defects can present as amaurosis fugax. Migraine is another rare cause in young adults and may produce transient visual loss by affecting either the retinal or the choroidal circulation. The features are often atypical and more common causes need to be excluded before a diagnosis is made. Choroidal migraine produces patchy visual loss, rather like pieces missing from a jigsaw puzzle, due to involvement of the choroidal lobular circulation (see Ch. 9).
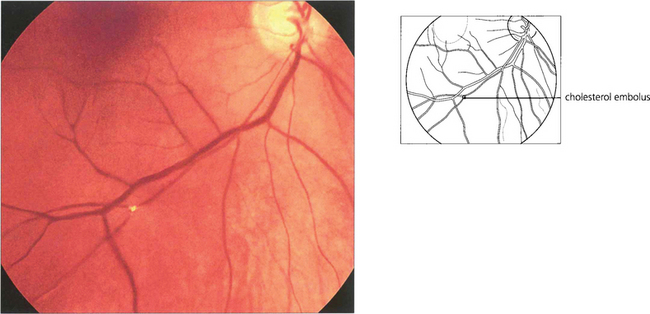
Fig. 14.8 Cholesterol crystals are seen frequently as a coincidental finding in elderly patients and are a sign of atheromatous disease in the carotid circulation (usually at the bifurcation of the common carotid). They are flat crystals that glint and reflect light as the ophthalmoscope is tilted to examine the fundus and are most commonly found at bifurcations of the retinal arteries. Because of the planar shape of the crystal, blood flow may not be disturbed and the patient does not complain of any symptoms. Cholesterol emboli are also known as ‘Hollenhorst’ plaques after the Mayo Clinic ophthalmologist who made the first description.
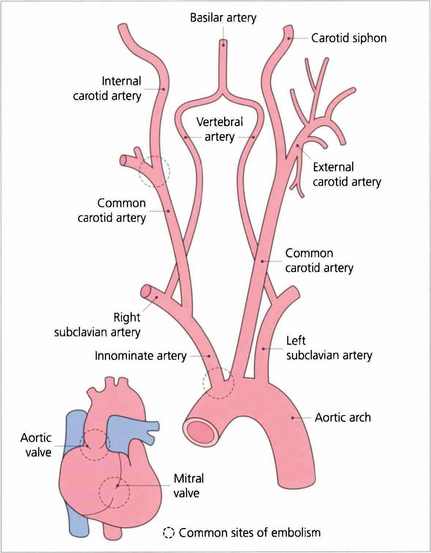
Fig. 14.9 Cholesterol emboli usually arise at the bifurcation of the common carotid artery, less frequently at the origin of the great vessels. Calcific emboli usually arise from the aortic valve or ascending aorta.
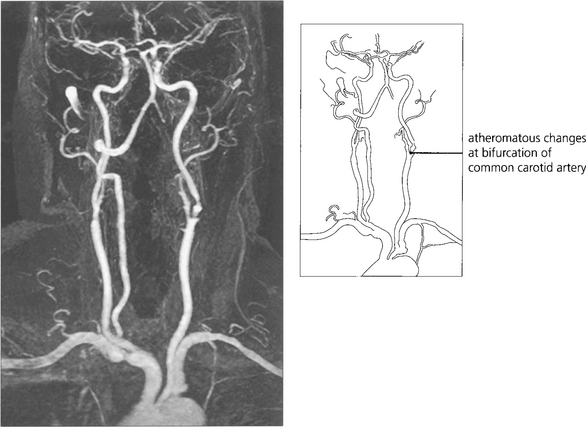
Fig. 14.10 If the patient is likely to be a candidate for vascular surgery, imaging of the carotid bifurcation is indicated to define an atheromatous lesion. This can be done by Doppler ultrasonography or magnetic resonance angiography. These have now superseded formal arterial angiography which carries a significant risk of stroke in its own right. Clinical trials have established that if the patient is fit for surgery, symptomatic stenoses of greater than 70 per cent are best treated by surgical carotid endarterectomy. Milder degrees of stenosis and unfit patients are better treated medically with inhibitors of platelet aggregation.
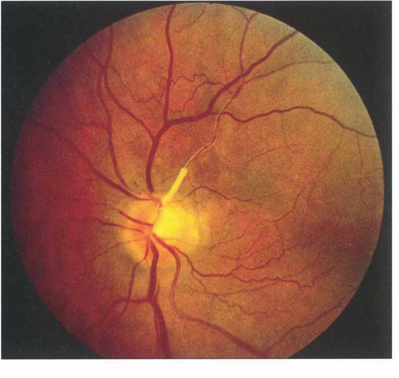
Fig. 14.11 Lipid deposition may be seen in the retinal arterial wall following vascular endothelial cell damage after embolization. In this patient there is marked yellowish white sheathing at the origin of the superior temporal artery and, peripheral to this, the vessel is thin, attenuated and fibrosed. Collateral vessels can be seen on the retina and the optic disc has sectorial pallor; the patient had a dense inferior nasal arcuate scotoma. Sometimes the lipid deposition occurs at a bifurcation of a major retinal arteriole giving a ‘trouser leg’ pattern of sheathing to the vessel.
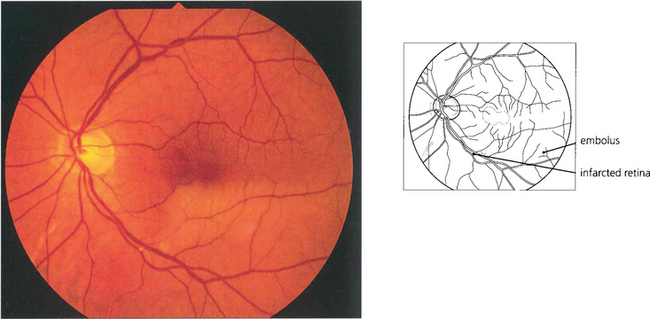
Fig. 14.12 Occlusion of a branch retinal artery is almost always the result of embolization. In this patient with a branch inferior temporal artery occlusion, a small embolus can be seen in the artery at a bifurcation. The embolus is white and globular, unlike a cholesterol embolus, and plugs the vessel. It originated from a stenotic aortic valve.
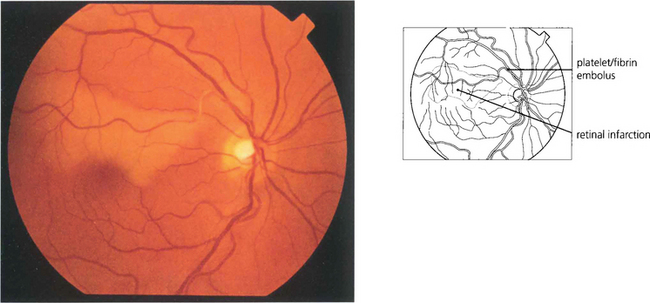
Fig. 14.13 Platelet and fibrin emboli originate from an ulcerating atheromatous plaque and look like soft porridgy material in the vessel. They produce retinal infarction or amaurosis fugax and can sometimes be observed moving slowly through the retinal arterial circulation as the attack evolves. Video fluorescein angiography shows that transient multiple platelet embolization is common during cardiac bypass procedures.
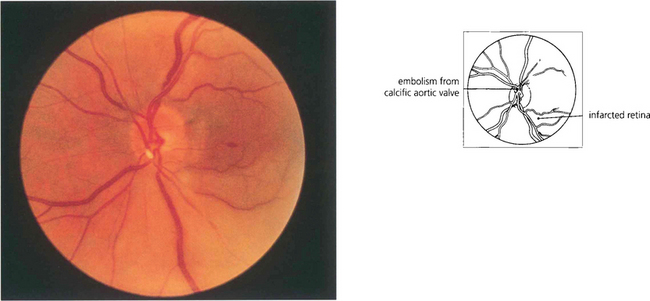
Fig. 14.14 Embolization from fragments of a calcific aortic valve are seen occasionally; their characteristic appearance is different from that of other types of emboli, so aiding their identification. They tend to be larger and globular with a pearly white appearance and lodge in the larger arteries at the optic disc. Echocardiography confirms the diagnosis.
VENOUS OCCLUSIONS
CENTRAL RETINAL VEIN OCCLUSION
Elderly patients with central retinal vein occlusion have an increased incidence of arteriosclerosis, smoking, hypertension and diabetes. The role of associated arterial disease in the pathogenesis remains controversial but, as the central retinal artery and vein share a common fascial sheath within the optic nerve, thickening and hypertrophy of the artery can compromise the vein’s diameter leading to obstruction. Patients often notice visual loss on waking with vision having been normal the night before and it has been postulated that lower ocular perfusion due to lower blood pressure and pulse rate and increased intraocular pressure during sleep contribute to this (see Ch. 7). CRVO is also a well recognized association of raised intraocular pressure; this is particularly important to recognize as lowering the IOP in the fellow eye may prevent a subsequent occlusion in this eye.
Although CRVOs are most common in those aged over 60 years, younger patients may also be affected.
Patients with retinal vein occlusion have an increased incidence of death from cardiac or cerebral causes. Furthermore, there is a 15 per cent risk of recurrence in the same or fellow eye over 5 years. All patients require medical investigation (Table 14.1).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


