Pediatric Ophthalmology
Edited by P. F. Gallin
Thieme Medical Publishers, Inc.
New York ©2000

16

The Red Eye
The eye, of an adult or of a child, may become red for a variety of reasons; some are trivial and some are vision threatening. There are six major etiologic categories that can cause red eye in infants and children: conjunctivitis, keratitis, uveitis, scleritis, angle closure glaucoma, and malignancy. Detailed discussion about uveitis, scleritis, angle closure glaucoma, and malignancy are given elsewhere in this book. We will thus concentrate on conjunctivitis and keratitis as causes of red eye in this chapter.
 Conjunctivitis
Conjunctivitis
Nonatal Conjunctivitis
Neonatal conjunctivitis (ophthalmia neonatorum) occurs in early infancy prior to 1 month of age.1 The most common cause of neonatal conjunctivitis is chemical conjunctivitis, secondary to silver nitrate gonorrhea prophylaxis, which occurs in approximately 90% of infants who receive this treatment.2
The conjunctival flora of newborns reflects the exposure during the birth process; 80% of infants delivered by cesarean section within 3 hours of membrane rupture have sterile conjunctiva.3 Vaginally delivered infants have conjunctival flora similar to that of female genital tract.3,4 This is obviously important in regard to sexually transmitted diseases, and hence, in all developed countries, prophylactic treatment is initiated immediately upon delivery.
Infectious neonatal conjunctivitis occurs in about 1 to 12% of infants,5,6 and can be caused by a number of infectious agents: Chlamydia trachomatis, Streptococcus species, Staphylococcus species, Escherichia coli, Haemophilus species, Neisseria gonorrhea, and herpes simplex virus. The availability and wide application of topical antibiotics or chemical prophylaxis at birth have helped to decrease the incidence of the once vision-threatening epidemic of N gonorrhea ocular infection.
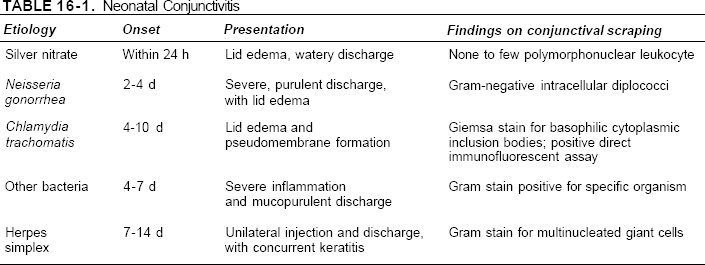
Table 16-1 summarizes the etiology relative to the time of onset and the clinical presentation of various causes of neonatal conjunctivitis. However, because gonococcal infections are rapidly destructive, conjunctivitis in the newborn should be considered an ophthalmic emergency. The physician should not rely exclusively on the timing of the infection or the clinical appearance to make a specific diagnosis. Empiric treatment with topical erythromycin should be begun while awaiting culture results.
Laboratory
Any infant who presents with conjunctivitis must have a very careful evaluation, including conjunctival scraping for Gram- and Giemsastained smear and for culture on chocolate agar or Thayer-Martin for N. gonorrhea and culture on blood agar for other bacteria. Chlamydial infection can be assessed by a Giemsa stain of the conjunctival scraping for intracytoplasmic inclusion bodies, which can often be done immediately by the physician in the emergency room, or direct immunofluorescence antibody assay. If a corneal epithelial defect is present, culture for herpes simplex virus is indicated.
The physicians should initiate treatment of neonatal conjunctivitis immediately prior to laboratory results, as certain organisms can penetrate an intact corneal epithelium. Empirical antibiotic coverage may include topical erythromycin ointment and intravenous or intramuscular third-generation cephalosporin (Ceftriaxone, 30 to 50 mm/kg/d).2 Therapy can then be altered based on laboratory results.
Types of Conjunctivitis
Chemical Conjunctivitis
Chemical conjunctivitis occurs within the first 24 hours of the infant’s delivery and is usually bilateral. There is often watery discharge and bulbar conjunctival injection. This conjunctivitis is caused by silver nitrate 1% drop prophylaxis. Fortunately, chemical conjunctivitis generally resolves spontaneously within 2 to 3 days.2
Chlamydial Conjunctivitis
Chlamydial conjunctivitis is the second most common type of neonatal conjunctivitis in developed countries, following chemical conjunctivitis.7 It has an onset later than that of gonococcal conjunctivitis, usually 4 to 7 days after birth. Chlamydial conjunctivitis is more indolent and less severe than gonococcal conjunctivitis. There may be significant lid swelling, conjunctival hemorrhage (Fig. 16-1), and pseudomembrane formation. The physician can make the diagnosis by observing intracytoplasmic inclusion bodies by Giemsa stain. Giemsa stain of chlamydial conjunctivitis will demonstrate basophilic cytoplasmic inclusion bodies in epithelial cells in 50 to 90% of culture-proven cases.8 However, currently, the diagnostic method of choice is the direct immunofluorescent monoclonal antibody stain (e.g. MicroTrak), which has 87 to 100% sensitivity,9 enzyme immunoassay (e.g., Chlamydiazyme), or DNA probe. McCoy cell cultures are the standard for culturing Chlamydia.8

FIGURE 16-1. Conjunctivitis caused by Chlamydia trachomatis with marked conjunctival injection and hemorrhage.

FIGURE 16-2. Conjunctivitis caused by Neisseria gonorrhea with severe purulent, serosanguineous discharge, and lid edema and chemosis.
Chlamydial neonatal conjunctivitis may resolve spontaneously over several weeks. However, active treatment is indicated to prevent late onset pneumonitis, rhinitis, or otitis.10 Therapy includes topical eythromycin or tetracycline ointment and oral erythromycin 30 to 50 mg/kg/d in four divided doses for 2 to 3 weeks. Both parents should also be treated with oral erythromycin or doxycycline for 2 to 3 weeks.2
Gonococcal Conjunctivitis
Effective prophylaxis programs have helped to decrease the incidence of gonococcal neonatal conjunctivitis in the United States and all other developed countries.7 Gonococcal conjunctivitis typically presents as severe, purulent conjunctivitis with lid edema and chemosis and serosanguineous discharge (Fig. 16-2). The conjunctivitis usually occurs approximately 48 to 72 hours after birth; however, if there is a premature rupture of amnionic membrane, the conjunctivitis may have an earlier onset.2
In addition to the conjunctivitis, N. gonorrhea can also cause severe keratitis, with corneal ulcer and perforation. Thus, the physician must always use fluorescein staining in evaluating the cornea.
As gonococcal conjunctivitis can lead to devastating sequelae, its diagnosis and treatment must be made promptly. Immediate Gram stain of conjunctival scraping is critical because it will often reveal typical Gram-negative intracellular diplococci (Fig. 16-3), which is virtually diagnostic of N. gonorrhea. Chocolate agar-plated cultures in a CO2 enriched atmosphere or Thayer-Martin media placed in a 37°C incubator should be used for definitive gonococcal cultured isolation.

FIGURE 16-3. Gram negative intracellular diplococci from conjunctival scrapings, diagnostic of Neisseria gonorrhea.
Appropriate therapy for N. gonorrhea conjunctivitis is topical eythromycin ointment and systemic third-generation cephalosporin (Ceftriaxone, administered either intravenously or intramuscularly, 30 to 50 mg/kg/d in divided doses).2 Some authors have reported effective treatment with a single dose of 1 gram of Ceftriaxone.11 Intravenous penicillin G 50,000 units/kg/d every 12 hours for 7-days is an alternative treatment2 but one must be aware that resistant N. gonorrhea exists. In addition, the physician must consider concurrent infection with Chlamydia or syphilis whenever gonorrhea infection exists. Syphilis infection will require a much-prolonged course of treatment. Coexistent chlamydial infection will necessitate therapy for mother, father, and in some cases, sexual partners.
Herpes Simplex Conjunctivitis
Approximately 70% of cases of herpes simplex neonatal conjunctivitis are secondary to type II herpes simplex virus (HSV).2 The conjunctivitis often occurs later than does gonococcal or chlamydia conjunctivitis, between 1 and 2 weeks postpartum.2 Many cases are unilateral, with conjunctival injection and discharge. A concurrent keratitis is often present, with positive typical dendritic fluorescein staining of the corneal epithelial defect. One should request viral cultures of conjunctival scraping to obtain the diagnosis. However, viral cultures may take 7 to 10 days to become positive; treatment should be initiated immediately if there is sufficient clinical suspicion and should include topical trifluorothymidine (Viroptic) drops nine times daily or vidarabine (Vira-A) ointment five times daily and systemic acyclovir.
Prophylaxis
In 1881, Crede first used 2% silver nitrate for prophylaxis against neonatal conjunctivitis caused by N. gonorrhea.12 Prior to that time, gonococcal conjunctivitis was a leading cause of blindness, occurring in 10% of newborns. Prophylaxis with silver nitrate and other agents has greatly decreased the incidence of gonococcal conjunctivitis to approximately 0.06%.6 In recent years, the administration of silver nitrate to the eyes of neonates is no longer popular for two reasons. First, silver nitrate may cause a chemical conjunctivitis that may masquerade the diagnosis. Second, with the declining incidence of gonococcal conjunctivitis worldwide, C. trachomatis is now the leading cause of neonatal conjunctivitis, and silver nitrate does not provide prophylaxis against Chlamydia.6 In 1980 and again in 1986, the American Academy of Pediatrics endorsed the use of 1% tetracycline or 0.5% erythromycin ointment as prophylaxis against neonatal gonococcal conjunctivitis. Currently, there are three accepted forms of neonatal conjunctivitis prophylaxis: 1% silver nitrate, 0.5% erythromycin ointment, and 1% tetracycline ointment; all three seem to have similar efficacy.6,13 Recently, 2.5% povidone-iodine has been used for ophthalmia neonatum prophylaxis, and this has been shown to be superior to silver nitrate and erythromycin.14 Povidoneiodine is effective against a broad spectrum of pathogens, including viruses such as human immunodeficiency virus and herpes, and may thus become the gold standard for prophylaxis of neonatal conjunctivitis.14
Pediatric Conjunctivitis
Conjunctival inflammation in a child is a nonspecific finding and can be secondary to a variety of disease processes. Infantile glaucoma, bacterial conjunctivitis, infectious keratitis, and uveitis all may share similar signs and symptoms. It is obviously important that the correct diagnosis be established for proper management. It may be necessary to restrain the child or to perform examination under anesthesia so that careful examination (by standard or handheld slit lamp) can be done, including checking intraocular pressure, looking for anterior chamber cells, and staining of the conjunctival and corneal epithelium.
The common causes of pediatric conjunctivitis are listed in Table 16-2. Approximately 50% of acute conjunctivitis in children is secondary to bacterial infection, 20% is caused by adenovirus, and 30% is culture negative.15 Acute hemorrhagic conjunctivitis is most often caused by Haemophilus influenzae and adenovirus,2 whereas chronic conjunctivitis in childhood is most commonly caused by chronic blepharitis and allergic conjunctivitis.
| Bacterial Staphylococcus species Haemophilus species Pneumococcus species Streptococcus species Chlamydia trachomatis Bartonella henselae Viral Adenoviruses type 3, 7, 8, and 19 Molluscum contagiosum Human papillomavirus Noninfectious Allergic Hay fever conjunctivitis Vernal conjunctivitis Giant papillary conjunctivitis Meibomian gland dysfunction Conjunctivitis associated with systemic diseases Stevens-Johnson syndrome Graft-versus-host disease |
Bacterial Conjunctivitis
Distinguishing features of bacterial conjunctivitis are acute purulent inflammation of the bulbar tarsal conjunctiva and mucopurulent discharge. The most common pathogens include species of Staphylococcus (Fig. 16-4), Haemophilus, Pneumococcus, and Streptococcus.15,16
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


