Early postoperatively with sutures in place:
Symmetry of suture positions
Homogeneity of suture tension
Late postoperatively persisting without sutures:
Cut quality
Wound configuration (horizontal/vertical)
Symmetry of graft placement
The low quality of the trephination wound and geometric incongruities (horizontal and vertical) require higher suture tension in order to guarantee a watertight wound closure and pseudo-optimal topography during the early postoperative phase. Asymmetrical regional forces between the donor and recipient can lead to inhomogeneous wound healing processes. The removal of the sutures results in the release of forces due to geometric incongruities and inhomogeneous wound healing. For this reason, horizontal, vertical, and topographic discrepancies between the donor and recipient intraoperatively appear to be responsible for the increase in astigmatism after removal of the sutures. Thus, it is reasonable to conclude that in addition to wound healing, factors associated directly or indirectly with the quality of the wound geometry (quality of the cut, wound configuration (horizontal/vertical), symmetry of the graft fit) have a strong influence on long-term astigmatism after removal of the sutures [10, 11, 58].
The main intraoperative determinants (Table 6.2, Fig. 6.1) for high and/or irregular astigmatism after suture removal are [42, 61, 63]:
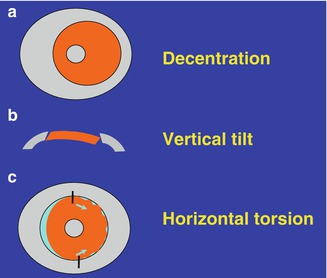
Decentration (donor and/or recipient trephination)
“Vertical tilt” (incongruent cut angle between donor and recipient)
“Horizontal torsion” (horizontal discrepancy between the donor and recipient form and/or asymmetrical graft fit – “The second cardinal suture is crucial!”)
Table 6.2
Intraoperative determinants of high and/or irregular astigmatism after penetrating keratoplasty
Decentration of donor and/or recipient trephination |
“Vertical tilt” due to incongruent wound configuration [42] Application of different trephines for the donor and recipient Trephine tilt (i.e., not parallel to the optical axis) Limbus level not supported horizontally Slipping of the trephine in the stroma during the incision process Intraocular pressure too high/too low |
“Horizontal torsion” [42] Asymmetrical placement of the second cardinal suture (angle unequal 180°) Incorrect fit of the donor and recipient due to incongruity |
Focal overlap or dehiscence of the donor disk in the recipient bed |
Excessively over/undersized donor disk |
Distortion or compression of the cornea |
Trauma to the cornea caused by instruments |
Properties of the suture Suture material Suture technique (interrupted suture, single running suture, double running suture, combinations) Length of the stitch Depth of the stitch Angle of the stitch to the donor-recipient junction “Depth disparity” Tightness of the suture |
Simultaneous intraocular surgery (e.g., triple procedure, artificial lens replacement, etc.) |
Flieringa ring and lid speculum |
Personal experience of the microsurgeon |
Fig. 6.1
Main reasons for high astigmatism after keratoplasty. (a) Decentering of the donor and/or recipient trephination, (b) “vertical tilt” due to uneven cutting angle, (c) “horizontal torsion” due to asymmetrical suture placement
Trephination Technique
In principle, keratoplasty may be indicated for optical, curative, and tectonic reasons. In practice there can be overlaps between different categories. However, corneal grafts can also be classified according to the type of donor tissue, the vertical/horizontal shape of the graft, and the location of the graft within the recipient [40, 42].
An “optimal trephination” requires:
Full visual control
No contact
Optimal donor and recipient centration
Identical shape of donor and recipient (typically circular round)
Congruent incision angles
360° symmetrical donor-recipient alignment
No completion of the trephination using scissors required
No damage to intraocular structures (iris, lens)
In the future: self-sealing donor-recipient apposition (“keylock principle”)
Donor Trephination
From a 16 mm corneoscleral disk, as provided by the cornea bank, the graft can be produced in two ways:
In the past it was punched from the endothelial side against a firm surface, e.g., paraffin or Teflon block, with the help of special trephines (e.g., “punch trephine”). Here, particular attention must be paid to ensuring that the excision is performed in a centered position and that the trephine is not tilted, as this would result in an elliptical disk with slanted edges [11]. This risk can be reduced through the use of “guided donor trephine systems” (e.g., guillotines). In the histological assessment, the cut surfaces without consideration of the cut angles appear to be almost “perfect.” However, the deviation in the direction of the cut toward the exterior results in a convergent cut angle due to the smaller diameter on the level of Descemet’s membrane and a greater diameter on the level of Bowman’s layer (“undercut,” Fig. 6.2) [82].
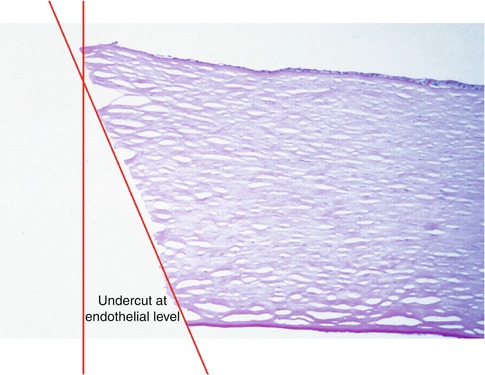
Fig. 6.2
Donor trephination from the endothelial side: smooth cutting surface, but “undercut” at the level of Descemet’s membrane
Since the introduction of “artificial anterior chambers,” microsurgeons have been able to carry out donor trephination from the epithelial side, i.e., in the same direction as in the patient. If the pressure in the artificial anterior chamber is kept at its normal level (e.g., 22 mmHg), the advantages with respect to the congruence of the cutting angles are self-evident [48].
Recipient Trephination
In order to increase the overview and reduce vis à tergo, a Liebermann lid speculum can be used. Almost any viscoelastic agent is suitable for stabilizing the anterior chamber during trephination and suture placement.
A Flieringa ring is not necessary for keratoplasty only or a triple procedure, however, for aphakic and/or vitrectomized eyes, especially if a secondary sclera-fixated or retroiridal artificial lens implantation is planned.
Investigations by van Rij and Waring have shown that in recipient trephination, the use of all trephine systems results in openings which are larger than the nominal trephine size. Furthermore, the diameter at the level of Descemet’s membrane is greater, resulting in divergent cut angles [49, 82]. This can be explained at least in part by bulging (“ballooning”) of the cornea in the trephine opening due to the pressure exerted.
The higher the intraocular pressure, the more divergent angles can be expected in recipient trephination [48].
This phenomenon of “ballooning” is one of the main disadvantages of the mechanical trephine and can at least partially be prevented by the use of a so-called obturator (exception: keratoconus).
The combination of a donor disk that has been punched from the endothelial side and therefore has convergent cut angles, with a recipient opening with divergent cut angles, leads to a triangular-shaped tissue defect at the level of Descemet’s membrane. This has to be compensated for intraoperatively by means of increased suture tension, which can result in flattening, vertical tilt, and irregular astigmatism (Fig. 6.3).
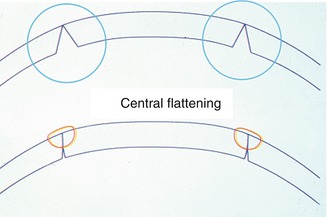
Fig. 6.3
The combination of the donor cornea (convergent cutting angle) trephined from the endothelial side and the mechanically trephined recipient cornea (divergent cutting angle) causes a triangular deficit at the level of Descemet’s membrane, which has to be compensated for by suture tension. This can lead to central flattening, vertical tilt, and irregular astigmatism
Technical Details of PKP
General anesthesia has clear safety advantages over local anesthesia, especially in young keratoconus patients. The arterial blood pressure should be kept as low as possible when the eye is open (“controlled arterial hypotension”).
Typically, the pupil is constricted with pilocarpine in order to protect the lens of the phakic eye.
Paracentesis at the limbus is recommended before trephination.
The head and limbus level must be horizontal during trephination.
A peripheral iridotomy at 12 o’clock prevents pupillary block and therefore an acute glaucoma attack. In case of keratoconus after the administration of atropine, this may appear as a so-called Urrets-Zavalia syndrome with a persistent maximally dilated pupil due to an iris sphincter necrosis [80].
The correct position of the second cardinal suture is absolutely crucial for a correct graft alignment.
Graft Size and Oversize
Graft Size
In a quantitative study we were able to show that the corneal diameter in keratoconus patients is significantly greater than the diameter in Fuchs’ patients (mean horizontal diameter of 11.8 mm in keratoconus compared to 11.3 mm in patients with Fuchs’ dystrophy [54]). In general, larger graft dimensions have a favorable effect on the optical qualities and endothelial cell count, while a low rate of immunological rejection and lower risk of postoperative ocular hypertension are affected by a small graft.
The graft size should be determined on an individual basis: “as large as possible, but as small as necessary.”
For many eyes with keratoconus, an 8.0 mm diameter has proven to be a good preset for communication with the cornea bank (arcus lipoides!), while for many eyes with Fuchs’ dystrophy not suitable for posterior lamellar keratoplasty, a 7.5 mm diameter is appropriate. Today, diameters from 5.5 to 7.0 mm are only very rarely needed and are usually reserved for small eyes with special immunological implications.
It has been assumed that a smaller graft is associated with higher astigmatism after keratoplasty. In a more recent study, in which we compared 8.0, 7.5, and 7.0 mm grafts with each other, we were able to show the following [58]:
Smaller grafts are associated with a flatter curvature.
Smaller grafts are associated with higher topographic irregularity.
Smaller grafts result in a higher proportion of non-measurable keratometry images.
Suture removal is associated with a positive tendency toward regularization of the topography.
It has not been possible to show a difference with respect to the amount of net astigmatism between smaller and larger grafts, neither for grafts with nor without suture.
Recent studies show that the rate of chronic endothelial cell loss after PKP depends on the initial diagnosis [34, 47]. Endothelial migration along a density gradient from the donor to the recipient ring is probably the main reason for this phenomenon in pseudophakic bullous keratopathy. For this reason, eyes with bullous keratopathy are probably better treated with a larger graft, not only in order to improve the optical quality but also to transplant as many endothelial cells as possible. Nevertheless, the graft size must be determined individually by the microsurgeon for each individual patient before recipient trephination in order to find the best compromise between immunological purposes and optical quality. A slit lamp with a measuring device, such as the Haag-Streit slit lamp, can be helpful. Furthermore, the removal of a vascularized pannus is recommended (in contrast to vascularized stromal corneal scars) before trephination in order to achieve a greater “individually ideal” graft diameter [52].
Graft Oversize
In mechanical trephination the diameter of the recipient bed tends to be larger than the trephine diameter. In contrast, the diameter of the donor disk, which is punched from the endothelial side, tends to be smaller than the trephine diameter, which has a corresponding effect on the spherical equivalent [21, 82]. For this reason, “donor oversizing” of 0.25–0.50 mm is usually carried out in this situation. This is performed on the one hand to prevent the flattening of the graft and on the other hand to prevent narrowing of the iridocorneal angle where there is a predisposition to secondary glaucoma [24, 46]. In contrast, no oversizing is required with the use of guided trephine systems or laser trephination in which the donor is cut from the epithelial side. In the case of keratoconus, it has been recommended not to carry out donor oversizing.
Undersizing of the graft for the purpose of simultaneous correction of keratoconus-intrinsic axial myopia will result in irregular astigmatism and is not recommended. The difficulty of achieving a watertight wound closure requires excessive suture tension, with the consequence of irregular astigmatism and a relative cornea plana.
Pupil or Limbal Centration?
Centration is essential, both in terms of the immunological graft reaction and the astigmatism after keratoplasty [31, 32, 53, 81]. Typically, an attempt is made to reach a compromise between limbus and pupil centration in nontraumatized pupils. However, limbus centration is preferred especially in the case of keratoconus, scars after trauma, or irregular astigmatism due to other causes. In such eyes, the center of the entrance pupil is in fact optically displaced from the position of the actual anatomical pupil [33]. For example, the pupil in the typical keratoconus eye tends to be optically displaced superonasally due to the inferotemporal location of the cone.
We use a radial keratotomy marker with eight lines in order to ensure limbal centration (Fig. 6.4). Additional central punctate marking can be helpful for certain trephine systems (e.g., Hessburg-Barron trephine, GTS after Krumeich).
Fig. 6.4
Radial keratotomy marker for recipient centration with respect to the limbus
Keratoconus
In keratoconus, a large (typically 8.0 mm) central circular keratoplasty is indicated as soon as hard oxygen-permeable contact lenses are no longer tolerated. If nonmechanical excimer laser trephination is used, corneas which are extremely steep before keratoplasty do not have worse prognosis than those which are less deformed [84].
A larger graft diameter in keratoconus contributes toward obtaining a sufficiently thick cornea on the trephination edge, since as a result the cone can usually be completely excised. We advise against centering the trephination at the center of the cone, as this typically necessitates decentering of the trephination with regard to the limbus. This would have unfavorable impacts on the astigmatism [81]. Cauterization of the cone has been suggested in order to avoid divergent cutting angles, but the achieved effect is not reproducible. For this reason we do not recommend cauterization of the cone. An obturator should not be used with keratoconus in order not to produce undesirable irregularly elliptical or even pear-shaped host openings (Fig. 6.5). In this context, “non-contact” excimer laser trephination is preferred over the mechanical method in order to avoid noncircular recipient openings.
Fig. 6.5
In case of keratoconus it has been recommended not to use an obturator in order to avoid elliptical or pear-shaped excision shapes. The same principle of applanation during trephination applies in femtosecond laser application (Courtesy of Professor Herbert Kaufman)
In keratoconus, the inhomogeneous corneal thickness typically results in premature perforation at the thinnest point of the cornea, which has to be considered when using conventional trephines in order not to inadvertently traumatize the iris or even the lens.
Suture Technique
The type of trephination has a major impact on the correct placement of the first four or eight cardinal sutures [45, 63]. The main purposes of these cardinal sutures include:
The symmetrical horizontal distribution of donor tissue in the recipient bed
Good adaptation of the donor and recipient wound edge on the level of the Bowman’s layer
Stabilization of the anterior chamber to ensure that further suturing is uniform.
Concerning donor-host alignment, external steps must be avoided, although internal steps sometimes have to be tolerated in the case of thin recipient corneas, for example, in pellucid marginal degeneration or herpetic scars.
As far as the correct placement of the second cardinal suture is concerned, unintentional deviations from circular recipient openings can represent a challenge even for the experienced keratoplasty surgeon. After removal of the cardinal sutures, the quality of the trephination and the correct positioning of the graft are the main determinants for a watertight wound closure. The better the trephination, the lower the final suture tension which is necessary to ensure a watertight wound closure after removal of the cardinal sutures. The lower the final suture tension is, the more quickly an improvement in visual acuity can be expected. In the case of an intact Bowman’s layer, a 16-stitch double-running diagonal cross-stitch suture (10-0 nylon) after Hoffmann is typically preferred in Germany [18] (Fig. 6.6). The faster visual rehabilitation with running sutures – in contrast to multiple interrupted sutures and combined suture techniques – is attributable to the regular topography of the cornea and the avoidance of a relative cornea plana. In addition, with this double-running suture, the risk of suture loosening is reduced [22].
Fig. 6.6
Excimer laser keratoplasty (8.0/8.1 mm) with typical double-running 10-0 nylon cross-stitch suture, each with 8 stitches (after Hoffmann [18]) in keratoconus
The better the trephination, the more easily a watertight wound closure is achieved.If excessive suture tension is required in order to achieve a watertight wound closure, the regularity of the topography and, therefore, the visual acuity after keratoplasty are generally impaired.
Conventional Mechanical Trephines
Unfortunately, conventional mechanical trephination is always associated to some extent with the deformation of corneal tissue, including distortion of the cut edges, with irregular cutting surfaces as a consequence of the axial and radial forces which are induced by the use of these trephines [42, 63]. The cut angles deviate from the perpendicular and are often different in the donor and recipient, especially when the donor trephination is performed from the endothelial side [11, 21, 45, 46]. The fitting of the donor tissue into an unstable recipient bed is sometimes very difficult to achieve in a perfectly symmetrical manner. After the suturing in of incongruent cut edges and the resulting induction of a vertical tilt [31, 32], the healing of the wound can result in pronounced distortion of the graft topography, especially after suture removal [10, 15, 36, 39]. Moreover, the asymmetrical placement of the cardinal sutures can lead to the uneven distribution of donor tissue in the recipient bed, in particular if the second cardinal suture is not positioned exactly 180° opposite the first stay suture (“horizontal torsion” [42]).
If conventional trephines are used, it is recommended that systems should be applied which in the case of donor trephination from the epithelial side provide for the use of an artificial anterior chamber for fixation of the corneoscleral disk. The trephines should always be as sharp as possible in order to keep inappropriate squeezing and shearing forces as small as possible. Disposable items may be advantageous here – also with regard to prion-caused contagious diseases.
Nonmechanical Excimer Laser Trephination (Fig. 6.7a, b)
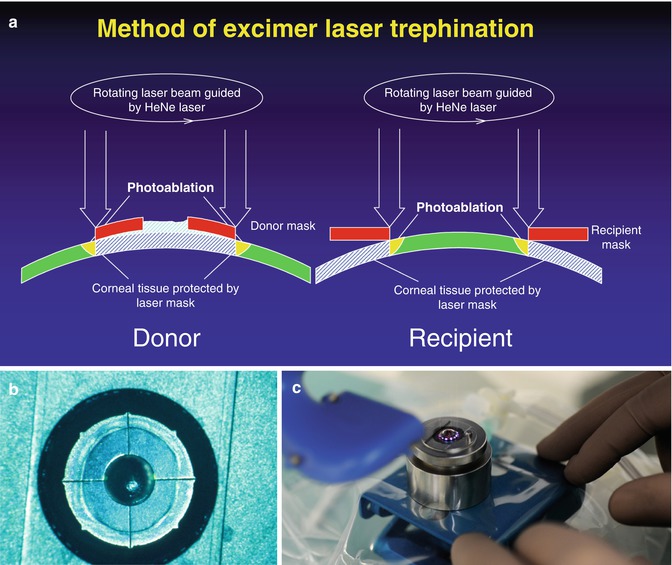
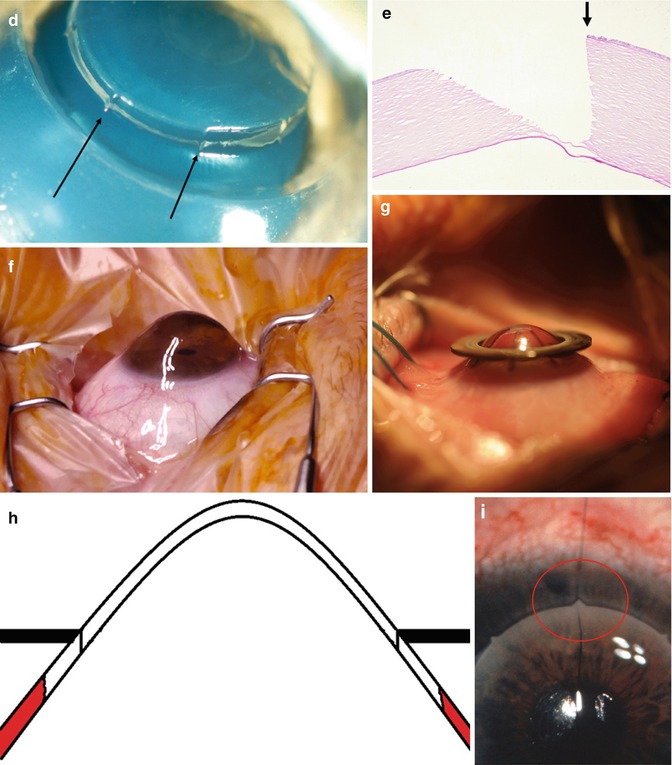
Fig. 6.7
(a) Principle of excimer laser trephination in the donor and recipient (schematic sketch, sagittal view). (b) Donor mask (8.1 mm in diameter) with eight “orientation teeth” on the outside lying directly on the corneoscleral disk in the artificial anterior chamber. The laser is guided along the outer edge. (c) Pseudo-ring-shaped automated Schwind AMARIS excimer laser ablation profile along the outer edge of a donor mask on a corneoscleral disk in an artificial anterior chamber. (d) Donor trephination immediately before penetration with smooth cut edges and orientation teeth (arrows; macroscopy). (e) Histology of straight, almost perpendicular incision edges immediately before donor trephination with the excimer laser. (f) Side view of a very prominent keratoconus immediately before trephination. (g) During host trephination with the excimer laser, the metal recipient mask (8.0 mm in diameter) is well centered around the cone without deformation. The laser is guided along the inner edge of the mask. (h) Schematic sagittal view of the cone protruding through the central hole of the metal recipient mask allowing a trephination without deformation. (i) Exact positioning of the second cardinal suture in penetrating excimer keratoplasty through the use of a small tooth and a corresponding notch to prevent “horizontal torsion” (intraoperatively)
Under the hypothesis that the characteristics of the wound bed are considerably more important for the astigmatism after suture removal and the optical quality of the graft than various suture techniques or methods of subsequent suture adjustments, the technique of nonmechanical corneal trephination has been developed and optimized in Erlangen since 1986 [41]. Originally, the elliptical shape was proposed on the basis of the idea that an elliptical graft could best be fitted to the natural elliptical human cornea, both from the optical and the immunological perspective [28]. Prof. G.K. Lang published details of the first two patients after elliptical keratoplasty in 1990 [29]. A total of 42 elliptical keratoplasties were performed in humans from 1989 to 1991 [75]. Subsequently, this method was abandoned for optical reasons, because the need for simple interrupted sutures to prevent rotation of the graft in the recipient bed and the need for asymmetrical suture tension in these multiple interrupted sutures had ultimately not resulted in improved curvature, neither with nor without sutures [76]. Today, we still use elliptical excimer laser keratoplasty for elliptical ulcers with descemetoceles or penetration for the purposes of keratoplasty à chaud (a typical example of elliptical ulceration would be acanthamoeba keratitis) or pellucid marginal degeneration with eccentric thinning of the cornea at the bottom close to the limbus [27].
Since July 01, 1989, more than 4,000 eyes have been successfully operated in Erlangen and Homburg/Saar with the MEL70 excimer laser made by Zeiss Meditec and, recently, with the AMARIS excimer laser made by Schwind (Fig. 6.7c).
With a share of approximately one third, keratoconus has always been by far the most common indication for PKP with this “non-contact” excimer laser technique.
Technique
Before trephination, the limbus is centered along the vertical helium-neon target beam in the donor and patient in order to ensure a reproducible position to the laser beam and therefore symmetrical cutting angles in the entire circumference.
For donor trephination from the epithelial side, a round open metal mask (diameter 5.6–8.6 mm, central opening 3.0 mm for centering, thickness 0.5 mm, weight 0.2 g, 8 “orientation teeth”) is placed on a corneoscleral disk (16 mm) which is fixed in an artificial anterior chamber under microscopic control (Fig. 6.7b–e). The pressure within the artificial anterior chamber is adjusted to approximately 22 mmHg using Maklakoff tonometer [2].
For recipient trephination which is performed clinically with the manually or automated guided laser beam, a corresponding recipient mask is used (diameter 12.9 mm, central opening 5.5–8.5 mm, 8 “orientation notches”). Before the start of trephination, centering relative to the limbus is achieved through the association of the eight notches in the mask with the eight linear marks of a blue-stained radial keratotomy marker which has been previously applied under microscopic control (Fig. 6.7f–h).
Advantages of Nonmechanical Trephination
The main advantage of this excimer laser cutting method, which is performed from the epithelial side in donor and recipient, is the avoidance of mechanical distortions during trephination (Table 6.3). This results in smooth cut edges which are congruent in both the donor and recipient, so that the “vertical tilt” is reduced [32]. “Orientation teeth” on the edge of the graft [4] and corresponding notches in the edge of the recipient for undoubted symmetrical positioning of the first eight cardinal sutures reduce the “horizontal torsion” (Fig. 6.7i). In this way it is possible to improve the optical quality after transplantation. Furthermore, donor and recipient centration is improved [31, 53]. These beneficial influences on the main intraoperative determinants of astigmatism after keratoplasty (Table 6.2) result in lower keratometric net astigmatism, higher topographic regularity, and improved spectacle-corrected visual acuity after suture removal [50, 51, 74].
Table 6.3
Advantages of nonmechanical trephination with the 193 nm excimer laser along metal masks with “orientation teeth”
1. No trauma to intraocular tissues |
2. Prevention of deformation and compression of the tissue during trephination |
3. Reduction of “horizontal torsion” (“orientation teeth”) |
4. Reduction of “vertical tilt” (almost perfect congruent incision edges) |
5. Improvement of recipient and donor centration |
6. Possibility of “harmonization” of donor and recipient topography |
7. Reduction of anterior chamber inflammation after keratoplasty |
8. Reduction of astigmatism after suture removal |
9. Increase in the regularity of the topography of the cornea |
10. Significantly better spectacle-corrected visual acuity |
11. Feasibility of trephination of an instable cornea (e.g., “open eye,” descemetocele, status post-radial keratotomy, iatrogenic keratectasia after LASIK). Any shape possible (e.g., elliptical) |
In addition to less disruption to the blood-aqueous barrier in the early phase after keratoplasty [26], the laser trephination does not result either in increased cataract formation [5] or higher endothelial cell loss of the graft [56]. In addition, the frequencies of the immunological graft reaction [55] and secondary ocular hypertension were comparable in both techniques [57]. The use of metal masks allows an arbitrary trephination technique [75, 76]. Moreover, the use of the laser allows the trephination of an instable cornea, such as in a perforated corneal ulcers (or descemetoceles) or after radial keratotomy or in iatrogenic keratectasia after laser in situ keratomileusis LASIK [27, 59, 60].
Practical Considerations for the Microsurgeon
The somewhat longer trephination time (around 90 s with the Schwind laser) is largely compensated for by the practical advantages for the microsurgeon during the subsequent course of the surgery [41, 42, 51, 60, 66, 74]:
Injury to intraocular structures is impossible with the laser, as tissue ablation ceases as soon as the aqueous humor fills the trephination canal after focal perforation.
The need to complete the cut using scissors is reduced to a minimum.
The location of the first eight cardinal sutures is unequivocally specified by the eight “orientation teeth/notches.”
Crescent-shaped tissue deficits in the region of the donor-recipient junction (such as in the case of noncircular recipient openings, e.g., in keratoconus) are avoided, so that a latent watertight closure is often achieved after just four cardinal sutures.
During the subsequent suturing procedure, the anterior chamber remains largely stable as a rule.
The final double-continuous suture only has to be tightened to a very slight extent in order to maintain an anterior-step-free wound adjustment and watertight wound closure – even after the removal of the eight cardinal sutures.
For this reason, additional interrupted sutures with an unfavorable effect on the graft topography are needed only very rarely at the end of surgery.
Furthermore, the so-called barrel-top formation at the proximal ends of the sutures, which result in a relative cornea plana and, therefore, delayed optical rehabilitation, is largely avoided.
After removal of the eyelid speculum and the fixation sutures, the use of a Placido disk after intraoperative suture adjustment often provides a round projection image.
Nonmechanical trephination using the 193 nm excimer laser along metal masks has significantly improved the results of penetrating keratoplasty after suture removal. The use of the excimer laser also allows controlled trephination of instable corneas, such as in perforated ulcers or iatrogenic keratectasia after LASIK.
Excimer Laser-Assisted Deep Lamellar Keratoplasty DALK
It is well-known that deep lamellar keratoplasty (DALK) only results in good visual acuity when Descemet’s membrane was exposed intraoperatively [69, 71]. When Descemet’s membrane is perforated, this usually results in a “conversion” to PKP. In order to ensure that the typically young keratoconus patient does not experience any disadvantages as a result of the planned DALK, we prepare the donor and recipient trephination with the excimer laser in a typical manner. However, we do not perforate the patient’s cornea. If the “big bubble” is successfully achieved and we can bare Descemet’s membrane – without perforating – we terminate the operation as DALK. If this does not succeed to our satisfaction, the operation can be completed as excimer laser PKP with all of the advantages described above without any disadvantage for the patient. Primum nil nocere….
Femtosecond Laser Trephination for PKP
The femtosecond laser (FSL) operates at a wavelength of about 1 μm (infrared) and the excimer laser at 193 nm (UV). The cornea is transparent to the FSL. The excimer laser is absorbed by the cornea. The pulse duration of the excimer laser is a few nanoseconds, whereas that of the FSL is a few 100 femtoseconds. The repetition rate of the excimer laser today reaches up to 1000 Hz and in the FSL within the range of several kHertz. The energy density of the excimer laser fluctuates between 150 and 400 mJ/cm2, and that of the FSL between 1 and 10 J/cm2. The pulse size of the excimer laser fluctuates between 0.6 and 6 mm, whereas in the FSL it is a few micrometers. The tissue interaction of the excimer laser is based on direct photoablation, while the tissue interaction of the FSL is plasma mediated.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


