Fig. 5.1
Classification of anterior lamellar keratoplasty
Superficial Anterior Lamellar Keratoplasty
Automated Lamellar Therapeutic Keratoplasty (ALTK)
Purpose and Indication
The purpose of the automated lamellar therapeutic keratoplasty (ALTK) is visual recovery from the corneal disorders that have stromal opacity from superficial to mid-stroma. Good indications are the superficial stromal disorders such as lattice corneal dystrophy, stromal scar after corneal infection, refractive surgery, or trauma [9, 42, 48]. If the depth of the stromal opacities is deeper than 100 μm from the surface, ALTK rather than PTK is indicated.
ALTK is less invasive than the conventional anterior lamellar keratoplasty. The procedure can be sutureless with topical anesthesia. The wound quality by microkeratome [16] or femtosecond laser [5, 51] is less irregular than that by the manual cut, and the femtosecond laser can minimize the disparity of the size between host and graft. The shape of the donor by the microkeratome basically resembles the free-cap flap in LASIK. The thickness profile of the graft is meniscus shaped in the center, and the edge is tapered with an acute angle. Therefore, one needs to pay careful attention to wrinkles and dislocation of the graft. In contrast, the graft made by femtosecond laser has a planar shape in the center, and the edge has a side cut with an obtuse angle. Therefore, less dislocation of the graft and better wound adaptation is expected.
On the other hand, femtosecond-assisted ALTK cannot be performed on eyes with dense corneal opacity. In addition, one should recognize that the shape of the stromal bed would be irregular if ALTK was performed on eyes with an irregular anterior surface.
Preoperative Examination
To evaluate the surgical indication for ALTK, the depth and density of the stromal opacity and the smoothness of the anterior corneal surface are critical. Slit lamp examination and corneal topography are useful for identifying the irregularity of the anterior corneal surface. Also, it will be difficult to use femtosecond laser if the iris under the lesion is invisible with slit lamp examination. The anterior segment OCT is helpful for checking the depth of the stromal opacity and determining the depth of cut. To avoid keratectasia, the stromal bed should be more than 250 μm in ALTK.
Procedure and Postoperative Management
The graft is prepared first using microkeratome or femtosecond laser with the use of the artificial anterior chamber for the corneoscleral donor. The thickness is generally set to 250 μm for microkeratome and 200–280 μm for femtosecond laser with the epithelium off. The graft is removed under the surgical microscope and stored. With the topical anesthesia, the stromal cut is made using microkeratome or femtosecond laser for the recipient. After the removal of the pathological tissue, the donor tissue will be placed on the stromal bed for a waiting period of more than 3 min.
When the interface between host and graft is irregular or there is a disparity in size between the host and graft, several sutures will be placed. Finally, a bandage soft contact lens is put in place to avoid the dislocation of the graft.
Adjunctive surgery might be conducted to enhance the outcome in the femtosecond-assisted ALTK. PTK is sometimes done in order to remove the residual scars or smooth the stromal bed simultaneously or separately [38].
The postoperative treatment is basically similar to LASIK or PTK. After surgery, the contact lens is removed, and epithelial healing is confirmed. The topical steroid and antibiotics are prescribed and tapered.
The main complications associated with ALTK are residual stromal opacity at the stromal bed and irregular astigmatism. Epithelial ingrowth rarely occurs at the interface.
Central SALK
Purpose and Indication
Currently, conventional ALK is being replaced by penetrating keratoplasty (PK) or DALK in most cases. This is because the visual improvement by conventional ALK is suboptimal as a result of the irregular astigmatism or scattering associated with the irregular thickness profile in the lamellar donor and stromal bed in the recipient cornea in addition to the residual opacity at the stromal bed.
However, there are a couple of exceptions in which conventional ALK is still being performed. One is for ocular surface disease, and another is for the tectonic purpose such as corneal perforation or Descemetocele.
For the ocular surface diseases associated with limbal stem cell deficiency (LSCD), PK was considered to be contraindicated because of the high incidence of endothelial rejection. Although DALK can be performed for ocular surface disease, the procedure is usually more difficult than for keratoconus or corneal stromal dystrophy, and there are higher risks of perforation which might require the conversion to PK. To avoid the corneal perforation, central SALK combined with LT or cultured cell sheet is preferred in such cases, especially for allograft transplantation. In addition to improving the transparency of the stroma, SALK is useful for providing the healthy stroma as the base for harvesting the implanted epithelium migrating from the LT [19, 47] or cultured cell sheet [27, 29].
PK has been performed on eyes with corneal perforation and Descemetocele for a long time. As the ocular inflammation and anterior synechia associated with perforation can be a risk factor for the rejection reaction of the endothelium, lamellar grafting has advantages over PK in such conditions. Mini-lamellar graft is preferred for sealing the corneal perforation due to stromal melting associated with rheumatoid arthritis and other autoimmune diseases. This can be done with a cryopreserved donor as the emergency surgery.
Preoperative Examination
It is not easy to observe the condition of the corneal thickness and the anterior chamber with slit lamp examination in patients with severe ocular surface diseases such as Stevens-Johnson syndrome/toxic epidermal necrosis and ocular cicatricial pemphigoid. Anterior segment OCT is useful for evaluating the thickness profile of the cornea for these conditions. More surgical skill will be required if the eye has extreme corneal thinning. Measurement of corneal thickness at the site of partial trephination can be performed preoperatively and/or intraoperatively with OCT and pachymetry to determine the depth of cut.
Procedure
In the central ALK for ocular surface diseases, the partial trephination up to about half depth of the thinnest pachymetric reading at the site followed by the manual dissection of host cornea is performed first using a knife or a spatula. The use of spatulas and lamellar dissectors exclusive to lamellar keratoplasty is recommended. The very fine slit illuminator that can be attached to the operation microscope is commercially available and is very useful during delamination in terms of the prevention of perforation and for maintaining uniform thickness of the stromal bed. The handheld slit lamp can be used instead.
After completing the lamellar dissection of the host cornea, the lamellar donor will be prepared. The donor cornea will be mounted on the artificial anterior chamber and well pressurized. The donor was trephined partially with the same diameter and dissected using spatulas. Then, the donor cornea will be placed and sutured.
After surgery, watch carefully for possible infection at the interface between host and graft, persistent epithelial defect in limbal stem cell deficiency, and stromal rejection in case of vascularized cornea.
Peripheral SALK
Purpose and Indication
Peripheral SALK is considered for the tectonic purpose when there is a perforation or a remarkable stromal thinning at the peripheral cornea. This procedure is performed to increase the ocular integrity by treating or preventing corneal perforation and also by reinforcing the peripheral cornea and inhibiting the protrusion of the thinning area. Terrien marginal corneal degeneration, Mooren ulcer, and marginal ulcer associated with autoimmune diseases are the main indications for the peripheral SALK [6, 30].
Preoperative Examination
It is important for surgeons to evaluate the area of thinning at the peripheral cornea. In addition to the slit lamp examination, anterior segment OCT and Scheimpflug camera are useful for mapping the thickness profile of the cornea. Based on the information, one can determine the shape and size of the graft.
The inflammation of the ocular surface should be checked and reduced as much as possible before surgery. The loss of palisades of Vogt (POV) and delayed fluorescein staining of the corneal surface are important signs indicating limbal stem cell deficiency.
For Mooren ulcer, the lesion of corneal infiltrate and area of inflammation at the conjunctiva should be checked carefully, and Brown’s conjunctival excision and keratoepithelioplasty (KEP) should be considered for the active inflammatory stage with the general and topical use of steroid and immunosuppressant [20, 46].
Procedure
If only localized corneal perforation was found with minimum localized area of corneal thinning, mini-lamellar graft can be considered. However, if the corneal thinning is extended circumferentially for most of the eye, peripheral SALK is indicated. In such cases, the use of the usual round graft does not fit the shape of the corneal thinning, and the host-graft junction may cross the area on the entrance pupil, resulting in irregular corneal astigmatism. Therefore, an annular, sector annular, or crescent-shaped lamellar graft is made. In the extremely advanced cases, total lamellar graft may be used. To create the lamellar graft, the marking of the thinning zone of the host cornea is critical, and in addition a paper pattern may be useful for measuring the area with a caliper.
For the annular or sector annular graft, marking with large and small trephine blades is useful for creating an identical incision at both host and graft. Incision is made manually with a knife on the mark. Then, the stroma inside the incisions is carefully dissected with lamellar spatulas. The donor is mounted at the artificial chamber or sutured to the base for improving handling during the preparation. The same marking is made on the donor, and identical incisions are made followed by the dissection in the same fashion. For advanced cases, free-hand corneoscleral graft may be used.
After aligning the graft on the host, the graft is sutured from the proximal side followed by the suture at the distal side alternately. The deep and short bite is preferred especially at the proximal side. The soft contact lens will be placed for a while to facilitate wound healing and to prevent the persistent epithelial defect. The appropriate use of general and topical steroid and immunosuppressant is critical for inflammatory disorders.
Ectopic SALK
Purpose and Indication
Ectopic SALK is sometimes considered for limbal dermoid, recurrent pterygium, conjunctival defect associated with tube shunt, necrotizing scleritis, or scleromalacia [35, 39]. This is mainly for the tectonic lamellar patching, to prevent the recurrence of the original disease, conjunctival epithelization, and reinforcing the scleral tissue. Although scleral tissue can be used for the condition, corneal tissue has advantages over scleral tissue, such as better epithelization or prevention of the original disease, because of the intact Bowman’s layer and for the cosmetic reason that the graft is close to the peripheral cornea or the lesion extending to the peripheral cornea.
Preoperative Examination
Ocular infection and limbal stem cell deficiency should be ruled out. Diplopia and the limitation of eye movement should be checked carefully for recurrent pterygium. For limbal dermoid during childhood, the prevention of amblyopia is the key for the procedure. Examination and treatment for amblyopia should be conducted not only after surgery but also before surgery.
Procedure
For limbal dermoid, the conjunctiva is removed from the surrounding area of the dermoid. The cautery of feeding vessels is helpful for avoiding bleeding during excision of the tissue. The partial cut with trephine followed by dissection under the dermoid is conducted. The slit illumination during excision is useful for avoiding the corneal perforation. Full-thickness graft can be used in most of cases. If necessary, trimming at the posterior edge of the graft is effective for good adaptation of the wound.
In general, the recurrence of pterygium can be treated with the combination of mitomycin C, amniotic membrane, and conjunctival autograft. However, massive proliferation of the conjunctiva or thinning at the peripheral cornea and/or sclera may require the additional use of a tectonic lamellar patch.
Deep Anterior Lamellar Keratoplasty (DALK)
Purpose and Indication
For a long time, penetrating keratoplasty (PK) had been the gold standard of surgery for loss of vision associated with corneal opacities or severe irregular astigmatism. PK is a straightforward procedure, and the results are generally excellent without the serious general complications that are sometimes inevitable in allogenic transplantation, including the kidney, heart, liver, or other organ transplantations.
However, there are some problems in PK to be solved. Intraoperatively, surgeons have to worry about the risk of suprachoroidal hemorrhage as part of the nature of the open sky procedure. Postoperatively, endothelial rejection and endothelial decompensation can be the main cause of graft failure. Topical steroid that is used for the prevention of rejection reaction might induce glaucoma in steroid responders and also increase the risk of infection and cataract. The ocular integrity following PK is not as good as that in normal eyes, and there is a risk of wound dehiscence associated with trauma or suture removal [18, 22].
In addition, there is a trend toward minimally invasive ophthalmic surgery nowadays. If patients had stromal pathologies of the cornea with healthy corneal endothelium, DALK, which replaces only pathological stroma and preserves the corneal endothelium and Descemet’s membrane, will be less invasive and can be performed as a closed surgery. Because corneal endothelium is auto-tissue in DALK, endothelial rejection and prolonged used of topical steroid can be avoided, and a stronger wound is advantageous for earlier suture removal and less risk of wound dehiscence.
Although the concept of selective lamellar keratoplasty has been considered for a long time, sufficient dissection of stroma in DALK was technically very difficult and time consuming. Lamellar keratoplasty, which is currently termed anterior lamellar keratoplasty (ALK), had been mainly performed not for optical purposes but for tectonic purposes. This is because manual dissection of the stroma has to be conducted for both host and donor in ALK. As the lamellar graft and stromal bed of the host tended to be irregular by the manual dissection, visual recovery following ALK was suboptimal and inferior to that following PK. Therefore, PK has been the primary procedure even for eyes with healthy corneal endothelium.
The advances in surgical microscopes and instruments for stromal dissection made it possible to perform layer-by-layer removal of pathological stroma. In addition, the visualization and handling of the very thin corneal stroma were remarkably improved by the air injection to the stroma [3] or hydration of stroma [40]. With these techniques, surgeons can expose the Descemet’s membrane or reach the pre-Descemetic layer and implant the full-thickness graft. This procedure was previously called deep lamellar keratoplasty (DLK). As DLK also stands for diffuse lamellar keratitis after LASIK, the acronym DALK took the place of DLK.
These layer-by-layer techniques required specific skills on the part of the surgeon and longer surgical time with unique intra- or postoperative complications such as the rupture of Descemet’s membrane and double chamber.
The big bubble technique developed by Anwar made DALK more popular [2]. This is because one can expose the Descemet’s membrane more easily in less time than with layer-by-layer techniques. When the big bubble was not shown, the visibility of corneal stroma was deteriorated, and the layer-by-layer procedure became more difficult. For avoiding perforation with the needle and increasing the probability of big bubble formation, modified techniques such as the use of blunt cannula and lamellar dissection before air injection were devised. As alternative techniques for exposing the Descemet’s membrane, many variations including hooking technique and visco-delamination technique were introduced.
Currently, DALK can be classified into two categories: Descemetic DALK and pre-Descemetic DALK (Fig. 5.2). In pre-Descemetic DALK, the thin stroma layer still remains on the Descemet’s membrane, so its surface is irregular. On the other hand, in Descemetic DALK the Descemet’s membrane or pre-Descemetic layer is exposed, and the surface is shiny and smooth.
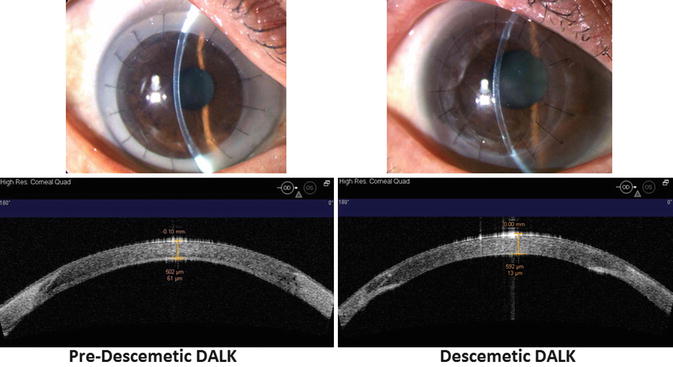
Fig. 5.2
Pre-Descemetic DALK and Descemetic DALK
Indications for optical DALK are irreversible stromal opacity with intact corneal endothelium and Descemet’s membrane. Therefore, keratoconus, stromal corneal dystrophy, necrotizing keratitis in herpetic keratitis, old interstitial keratitis, stromal scar after trauma, or corneal infection are good indications for DALK. Also, keratectasia following LASIK and extremely irregular cornea following radial keratotomy or other refractive surgeries can be indications for DALK. On the other hand, if there is a history of acute hydrops in keratoconic eye or damage to Descemet’s membrane for any reason, there will be a higher chance of rupture in Descemet’s membrane during big bubble technique.
Preoperative Evaluation
As DALK is basically the procedure that replaces the pathological corneal stroma with a healthy one, all the other components, i.e., corneal endothelium, Descemet’s membrane, and corneal epithelium should be determined as being in good condition before surgery.
Endothelial function can be estimated by the combination of slit lamp examination, specular microscope, pachymetry, and OCT. The slit lamp findings such as stromal edema, subepithelial edema, and folds in Descemet’s membrane are signs of endothelial dysfunction. The endothelial cell density at the clear part of the cornea is useful for estimating the corneal endothelial count when the corneal pathology is in an inactive stage. Pachymetry with ultrasound or OCT is useful for quantitating the stromal edema. The cross-sectional images of the cornea with the anterior segment OCT can show us the information at the invisible area with slit lamp because infrared light penetrates more deeply than visible light. The folds in Descemet’s membrane or retro-corneal fibrosis may be identified with OCT in the invisible area with the slit lamp. The observation of Descemet’s membrane with the slit lamp examination and OCT is also very important for excluding its damage due to acute corneal hydrops or perforating corneal injury.
For working out a surgical strategy, confirming the thickness profile of the stroma, especially the location and degree of the thinnest point and the thickness at the site of partial trephination, is helpful.
Similarly to PK, the assessment of cornel epithelium for ruling out limbal stem cell deficiency is critical, and also the evaluation of the condition of the lid, lacrimal function, and function of the nasolacrimal duct is necessary. Glaucoma, ocular infection, and inflammation of the anterior segment should be treated and stabilized before the surgery. Ocular comorbidities including cataract, vitreoretinal diseases, and neuro-ophthalmological disorders should be evaluated.
Procedure
DALK can be performed under local or general anesthesia while soft eye is maintained during surgery. It is important to ready for the conversion to PK in all cases, even if the risk is low. For considering the risk of conversion to PK, the pupil is usually constricted with miotic drug before surgery. Partial thickness trephination is performed on half to two-thirds of the corneal thickness at the area. Then, stromal dissection is started with one of the following techniques.
Big Bubble Technique
The original technique introduced by Anwar uses the fine needle with the bevel side down and inserts the tip of the needle to the deep stroma near the center from the partially trephined area followed by the injection of the air to the stroma [2]. Although the emphysema at the stroma is usually made of fine bubbles, the whitish ring (big bubble) that expands from the site of needle to the periphery can be seen when the tip of the needle is close enough to the posterior corneal surface. This phenomenon is called the formation of big bubble, and it represents the separation of Descemet’s membrane from the stroma inside the whitish ring.
There are two types of big bubble [12]. The Type 1 bubble starts from the center of the cornea and expands to the periphery in a concentric fashion. It usually stops when the diameter reaches about 8.5 mm diameters. The Type 1 bubble has a well-circumscribed central dome shape. The dissection in Type 1 is conserved between the stroma and pre-Descemetic layer [12, 15]. This pre-Descemetic layer is acellular and strong, and its thickness is about 10 μm. The Type 2 bubble is sometimes eccentric, and it starts anywhere and easily expands up to angle. The Type 2 bubble is thin walled and can extend up to 10.5 mm in diameter. The dissection is considered between the pre-Descemetic layer and Descemet’s membrane. The Type 2 bubble is easy to rupture even with the mild touch of blunt instruments.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


