The Optics of Myopia
Wayne G. Whitmore
The optical correction of the myopic eye can present unique and frustrating management problems. An understanding of the optical considerations that govern the visual rehabilitation of these patients is indispensable to their proper management. Myopia is the most common human eye disorder, with an increasing prevalence of about 42% in the United States population1 that varies with age, sex, race, ethnicity, occupation, education, environment, and other factors in various sampled populations.2,3 Myopia can affect up to 80% of young adults in Taiwan4 and Singapore.5 In a general ophthalmology practice setting, myopes represent a larger proportion of patients because of their dependence on visual aids, their desire for refractive surgery, or because of their increased risk for ocular diseases such as cataract, glaucoma, retinal degenerations, and retinal detachment.2
The refractive power of the cornea and crystalline lens, modified slightly by anterior chamber depth (and to a lesser extent by the aqueous and vitreous), determines the refractive power of the eye. In combination with the axial length, these elements determine the refractive state of the eye. Extensive investigations into the range of measurements for these different components of refraction have shown normal distributions for all except axial length. The distribution for axial length shows an excess or kurtosis at approximately 23.5 mm with a skew toward increased axial lengths.6,7 By what appears to be an active process of “emmetropization,” these components tend to develop and correlate so that most eyes become emmetropic. Animal experiments in primates and other vertebrates have shown that normal postnatal eye growth is dependent on form vision (to the retina) and that with normal development and normal visual input, eyes “seek to become emmetropic” giving a distribution curve of refractions with a kurtosis around emmetropia showing a skew toward myopia.8,9 Despite the strong evidence for potentially controllable environmental factors in myopia development, genetic factors clearly play a significant and probably the predominant role as the determinant of the ultimate refractive state of the eye.2,10 Ongoing research may change this in the near future (see last section in this chapter—New Developments in the Treatment of Myopia).
DEFINITION OF MYOPIA
Myopia is defined as that optical condition of the nonaccommodating eye in which parallel rays of light entering the eye are brought to a focus anterior to the retina. It also can be described as the condition in which the far point of focus is located at some finite distance in front of the cornea. For practical purposes, this is a distance of less than 6 meters, the distance at which visual acuity is normally tested. Thus, the uncorrected, nonaccommodating myopic eye has some point at a finite distance beyond which objects are not seen clearly. At this far point, an object is in clear focus, but with increasing distances beyond it, the image becomes progressively more indistinct (Fig. 42-1). This far point also is defined as the focal point of the eye. The degree of myopia in diopters (D) is found by determining the reciprocal of the distance to the far point or focal point of the eye measured in meters. Therefore, P = 1/f where P is the power of the refractive error in diopters and f is the distance of the far point or focal point of the eye in meters from the eye. If the far point of an eye is at 33.3 cm, then the eye is 1/0.333 m = 3.0 D myopic.
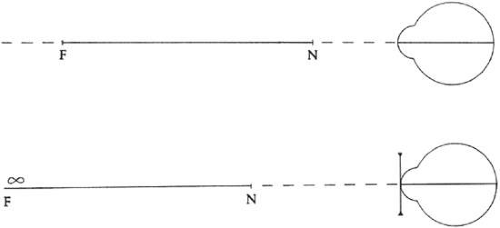 Figure 42-1. Light rays originating at the far point (F) of a -5-D eye focus at the retina. The far point and retinal focal point (f) are said to be conjugate. (Curtin BJ: The Myopias: Basic Science and Clinical Management. Philadelphia: Harper & Row, 1985) |
REFRACTIVE AND AXIAL MYOPIA
Despite there being some overlap, Curtin2 has recommended the classification of myopia as either refractive (“correlation” or “simple”) or axial (intermediate and pathologic) on clinical grounds, with axial myopia showing distinguishing characteristics (such as crescent formation) and having an increased risk of ocular diseases such as glaucoma, cataract, retinal degenerations and retinal detachment. In refractive myopia, the overall refractive power of the eye as determined by cornea and crystalline lens power, modified by anterior chamber depth, is excessive in relation to an eye of “normal” axial length (21.5–25.5 mm). The axial length is normal because it is the product of normal growth and shows no signs of retinal, choroidal, or sclera thinning such as disc crescent formation, tessellation, or staphyloma. Axial myopia, on the other hand, is the result of an excessive elongation or expansion of the posterior segment of the eye with respect to the refractive components of the anterior segment. These myopic refractive state variations can have optical significance. Equal amounts of myopic progression are produced by smaller increases in axial length in refractive myopia compared with axial myopia. For example, in refractive myopia, 0.34 mm of axial length change equals approximately 1 D of refractive error change, whereas in axial myopia, 0.4 mm of axial length change equals approximately 1 D of refractive error change.11 The differences between axial and refractive myopia also affect retinal image size, which is discussed under Image Minification later in the chapter.
THE ANGLE KAPPA
The angle between the visual and pupillary axes of the eye is defined as the angle kappa. The visual axis in emmetropic eyes is normally slightly medial to the pupillary axis. This is defined as a positive angle kappa. In higher grades of myopia, a temporal shift in the visual axis with respect to the pupillary axis is seen, resulting in a negative angle kappa. Patients with a negative angle kappa may have the illusory appearance of esotropia on cursory examination (pseudoesotropia). This temporal shift of the visual axis in high myopia probably relates to an asymmetric expansion of the posterior segment of the globe. These illusory shifts in the visual axis can be distinguished easily from true tropias by cover testing.
THE SPECTACLE CORRECTION OF MYOPIA
The optical correction of myopia with spectacles, particularly the higher degrees, presents several considerations that must be addressed by the practitioner. Higher-power minus lenses cause image minification and “barrel” distortion in addition to prismatic image displacement. These problems are more pronounced in larger diameter lenses. Although these do not present an adjustment problem to myopes accustomed to wearing spectacles, changes in prescription may bring on their unpleasant optical effects. The thick-edged lenses necessary for higher myopic corrections can also present cosmetic problems for some patients. These considerations should be discussed with patients to ease the transition to, and permit a more realistic expectation of their vision with, stronger spectacles.
The minus spectacle lens operates at an optical disadvantage when compared with the same power plus lens at the same vertex distance, and this is increasingly so with higher degrees of refractive error. As can be seen in Table 42-1, a minus lens requires substantially greater power to correct a given refractive error and this is accentuated with greater vertex distances. Image minification also becomes more marked with greater lens powers of myopic correction and with increases in lens vertex distance.
Light rays originating from a point more than 6 meters in front of the eye are considered for practical purposes to be parallel on entering the pupil. At any point closer to the light source, the rays are said to have vergence, which is measured in diopters (D). The vergence of a light ray is equal to the reciprocal of its distance, in meters, from its point of origin. Thus, the vergence of light rays at a given point measured in diopters is inversely proportional to the distance from the focal point of those rays. This focal point may be in front of or behind a given reference point, resulting in divergent (i.e., minus vergence) or convergent (i.e., plus vergence) light rays, respectively. The divergence of light rays 20 cm from an object of regard with a vergence of -5.0 D is 10 times greater than the divergence of light from the same object at 200 cm with a vergence of -0.5 D (Fig. 42-2).
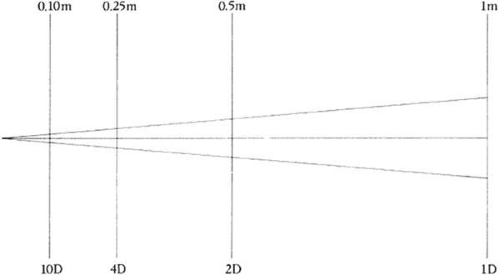 Figure 42-2. The vergence of light rays. At 0.5 m, the divergence power of the light ray is -2 D. (Curtin BJ: The Myopias: Basic Science and Clinical Management. Philadelphia: Harper & Row, 1985) |
A minus lens diverges parallel rays of light. Parallel rays of light entering a -2.0 D lens have a vergence of -2.0 D on leaving the lens, as though the source of the light rays were 50 cm in front of the lens. The optical correction of myopia is accomplished by interposing a minus lens between the cornea and the far (or focal) point of the eye so that the focal point of the lens coincides with the far point (or focal point) of the eye (Fig. 42-3). The closer the minus lens is placed toward the far point, the stronger it must be. Conversely, the closer the minus lens is placed toward the eye, the weaker the lens required to correct the myopia. To minimize optical disadvantages, the minus lens spectacles should be fitted as close to the eyes as possible. The higher the degree of myopia, the greater the optical benefits of a reduced vertex distance (i.e., the distance between the corneal surface and the lens). It is important to reduce vertex distance when refracting patients with moderate to high myopia (greater than 5 D) and to note this measurement on the spectacle prescription.
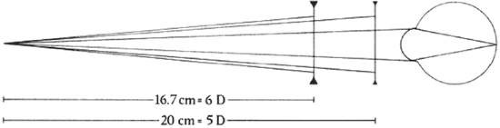 Figure 42-3. The optical correction of myopia is achieved by interposing a minus lens between the cornea and the far point of the eye so that the imaginary focal point of the lens is coincident with the far point. Increased vertex distances require stronger lenses. (Curtin BJ: The Myopias: Basic Science and Clinical Management. Philadelphia: Harper & Row, 1985) |
Minus lens design affects the position of its principal planes, with the back plane (closest to the eye) determining the effective focal length and vertex power of the lens.6 The biconcave lens of equal curvatures has its principal planes between its two surfaces. The meniscus lens, which has one surface convex and the other concave, has its principal planes toward the side of the lens on which the minus power is present. By placing its concave surface toward the eye, the effective vertex distance with the latter type of lens is decreased, which results in less distortion in peripheral vision and when viewing off the optical center of the glasses. Newer lenses of higher refractive index, manufactured in both glass and plastic, can now be made in aspheric single vision and aspheric progressive (multifocal) spectacles. Aspheric lenses for myopic corrections have a thinner edge for improved cosmesis and provide superior optics. When viewing through aspheric spectacles off the optical axis, there is less distortion, improved visual acuity, less chromatic aberration, and, in the case with the aspheric surface on the back of the lenses, an enlarged visual field.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


