(1)
Department of Ophthalmology and Visual Sciences, University of Iowa Hospitals and Clinics, Iowa City, IA, USA
The pioneer worker in the study of the ophthalmic artery, particularly its branches and their variations, was Meyer [1] (in 1887); his observations on 20 cases were accepted more or less as classical, and most accounts of the ophthalmic artery in the textbooks have been essentially based on his study of those 20 specimens, ever since. Apart from occasional reports of various abnormalities, there was no systematic study of the ophthalmic artery until my systematic anatomical studies in human beings [2–4]. I investigated its origin (in 170 specimens [2]), intracranial and intracanalicular course (in 106 specimens [2]), intraorbital course (in 61 specimens [3]), and its branches (in 59 specimens with satisfactory filling of all branches [4]). My studies revealed several discrepancies in Meyer’s [1] description, particularly about the branches, presumably because of his small number of specimens. A Medline search reveals that no further detailed, systematic anatomical study on a large number of specimens has followed mine, so that the following description is essentially based on my findings, with the addition of some later information.
Origin
A detailed description of this is given elsewhere [2]. The ophthalmic artery is the first major branch of the internal carotid artery. It arises soon after the latter has emerged from the cavernous sinus by penetrating the dura (Figs. 1.1, 1.2, 1.3a, 1.4, and 1.5); however, in two specimens, it arose just where the internal carotid pierced the dura, and, in about 7 %, the origin was less than 1 mm above the site of penetration [2]. In about 8 % of the specimens in my study, it arose while the internal carotid artery lay in the cavernous sinus (Figs. 1.3b and 1.6). The ophthalmic artery arises from the internal carotid, usually at its anteromedial or superomedial aspects (Figs. 1.1, 1.2, and 1.4).
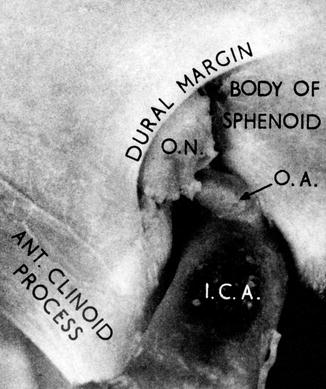
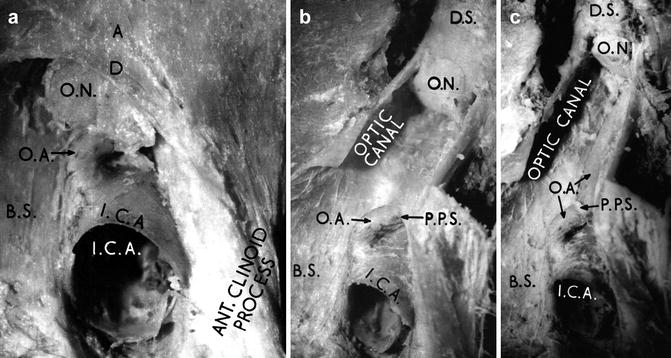
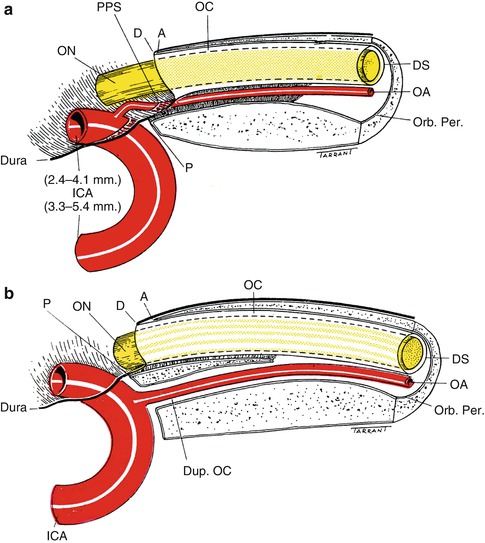
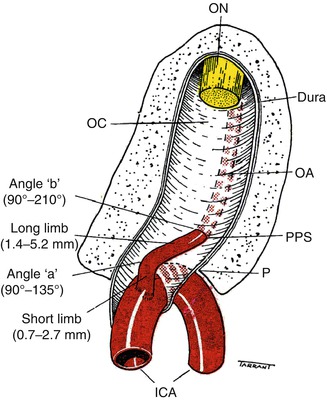
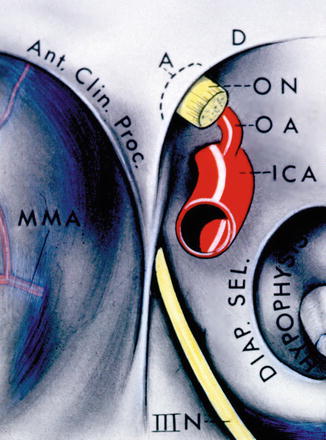
Fig. 1.1
Origin and intracranial part of the ophthalmic artery, with the optic canal intact (Reproduced from Hayreh and Dass [2]). OA Ophthalmic artery, ON optic nerve
Fig. 1.2
All from one specimen: (a) Origin and intracranial part of the right ophthalmic artery, with the optic canal intact. (b) On opening the optic canal, in addition to the above, site of penetration of the ophthalmic artery into the dural sheath is seen. (c) Origin and intracranial and intracanalicular course of the ophthalmic after, as seen on opening the optic canal and removing the covering dural sheath (Reproduced from Hayreh and Dass [2]). A bony intracranial margin of the optic canal, B.S. body of the sphenoid bone, D dura mater, D.S. dural sheath of the optic nerve, I.C.A. internal carotid artery, O.A. ophthalmic artery, O.N. optic nerve, P.P.S. point of penetration of the dural sheath
Fig. 1.3
A diagrammatic representation of lateral views of the optic canal, cavernous and intracranial part of the internal carotid artery, and origin of the ophthalmic artery (Reproduced from Hayreh [5]). (a) Shows details of the usual origin and intracranial and intracanalicular course of the ophthalmic artery. The diameters of the lumen of the internal carotid artery before and after the origin of the ophthalmic artery are shown. (b) Shows an extradural origin of the ophthalmic artery and its course through duplicate optic canal. A bony intracranial margin of optic canal, D dural margin of optic canal mater, DS dural sheath of the optic nerve, Dup. OC duplicate optic canal, ICA internal carotid artery, OA ophthalmic artery, OC optic canal, ON optic nerve, Orb. Per. orbital periosteum, P periosteum, PPS point of penetration of the dural sheath
Fig. 1.4
A diagrammatic representation of the origin and intracranial and intracanalicular course of the ophthalmic artery and its subdivisions, as seen on opening the optic canal (Reproduced from Hayreh [5]). ICA internal carotid artery, OA ophthalmic artery, OC optic canal, ON optic nerve, P periosteum, PPS point of penetration of the dural sheath
Fig. 1.5
A diagrammatic representation of cranial opening of the optic canal with dural margin intact, optic nerve, internal carotid artery, ophthalmic artery, hypophysis, and diaphragma sellae, as seen after removal of the brain. A intracranial margin of bony optic canal, Ant. Clin. Proc. anterior clinoid process, D dural margin of the optic canal mater, Diap. Sel. diaphragma sellae, ICA internal carotid artery, MMA middle meningeal artery, OA ophthalmic artery, ON optic nerve, III N third cranial nerve
Fig. 1.6
Both from one specimen. (a) The extradural origin of the right ophthalmic artery, so that no ophthalmic artery is seen on opening the optic canal; a thinning of the dural sheath is seen at “X,” indicating the position of the artery. (b) The ophthalmic artery is seen after removing the dural sheath covering it (Reproduced from Hayreh and Dass [2]). B.S. body of the sphenoid bone, D.S. dural sheath of the optic nerve, I.C.A. internal carotid artery, O.A. ophthalmic artery, O.N. optic nerve
In 164 of the 170 specimens in my study (Fig. 1.7a), the ophthalmic artery arose from the internal carotid artery. In four of the remaining 6 (Fig. 1.7b–e), although it arose from the internal carotid artery as usual, the main contribution of blood came from the middle meningeal artery through a marked enlargement of the normal anastomosis between the orbital branch of the middle meningeal and the recurrent meningeal branch of the lacrimal artery. In these four specimens, the caliber of the ophthalmic artery between its origin from the internal carotid artery and the point of origin of the lacrimal artery was much reduced. In the remaining two specimens (Fig. 1.7f, g), the arrangement was as above, except that the trunk of origin from the internal carotid artery was either absent (Fig. 1.7f) or obliterated (Fig. 1.7g) in its intracranial and intracanalicular course, so that the middle meningeal artery was the only source of the blood reaching the ophthalmic artery. The two trunks from the internal carotid and the middle meningeal arteries united on the lateral side of the optic nerve in three specimens (Fig. 1.7b, c, g) and on the medial side in the rest (Fig. 1.7d–f). Where the middle meningeal artery supplied all or most of the blood to the orbit (Fig. 1.7b–g), the condition was bilateral in two subjects (Fig. 1.7e, f of one and b, d of another) and unilateral in two (Fig. 1.7c, g). All these four subjects were past middle age. No other abnormal source of origin was seen in my series. Since then, there have been many anecdotal case reports of an ophthalmic artery originating from the middle meningeal, but there is no large study.
Fig. 1.7
A diagrammatic representation of variations in origin and intraorbital course of the ophthalmic artery. (a) Normal pattern. (b–e) The ophthalmic artery arises from the internal carotid artery as usual, but the major contribution comes from the middle meningeal artery. (f, g) The only source of blood supply to the ophthalmic artery is the middle meningeal artery, as the connection with the internal carotid artery is either absent (f) or obliterated (g) (Reproduced from Singh (Hayreh) and Dass [6]). ICA internal carotid artery, Lac. lacrimal artery, MMA middle meningeal artery, OA ophthalmic artery
Site of Origin of the Ophthalmic Artery from the Internal Carotid Artery
I investigated this in 106 specimens [2]. The ophthalmic artery arose from the bend made by the internal carotid artery as it pierced the dura to emerge from the cavernous sinus on the medial side of the anterior clinoid process (Figs. 1.1, 1.2, 1.4, and 1.5). In 95 (90 %), the origin was situated in the subdural space, in eight specimens it was extradural (proximal to the point where the internal carotid artery pierced the dura) (Figs. 1.3b and 1.6), and in one the connection between the ophthalmic and internal carotid arteries had disappeared (Fig. 1.7f). In the other two specimens, the artery arose just where the internal carotid artery pierced the dura: in one the origin lay partly in the subdural space and partly within the dura; in the other the ophthalmic artery carried a thin prolongation of the dura over its subdural course. When the origin was extradural, it was usually close to the point where the internal carotid artery pierced the inner layer of the dura from the cavernous sinus (Fig. 1.3b), but in one specimen it was very deep down in the cavernous sinus.
In 56 specimens, I investigated the origin of the ophthalmic artery from the internal carotid artery. The ophthalmic artery arose from the anteromedial aspect (in 54 %), superomedial aspect (in 37.5 %), medial aspect (in 7 %), or anterosuperior aspect (in 2 %) of the bend of the internal carotid artery. Sometimes the origin and/or initial part of the ophthalmic artery was closely related to the body of the sphenoid (Figs. 1.1, 1.2, and 1.5). The origin of the ophthalmic artery from the internal carotid artery in relation to the cranial opening of the optic canal was located up to 3 mm anterior to the opening in the optic canal (i.e., during the intracanalicular part) in 7 % of the specimens, at the opening of the canal in 5 %, and in 88 % up to 4.8 mm posterior to the opening in the cranial cavity.
Since my study [2], there have been several reports in the literature about the site of origin of the ophthalmic artery from the internal carotid artery. For example, Matsumura et al. [7] in 109 specimens found the origin of the ophthalmic artery to be subdural in 39 % and extradural in the remaining 61 %. Hokama et al. [8] in 50 specimens found it subdural in all but 5 %. Huynh-Le et al. [9], in 70 specimens, found the artery originating from the internal carotid artery within the subdural space in 49 %, and within the cavernous sinus in 6 %. Erdogmus et al. [10] in 38 specimens found the ophthalmic artery arising from the subdural portion of the internal carotid artery, except in 5 % where it originated extradurally. The ophthalmic artery originated from the superomedial wall of the internal carotid artery in 73.7 %, from the central in 21 %, and the lateral in 5.3 % of the specimens. Horiuchi et al. [11], in 119 specimens, found the ophthalmic artery originating from the subdural part of the internal carotid artery in 86 %, extradural in 8 %, and interdural in 7 %. Nishio et al. [12], in 25 adult cadavers, found that in 71 % the ophthalmic artery arose from the superomedial aspect of the internal carotid artery. Thus, the origin of the ophthalmic artery was subdural in 90 % [2] of persons in India, 95 % [10] in Turkey, while 5 studies from Japan reported it in 39 % [7], 49 % [9], 71 % [12], 86 % [11], and 95 % [8]. That wide variation in the Japanese studies is hard to explain.
Keller [13] reported three individuals in whom the internal carotid artery terminated in the ophthalmic artery without giving off any other branch.
Narrowing of the Internal Carotid Artery Beyond the Site of Origin of the Ophthalmic Artery
This has been described by many authors. In ten specimens, Whitnall [14] found the diameters of the internal carotid artery to be 5.4 mm before and 3.8 mm after the origin of the ophthalmic artery, whose diameter was 1.5 mm. According to Sudakevitch [15], the diameter of the internal carotid artery was diminished after the origin of the ophthalmic artery by 2–3 mm, and not more than 4 mm, although in five of 103 specimens, it was 5–8 mm. Fogelholm and Vuolio [16], in 77 cases of internal carotid artery occlusion, found the caliber of the ophthalmic artery in angiograms to be 0–2.5 mm. In my study [2], in 56 specimens the caliber of the internal carotid artery before the site of origin of the ophthalmic artery varied from 3.3 to 5.4 mm and beyond it from 2.4 to 4.1 mm (Fig. 1.3a), the difference varying from nil to 1.3 mm. The artery usually became smaller about 0.5 cm beyond the point where the ophthalmic artery branched off. The lumen of the ophthalmic artery was 0.7–1.4 mm, the same on both sides in 40 %. No correlation was seen between the narrowing of the internal carotid artery and the diameter of the ophthalmic artery. The ophthalmic and internal carotid arteries showed no variation in caliber with age, except in a 4-year-old child, whose internal carotid arteries were smaller than the adults’ (measuring 2.7 and 2.5 mm proximal to the site of origin of the ophthalmic artery, and 2.5 and 2.1 mm distal to it on the right and left sides, respectively). The lumina of the ophthalmic arteries, however, were almost the same as in the adults (0.9 and 1.0 mm). Whitnall [14] suggested two advantages for this narrowing of the internal carotid artery. (1) The ophthalmic artery branches off at right angles from, and at once turns to lie almost parallel with, the internal carotid artery. The mainstream of the internal carotid artery then would tend to suck blood out of the ophthalmic artery rather than force blood into the artery. The narrowing of the internal carotid, however, would tend to dam up the main bloodstream and force the blood back into it. (2) Another reason might be that this reduction in caliber reduces the direct impulse of the arterial pulsation on the brain. Duke-Elder [17] stated that this narrowing of the internal carotid artery would help to ensure an adequately high arterial pressure in the eye. Bock and Schwarz-Karsten [18, 19] also pointed out that the ophthalmic artery, because of its acute angle with the internal carotid artery at its origin, runs against the direction of the blood flow in the internal carotid. They described certain peculiarities in the arterial wall at the site of origin, based on a study of serial sections from eleven subjects of various ages. They demonstrated the presence of “cushions” composed of the smooth muscle and elastic tissue, produced by a thickening of the intima: (1) a spiral cushion like the spiral ridge of a screw at the angle of origin, (2) an ophthalmic cushion running almost vertically in the proximal part of the ophthalmic artery, and (3) a cushion within the internal carotid itself. They were unable to ascribe a definite functional significance to these cushions in the hemodynamics of the artery.
Syntopical Relation of the Origin of the Ophthalmic Artery with the Intracranial Part of the Optic Nerve
This has been variously described. Many [14, 20–29] have shown the site of origin as lateral to the optic nerve in their schematic diagrams, while others described it as medial to the nerve [30, 31], inferior to the nerve [15, 32, 33], under and might be medial to the nerve [34], and inferior to the middle of the nerve [35–37]. Linc and coworkers [38] found it under the nerve in 60 % of cases, medial to the nerve in 27 %, and lateral to the nerve in 13 %. In my study [2], the origin of the ophthalmic artery was inferomedial to the intracranial part of the optic nerve in 43 % of cases, under the center of the nerve in 37 %, inferolateral to the nerve in 16 %, lateral in 2 %, and medial in 2 %.
In one of the specimens in my series [2], there was a hard plaque in the lumen of the internal carotid artery just proximal to the narrowing, and in another, there was an oval area of very thin, more or less transparent, wall distal to the origin of the ophthalmic artery. A similar thinning of the medial wall was seen below the origin of the ophthalmic artery in another specimen; this area was ballooned out so that the lumen of the origin of the ophthalmic artery could be seen through it, and this thinning was closely related to the body of the sphenoid. In yet another specimen, the ophthalmic artery arose at the summit of a small dilatation of the internal carotid artery, and the wall of the latter lateral to the site of origin showed a similar, very thin, circular area. Sclerotic changes, as described above, were not uncommon, particularly in specimens from the older age group.
Caliber of the Ophthalmic Artery
I measured this in 56 specimens. It varied from 0.7 to 1.4 mm [2]. In about 40 % of subjects, the caliber was the same on both sides. The difference in the caliber of the internal carotid artery before and after the origin of the ophthalmic artery was not usually proportional to the caliber of the ophthalmic artery. In only 9 % were the two measurements equal; the narrowing of the internal carotid was greater in 14 % of specimens and less in 77 %. Occasionally, the lumen of the ophthalmic artery was markedly narrowed at its origin from the internal carotid artery.
Lang and Kageyama [39] studied the diameter of the ophthalmic artery in 75 specimens. The diameter 2 mm from the origin was 1.54 ± 0.04 mm (male) and 1.31 ± 0.05 mm (female). The incidence of the ophthalmic artery passing in the orbit medially under the optic nerve was 18.6 %. Erdogmus et al. [10] in a study of the ophthalmic artery in 38 human adult cadavers found the diameter of the ophthalmic artery at its origin 2.25 ± 0.3 mm on the right side and 2.16 ± 0.4 mm on the left.
Abnormal Origins of the Ophthalmic Artery
Abnormal origins of the ophthalmic artery depend on the anastomoses established by the artery with the adjacent vessels (Fig. 1.8). According to Krause’s law [40], “the varieties originate through abnormal development of normal anastomoses.” Meyer [1] confirmed this principle by observation and tried to explain the various abnormalities of the ophthalmic artery on this basis. When the ophthalmic artery does not arise normally from the internal carotid artery (as was the case in 2 of my specimens – Fig. 1.7f, g), or after normal development later becomes obliterated, or the trunk arising from the internal carotid artery is small, then one of the anastomoses with the adjoining arteries has the potential to become the main source of blood supply. That can also happen if the internal carotid artery is absent [41–54] or hypoplastic [55–58]. In every case, the absence was unilateral, except for the case of Fisher [48], who described a bilateral absence. In these patients, the ophthalmic artery arose either from the circle of Willis or from the middle meningeal artery. In Quain’s [53] case, the internal carotid artery was replaced by two branches of the maxillary artery, which entered the skull through the foramen ovale and foramen rotundum. The two branches joined and formed a single vessel that lay on the medial side of the trigeminal nerve. This vessel gave off the ophthalmic artery and other intracranial branches of the internal carotid artery – an arrangement regularly found in ruminants. The common carotid artery was found to be missing by Fife [50] and Boyd [54]. A hypoplasia of the internal carotid artery was seen bilaterally by Hyrtl [55, 56] and on one side by Guinard [57] and Orr [58]. In these cases naturally the origin and even the course of the ophthalmic artery are abnormal, depending on the artery with which the anastomosis is established. Meyer [1], Quain [59], Tikhomirow [60], and I [5] have described the various anastomoses of the ophthalmic artery. Figure 1.8 shows the various anastomoses between the ophthalmic artery and various branches of the external carotid artery. In addition, it may have fine anastomoses with the intracavernous part of the internal carotid artery via the superior orbital fissure (Fig. 1.9).
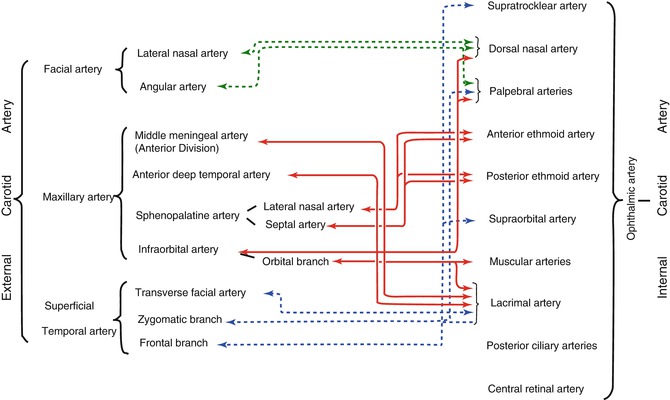
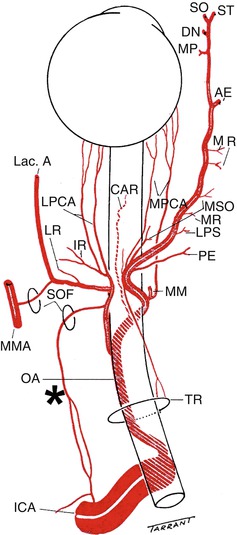
Fig. 1.8
A diagrammatic representation of anastomoses of the ophthalmic artery with various branches of the external carotid artery (Reproduced from Hayreh [5])
Fig. 1.9
A diagrammatic representation of the origin, course, and branches of the ophthalmic artery (OA). Anastomosis in the lateral wall of the cavernous sinus between the proximal part of the cavernous portion of the internal carotid artery (ICA) and a branch from the lacrimal artery passing through the superior orbital fissure (SOF) (Reproduced from Hayreh and Dass [2]). AE anterior ethmoid artery, CAR central artery of the retina, DN dorsal nasal artery, ICA internal carotid artery, IR muscular artery to the inferior rectus, Lac. A. lacrimal artery, LPS muscular artery to the levator palpebral superior, LPCA lateral posterior ciliary artery, LPS muscular artery to the levator palpebrae superioris, LR muscular artery to the lateral rectus, MM medial muscular artery, MMA middle meningeal artery, MP medial palpebral artery, MPCA medial posterior ciliary artery, MR muscular artery to the medial rectus, MSO muscular artery to the superior oblique, OA ophthalmic artery, PE posterior ethmoid artery, SO supraorbital artery, ST supratrochlear artery, TR tendinous ring
The following abnormal modes of origin of the ophthalmic artery have been reported in the literature.
From the Middle Meningeal Artery
This is the most common abnormal origin of the ophthalmic artery reported in the literature [1, 13, 34, 59, 61–78]. When the blood to the bed of the ophthalmic artery is supplied only by the middle meningeal artery, the trunk from the internal carotid artery either disappears or atrophies (Fig. 1.6f, g). Such a supply was seen by Adachi [70] in one of 142 specimens, and by me [2] in two of 170 specimens. Moreover, the literature contains reports of eleven more such cases [14, 34, 63, 68, 72, 76, 78]. Rarely does the central retinal artery arise from the middle meningeal artery. The middle meningeal artery originating from the ophthalmic artery has also been reported in the literature [13, 14, 32, 59, 69, 79–82]. In these cases, the ophthalmic artery contributes frequently to the anterior division of the middle meningeal artery. When the middle meningeal artery arises from the ophthalmic artery, the foramen spinosum is small.
As discussed above, an abnormal origin of the ophthalmic artery from the middle meningeal artery was seen in 6 (in 4 persons) of 170 specimens in my study [2] (Fig. 1.7b–g). This mode of origin is due to the strong development of the normal anastomosis between the recurrent meningeal branch of the lacrimal artery and the orbital branch of the middle meningeal artery passing through the superior orbital fissure or through a foramen in the greater wing of the sphenoid. This anastomosis is normally present during fetal life. The embryonic anastomosis is between the supraorbital branch of the stapedial artery and the ophthalmic artery (see below). Meyer [1] found this anastomosis present in all his twenty cases. It becomes stronger when the ophthalmic artery or its parent trunk is weakly developed or completely obliterated. The trunk that arises from the middle meningeal artery has also been called an accessory ophthalmic artery [76]. Occasionally, the lacrimal artery, instead of arising from the ophthalmic artery, may arise from the middle meningeal artery [1, 4, 14, 27, 29, 34, 59, 62, 65, 70, 76, 83–90]. Rarely, the middle meningeal artery may arise from the ophthalmic artery instead of from the maxillary artery [13, 14, 59, 69, 79–82, 91]. It is very rare for the entire orbit, including the central retinal artery, to be supplied from the middle meningeal artery. The central retinal artery usually preserves its connection with the cerebral circulation by arising from the internal carotid even though other branches in the orbit may arise from other sources, such as the middle meningeal.
An abnormal origin of the ophthalmic artery from the external carotid artery may also be explained by the comparative anatomy of the orbital arteries [7, 71, 92, 90, 93]. In the lower animals, the ophthalmic artery is derived from the external carotid artery, but as we go up the evolutionary ladder of the animal kingdom, the ophthalmic artery tends to arise from the internal carotid instead of the external carotid. In intermediate species, such as the dog, the internal and external ophthalmic arteries arise from the internal and external carotids, respectively, the former supplying the eyeball and the latter the orbit; an anastomotic branch between the two can maintain the intraocular circulation from either source [92, 94, 95]. In rabbits, the internal ophthalmic artery is smaller than the external [78, 95], and the same is the case in horses and goats [96]. According to Sudakevitch [15], the ophthalmic artery in pigs and cows terminates in two powerful posterior ciliary arteries behind the eyeball. The anastomosis between the two systems leads to individual variations in origin. I studied the ophthalmic arteries in rhesus monkeys; although they have a normal ophthalmic artery, a large lacrimal artery connects both the ophthalmic artery and the middle meningeal artery, so that the middle meningeal artery contributes a significant blood supply to the orbit, in addition to the ophthalmic artery [93].
From the Intracavernous Part of the Internal Carotid Artery
Meyer [1] described one case in which the ophthalmic artery developed from anastomoses between fine branches from the internal carotid on one side and the ophthalmic on the other side and then passed through the most medial part of the superior orbital fissure close to the posterior root of the lesser wing of the sphenoid. This was merely an anomalous course, because the ophthalmic artery still arose from the internal carotid. This mode of origin has been reported in five cases [1, 2, 78, 81, 94, 95]. Quain [59] and Wolff [37] also mentioned that the artery might enter the orbit through the superior orbital fissure. One such specimen was seen in my investigation; the ophthalmic artery arose from the internal carotid and entered the orbit through the most medial part of the superior orbital fissure. In another specimen, a branch from the lacrimal artery passed out into the cranial cavity through the superior orbital fissure and clearly anastomosed in the lateral wall of the cavernous sinus with a branch from the internal carotid which had arisen just after the latter had entered the sinus (Fig. 1.9). A similar branch was also seen in another specimen. In such a case, it passed through the superior orbital fissure or duplicate optic canal (Figs. 1.3b and 1.6) [78, 94, 95].
From the Middle Cerebral Artery
This rare occurrence has been reported when the ipsilateral internal carotid artery is missing [47, 49]. In the case cited by Lowrey [49], the right internal carotid was absent, but the left vertebral artery was larger and so also was the right terminal division of the basilar which supplied the middle cerebral artery in addition to the usual distribution.
From the Facial Artery
There is, surprisingly, no reference available for an abnormal origin of the ophthalmic artery from the facial artery through an enlargement of the normal anastomosis between the angular branch of the facial artery and the dorsal nasal branch of the ophthalmic artery. Gillilan [76] noted that this anastomosis, which may or may not occur on both sides, is the most constant. Meyer [1] said that the conditions for the use of this anastomosis were unfavorable because it would mean reversing the direction of the bloodstream in the vessel. Though this anastomosis was invariably present, the ophthalmic artery was never seen to arise from the facial artery in my series.
From the Infraorbital Artery
There is an anastomosis between the orbital branches of the infraorbital branch of the maxillary artery, passing through the inferior orbital fissure or infraorbital groove, and various branches of the ophthalmic artery, particularly the muscular branches, but no instance of the ophthalmic artery arising from the infraorbital artery can be found in the literature. Winslow [100], however, in 1776 wrote as follows: “The same external carotid, by means of the branch called internal maxillary artery, sends into the orbit through the fissure orbitalis inferior or the sphenomaxillaris, a notable branch, which is distributed in the periorbit, the muscles of the eyeball, in the proper retractor of the upper eyelid, in the fat, in the lacrimal gland, in the conjunctival membranes of the eyeball and the eyelids, in the caruncle, etc. It communicates with the internal carotid.” Haller [84] commented on this as follows: “Surely the utterances of Winslow, who had written rather too loosely, that the artery from the spheno-maxillaris, which to us is infra-orbital, is sent to the muscles, and ball of the eye have been misleading to clinical men.” There is no other mention of the ophthalmic artery arising as a branch of the infraorbital artery. Meyer [1] suggested that Winslow probably based his description on one exceptional case. No such mode of origin was seen in my series, though the anastomosis was very frequently present.
From the Anterior Deep Temporal Artery
The anastomosis between the ophthalmic artery and the anterior deep temporal artery through small canals in the zygomatic bone is not usually well developed, and no example is known of the ophthalmic artery arising from this source, although there are a few references in the literature to an abnormal origin of the lacrimal artery from the anterior deep temporal artery [87, 89]. No such case was seen in my series.
Course
This is described in detail elsewhere [2, 3]. The entire course of the ophthalmic artery can be divided into three parts: (a) intracranial [2], (b) intracanalicular [2], and (c) intraorbital [3].
Intracranial Course [2]
This section extends from the point of origin to the opening of the optic canal. In my study, it was investigated in 56 specimens. During this part, the ophthalmic artery is intimately related to the proximal part of the internal carotid artery (Fig. 1.1), to which it frequently adheres for some distance [2]. In seven specimens, the intracranial section was absent; in three of these cases, the ophthalmic artery was extradural, and it had no chance of entering the subdural space (Figs. 1.3b and 1.6). The length of the intracranial section was very variable. The subdural part of the ophthalmic artery is always attached to the under surface of the optic nerve by a loose meshwork of vascular connective tissue. In my study, in about 85 % of the specimens, the whole of the intracranial course lay in the subdural space, in about 10 % partly in the subdural space and partly within the substance of the dural sheath, and in 5 % it was extradural (Figs. 1.3b and 1.6). The relationship of the site of origin with the inferior surface of the optic nerve was not affected by the distance between the point of origin and the optic canal in my series, but it was observed that, when the site of origin was further from the optic canal, it tended to be located below the medial side, and vice versa. The initial part of the ophthalmic artery (which may be entirely or partly intracranial) follows a characteristic course, which I divided into 4 parts – from the origin onward, these are the short limb, angle “a,” long limb, and angle “b” (Fig. 1.4). Those are discussed at length elsewhere [2]. The origin the initial parts of the ophthalmic artery, or both, may be closely related to the sphenoid bone (Figs. 1.1, 1.2, and 1.5). Therefore, the likelihood of involvement of the ophthalmic artery and optic nerve in sphenoidal sinus disease must be kept in mind.
Intracanalicular Course [2]
This section lies in the optic canal, usually inferolateral to the optic nerve (Figs. 1.2b, c, 1.4, 1.6b, and 1.10). In the region of the optic canal, the two layers of the dura mater are fused, but they split up in the cranial cavity to form the cavernous sinus, while in the orbit the inner layer forms the dural sheath of the optic nerve, and the outer layer forms the orbital periosteum. In the cranial cavity, the ophthalmic artery mostly lies in the subdural space, but in the orbit it lies always between the two layers. In the optic canal, the ophthalmic artery usually lies partly in the subdural space (0.3–4.8 mm) and partly within the substance of the dural sheath (Figs. 1.2b, c and 1.4), less often entirely within the dural sheath with no subdural course (Fig. 1.6).
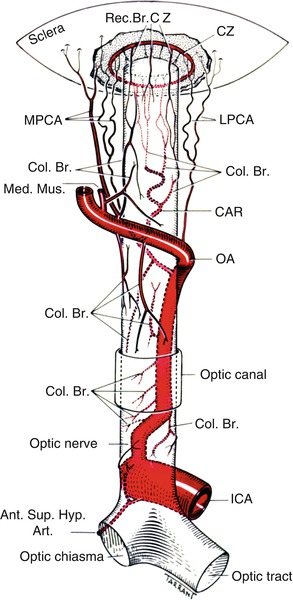
Fig. 1.10
A diagrammatic representation of the origin, course, and branches of the ophthalmic artery (Reproduced from Hayreh SS [100a]). Ant. Sup. Hyp. Art. anterior superior hypophyseal artery, CAR central artery of the retina, Col.Br. collateral branch, CZ circle of Zinn and Haller, ICA internal carotid artery, LPCA lateral posterior ciliary artery, LPS muscular artery to the levator palpebrae, LR muscular artery to the lateral rectus, Med. Mus. medial muscular artery, MPCA medial posterior ciliary artery, OA ophthalmic artery, Rec.Br.CZ recurrent branches of the circle of Zinn and Haller
Haller [84] quoted Cassebohm [101] as having described a special bony canal separate from the optic canal through which the ophthalmic artery might pass. A similar special canal was also described by Dubrueil [63]. Meyer [1] saw no such canal in his series, but Le Double [102] found twelve cases reported in the literature which occurred singly and bilaterally and in either sex. White [103] saw three such cases and found the artery more commonly grooving the posterior part of the floor of the canal. According to Whitnall [14] and Wolff [37], this is a very rare anomaly, and Whitnall [37] called it a “double optic foramen.” In eight specimens in my series, the ophthalmic artery arose extradurally, and in three of them (two in one subject) it traveled from the cranial cavity to the orbit in a special canal separated by a bony lamina from the optic canal (Fig. 1.3b). This special canal was lined by dura; it was thought to have been formed by ossification of the fibrous tissue between the ophthalmic artery and the optic nerve [1, 14, 37]. The ophthalmic artery, instead of passing through the optic canal or this separate canal, may also pass through the superior orbital fissure [1, 14, 37]. This was seen in one of my specimens, where it lay in the most medial part of the superior orbital fissure medial to the oculomotor nerve and then lay against the inferolateral aspect of the nerve and thereafter ran the usual intraorbital course.
When the artery arises in the subdural space, it always pierces the dural sheath of the optic nerve on its inferior aspect (Figs. 1.2 and 1.4). This penetration, as seen in 50 specimens with subdural origin in my study, occurred in the optic canal in 68 %, under the cranial opening of the optic canal in 20 %, and intracranially in 12 %. This site of penetration was under the lateral aspect of the nerve in 72 % and under the center in 28 %. Haller [84] once saw the ophthalmic artery passing over the optic nerve in this part of its course, but this was not seen in my series; nor was it reported by anyone else.
The ophthalmic artery runs within the substance of the dural sheath until it emerges at the apex of the orbit, where it usually lies at the inferolateral aspect of the optic nerve. During its course in the dural sheath, the artery is separated from the surrounding dura by areolar tissue (Figs. 1.2c and 1.6b), except where it proximally pierces the dural sheath (Fig. 1.2b, c). It can be very easily separated from the sheath and picked up from its bed. In my series, the walls of the ophthalmic artery were seen to be very thin during its course within the substance of the dural sheath. It was, in fact, so thin and transparent that the lumen of the artery was usually seen through it, and it was easily torn on handling.
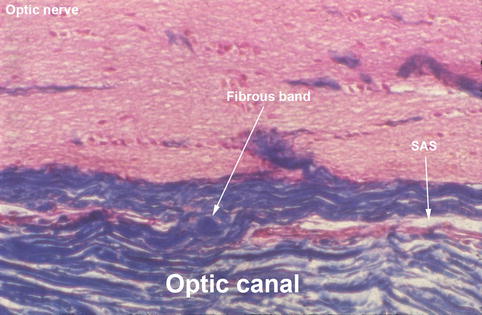
In the optic canal, the optic nerve is attached to the surrounding dura by fibrous bands (Fig. 1.11); through these bands run the fine branches from this part of the ophthalmic artery. In the event of fracture of the canal, if these fibrous bands are torn, the vessels they contain are also torn, resulting in optic nerve ischemic damage.