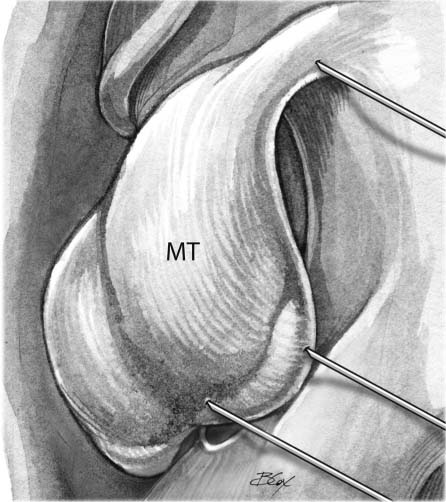
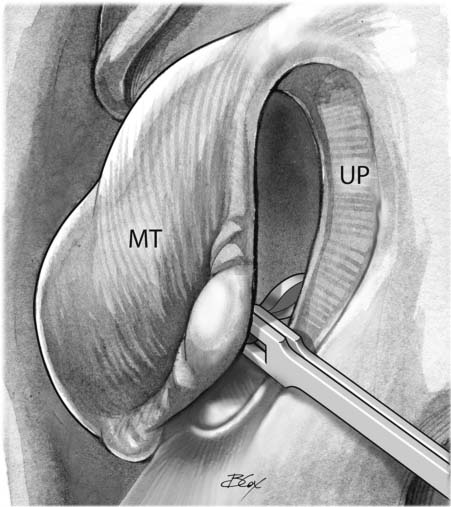
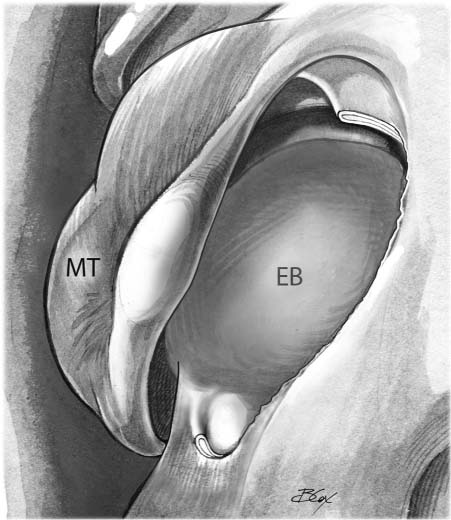
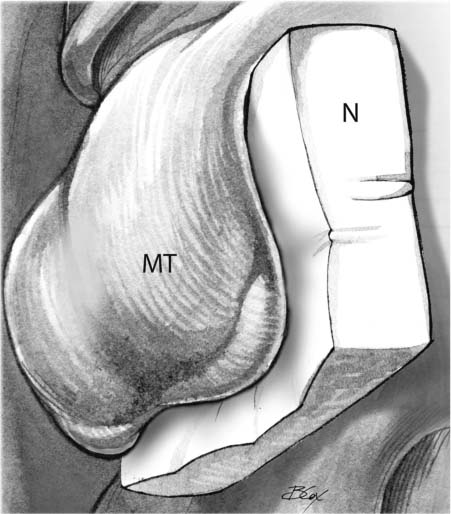
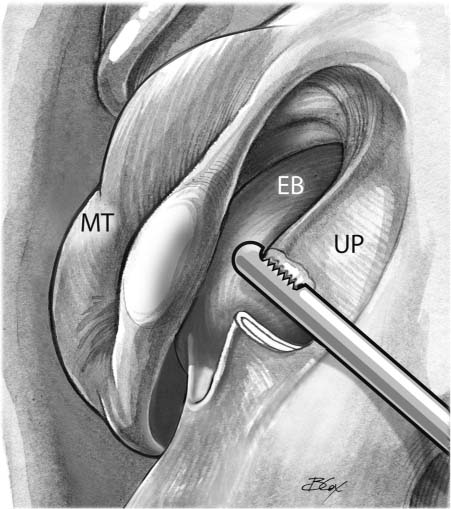
13 The Minimally Invasive Sinus Technique for the Maxillary Sinus Since its introduction in the mid-1980s, functional endoscopic sinus surgery (FESS) has become the standard surgical intervention for patients with chronic sinusitis refractory to medical therapy. Unlike prior sinus procedures such as the Lothrop or Caldwell–Luc, FESS represented a targeted intervention, aimed at restoring normal sinus mucosal physiology. FESS was the first surgical model for the treatment of chronic sinusitis to address the underlying pathophysiologic mechanisms of sinusitis as first described by Messerklinger in 1978.1 Through his endoscopic examination of the nose, Messerklinger made several important discoveries. In his book entitled Endoscopy of the Nose, he describes a pattern of shifting light reflexes seen on the mucosal surface of the sinuses representing mucociliary movement that we now recognize as mucociliary transport or clearance. Using endoscopy in conjunction with time-lapse photography, he examined the direction of mucus movement and found that clearance was directed from the larger sinuses to their respective ostia. He also noted that contact between mucosal surfaces leads to disruption of mucociliary movement thereby causing retention of secretions with subsequent obstruction of the subordinate maxillary, frontal, and anterior ethmoid sinuses. Furthermore, he recognized that contact is most likely to occur in the narrow transition spaces (i.e., ethmoidal infundibulum, hiatus semilunaris superior, and retroagger space/nasofrontal recess). Although contact may be due to several causes, such as inflammation from environmental irritants, allergic rhinitis, viral infection, or anatomic distortions, these factors are most influential to the disruption of sinus physiology and development of sinusitis when they directly affect the aforementioned transition spaces. The theory that transition spaces represent the primary physiologic/anatomic bottleneck for the development of sinusitis is further supported by the high frequency with which both computed tomography (CT) and clinical exam findings demonstrate inflammation limited to the maxillary, frontal, and anterior ethmoid sinuses (the posterior ethmoid and sphenoid sinuses do not drain into transition spaces). Another crucial principle introduced with FESS was that mucosal damage and mucociliary dysfunction is often a reversible process. Prior to Messerklinger, most rhinologists believed that the mucosal damage associated with chronic sinusitis was irreversible; therefore, procedures such as the Caldwell–Luc involved stripping of this “diseased” sinus mucosa. In his clinical experience with more than 2500 patients, Stammberger showed that once the transition spaces are cleared of disease, the larger sinuses usually heal without being touched even if mucosal damage seemed “almost irreversible.”2 Recent studies examining mucociliary clearance have shown that patients with chronic sinusitis have impaired mucociliary movement and that FESS is capable of correcting mucociliary dysfunction in these patients, thus demonstrating the reversibility of disease.3–6 Moreover, others have shown that mechanical damage to nasal mucosal epithelium results in loss of cilia and decreased mucociliary transport.7,8 To create optimal conditions for the reversal of disease to occur, surgical intervention should avoid destruction of cilia and emphasize mucosal preservation. Following the discoveries of mucociliary clearance, the reversibility of mucosal damage in chronic sinusitis, and the role of transition spaces as a nidus for sinusitis, FESS was a logical advancement. The technique, based on conservatism, served as a targeted intervention addressing the narrowed transition spaces and reestablishing drainage through primary birth ostia while avoiding direct manipulation of the larger sinuses themselves. Kennedy demonstrated the favorable long-term results of FESS with 98.4% of 72 patients reporting improvement compared with before surgery over an average 7.8-year follow-up period.9 Although there was a steep initial learning curve, many studies have since highlighted the relative paucity of complications associated with the procedure. In a study of 250 patients undergoing FESS, Levine reported that 8.3% of patients developed minor complications whereas only 0.7% developed major complications.10 In comparison, a study of 670 patients undergoing the Caldwell–Luc procedure, the previous gold standard intervention for chronic maxillary sinusitis, Penttillä reported a 19% rate of major complications as a result of the operation.11 Finally, because FESS is based on a minimally invasive approach compared with conventional sinus surgery, there was less overall postoperative discomfort and shorter hospital stays. Although FESS initially established itself as a less invasive, more targeted, and more effective technique than its predecessors, conventional FESS has evolved beyond this description. Originally, proponents emphasized that FESS provides a conservative and effective surgical intervention, rarely requiring a middle meatal antrostomy or stripping of diseased nasal mucosa. Over time, however, there has been a departure from these conservative principles with a tendency toward more aggressive intervention. As a result, surgeons have excessive freedoms in the nose, and sinus procedures are not standardized. There is no longer a systematic reproducible surgical model called FESS, and the surgical intervention and decision-making varies widely depending on the surgeon. Routine resection of middle turbinates, creation of large maxillary antrostomies, removal of all ethmoid bone, and manipulation of normally functioning sinus ostia are common examples of an aggressive surgical trend that has evolved over time without validation. One would hope and expect that procedures and treatment philosophies would and should be modified over time. However, we should also expect that there be reasonable scientific proof in support of such change. The departure from FESS principles will be discussed at length in a subsequent section. Although endoscopy offered a window for more precise visualization of nasal pathology, advances in other sinus instrumentation lagged. The original instruments used in FESS offered minimal precision, were associated with shear damage to normal mucosal tissue, and caused inadvertent stripping of mucus membranes. Technologic breakthroughs, coupled with a surgical model based on Messerklinger’s principles, led to the next major advance in rhinology—powered instrumentation and MIST. The minimally invasive sinus technique (MIST) is a targeted endoscopic intervention, introduced by Reuben Setliff, M.D., in 1994, with virtually identical goals to those originally reported for FESS. However, unlike conventional FESS, MIST strictly upholds Messerklinger’s functional concepts so that the surgeon performs a very targeted initial intervention. Although sinus ostia are rarely enlarged, MIST is much more than not performing a middle meatal antrostomy. The procedure, as outlined in the following section, is the only stepwise intranasal intervention with a defined beginning and end for all patients regardless of disease severity, thereby standardizing the procedure for surgeons and patients alike. By starting at the most medial aspect of the lateral nasal wall and moving laterally, the surgeon minimizes risk to the lamina papyracea. Furthermore, the procedure still allows for extension into the less involved posterior ethmoid and/or sphenoid cavities while maintaining an anatomic-based progression. This elegant, reproducible technique avoids unnecessary disruption of normal mucosa while restoring mucociliary clearance through the primary birth ostia. Although not specific to MIST, endoscopically guided powered instrumentation was first introduced with this procedure and is now routinely employed. In comparison to the early handheld instruments used in FESS, powered instruments provide through-cutting blades for improved precision and preservation of nondiseased mucosa, a key element to the restoration of normal mucociliary function. In one study, a powered microdebrider termed the hummer (Stryker Corp., Kalamazoo, MI), was shown by Setliff et al to be associated with accelerated healing and reduced synechiae formation.12 Real-time continuous suctioning at the tip of the instrument obviates the need for frequent instrument removal for cleaning, thereby reducing mucosal trauma and decreasing operating time. Continuous real-time suction also improves intraoperative visibility with the potential for reduced operative morbidity. Finally, because MIST markedly reduces nasal trauma, eliminates exposed sinus bone, and decreases blood loss, the healing burden placed on the nose is minimal and the need for uncomfortable nasal packing eliminated. MIST clearly offers several advantages over traditional methods employed in FESS. Although proponents of MIST recognize FESS as an effective surgical option for patients with chronic sinusitis, they question the need for departure from Messerklinger’s functional concepts. MIST is a true embodiment of these principles and improves upon FESS by providing an anatomically based reproducible approach to sinus surgery, invokes powered instrumentation with real-time suctioning, preservation of mucosa and turbinate tissue, leaves the primary birth ostia undisturbed in most patients (see below), and decreases operative morbidity. Turbinate tissue is critical to proper nasal and sinus physiology. Routine resection of the middle turbinate often leads to edema and/or stenosis of the nasofrontal duct, and can produce compensatory glandular hypertrophy of the remaining nasal tissue. Powered shaving (i.e., thinning) of the lateral aspect of the middle turbinate and powered resection of the lateral wall of concha bullosa can each improve middle meatal airflow without incurring the risks associated with turbinate resection. Turbinate surgery should always be coupled with the use of absorbable middle meatal stents to minimize the risk of middle meatal synechia. Creation of a middle meatal antrostomy (MMA) is occasionally required. Absolute indications include the biopsy of an antral mass, to correct maxillary sinus recirculation due to a MMA that is not connected to or involving the primary birth ostium, resection of a maxillary sinus fungal ball or inverted papilloma, and to allow for the application of topical medications or repeated outpatient antral lavage in select cases or end-stage hyperplastic sinusitis. The concern with creation of an MMA is not whether it works, but whether it is necessary as a routine procedure in all patients. There is no study to date that demonstrates the routine need for or the proper size of an MMA. However, in 2004, Albu and Tomescu reported their study in which every surgical candidate with chronic rhinosinusitis (CRS) had an MMA on only one maxillary sinus, but not the other.13 After a 19-month follow-up period, the results showed no difference in the postsurgical control of maxillary sinus symptoms or disease between the two sides. Thus, the potential risks of increased middle meatal scarring, interruption of mucociliary clearance and improper ostial function, development of maxillary recirculation by not including the natural ostia in the MMA, and the likely need for revision maxillary surgery preclude the routine creation of an MMA. In the holding area, patients receive a series of nasal sprays with the aim of causing vasoconstriction, and thus greater operative visibility with decreased bleeding. Two sprays of oxymetazoline (0.05%) solution are administered in each nostril. Three such doses are delivered at 5-minute intervals. Following these three doses of oxymetazoline, a cocaine/epinephrine solution is delivered via an atomizer containing 8 mL cocaine (10%) and 0.16 mL of 1:100,000 epinephrine (diluted 1:50,000). Two sprays of this solution are administered every 5 minutes for the 15 minutes prior to surgery (three doses). Of note, the oxymetazoline sprays must be taken before and not concurrently with the cocaine/epinephrine solution as the former plays a role in limiting the systemic absorption, and potential toxicity of the cocaine solution. General anesthesia is preferentially achieved via a laryngeal mask technique (LMA). Three injections of lidocaine 1% with epinephrine 1:100,000 are given. The first is injected into the anterior and lateral attachment of the middle turbinate to the lateral nasal wall. The subsequent two injections are placed directly into the body of the middle turbinate (Fig. 13.1). If the surgeon plans to operate on the contralateral nasal cavity as well, then preinjection should be avoided because more bleeding may result from a rebound effect of the injections. After the injections, a zero-degree endoscope is introduced and the middle turbinate gently medialized with a Freer elevator. Surgery then progresses anatomically in a step-wise manner, beginning with identification of the uncinate process at the hiatus semilunaris. The transition space located behind the uncinate associated with this landmark is the ethmoidal infundibulum. A pediatric backbiter is used, via a retrograde approach described by Parsons,14 to incise the uncinate process from the hiatus semilunaris toward the nasolacrimal duct (posterior to anterior) (Fig. 13.2). This technique provides an added measure of safety by starting the uncinectomy at the furthest point from the lamina papyracea. The uncinectomy should be inspected to ensure that all three layers of the uncinate have been transected and the lamina papyracea has not been violated. Powered instruments can then be employed to extend the uncinate resection superiorly to uncover the agger nasi cells, as well as anterior and inferior to uncover the primary maxillary sinus ostium (Fig. 13.3). These steps serve to open the transition space of the maxillary sinus, agger nasi cells (anterior ethmoid), and frontal recess (Fig. 13.4). Fig. 13.1 Injections are made in the left lateral nasal wall and middle turbinate (MT). Fig. 13.2 A pediatric backbiter is used to perform a left retrograde uncinectomy. UP, uncinate process; MT, middle turbinate. Fig. 13.3 The uncinectomy is completed superiorly and inferiorly using a microdebrider. EB, ethmoid bulla; UP, uncinate process; MT, middle turbinate. Fig. 13.4 The uncinectomy is complete exposing the maxillary os anterior and inferior in the ethmoidal infundibulum. The ethmoid bulla is also fully uncovered. EB, ethmoid bulla. Fig. 13.5 Nasopore (Stryker Corp., Kalamazoo, MI) is placed as an absorbable middle meatal dressing to help with hemostasis, middle turbinate (MT) position, and reepithelization. If multiple ostia are uncovered or identified in the lateral nasal wall, they are left undisturbed. Recent experience suggests that recirculation is uncommon in such cases as the mucociliary flow is already programmed around the additional ostia. This is in marked distinction to recirculation that occurs due to an MMA that is created in the posterior fontanelle that has no connection to the primary birth ostium. The latter case requires connection of the two ostia to correct the recirculation phenomenon. Once the standard MIST procedure is complete, all patients receive a 1-cm wide by 2-cm long piece of Nasopore (Stryker Corp., Kalamazoo, MI) into the middle meatus15 to prevent synechia (Fig. 13.5). Nasopore is a synthetic polyurethane resorbable sponge-like material that is biologically inert and functions well as a middle meatal spacer to aid in local hemostasis, medialization of the middle turbinate, and the prevention of synechia. No other nasal packing is placed. The nasopharynx, oropharynx, and hypopharynx are suctioned free of blood and debris that might have accumulated. The patient can then be safely reversed from anesthesia. Use of the laryngeal mask airway reduces the risk of coughing and/or bucking and the associated nasal hemorrhage during emergence (see Videos 13.1, 13.2, and 13.3). All patients are prescribed an oral antibiotic for the first 5 days after surgery. Nasal saline irrigations are begun within 24 hours of surgery and maintained for a minimum of 4 weeks. Middle meatal debridement is rarely required postoperatively. Most patients are able to return to work or school in 24 to 48 hours following the procedure regardless of the extent of surgery. Thus, MIST is not minimal surgery; however, it is minimally invasive surgery. There are no diet or activity limitations for most patients. Pain is usually minimal and well controlled with acetaminophen. Antihistamines and nasal steroid sprays are avoided for the first month following surgery to avoid excessive mucosal dryness and reduced ciliary flow. Since its introduction in the literature in 1996,12,14 MIST has grown in popularity worldwide. However, it was not until January 2002 that a formal outcome study was published comparing MIST to FESS.15 This study used the Chronic Sinusitis Survey (CSS) as the quality of life outcome instrument to assess improvement following MIST. The CSS was chosen because it has been proven a reliable, sensitive, and easily administered test to evaluate patient disability from chronic sinusitis. The CSS has also been used in previous outcome reports on FESS, allowing a direct comparison of the two techniques (see Video 13.4). To summarize: outcome from MIST as measured by the CSS medication, CSS symptom, and CSS total subscales either equaled or surpassed those after FESS. Compared with FESS, many more patients after MIST were improved to a level that was better than the normative symptom data for healthy individuals in the general population. The follow-up period for the MIST study was twice as long (23 months compared with 12 months) as the FESS study, yet still demonstrated improvement; and the surgical revision rate following MIST was 5.9% compared with an average of 10% following FESS. Furthermore, the results seen following MIST were consistent across the spectrum of disease severity (using CT grades I through IV), disproving the opinion that the procedure was only effective for minimal disease. These findings strongly support the recommendation that MIST be considered the initial surgical intervention for the treatment of chronic sinusitis. It strongly suggests that an excellent quality of life for chronic sinus sufferers could be achieved with targeted surgical manipulation of the nose and sinuses, it validates Messerklinger’s transition space theory and the reversibility of diseased nasal membranes, and it contradicts the rationale for the routine creation of a middle meatal antrostomy. Another, less formal outcome study on MIST entitled “Minimally Invasive Sinus Surgery in the Geriatric Patient” was published in 2001.16 The study used a geriatric population (ages 65–93) of 100 patients undergoing MIST for chronic sinusitis, to assess whether, due to their age, they had a greater potential for intra- or postoperative complications. Quality of life outcome following surgery was also assessed subjectively 6 months after surgery by the study patients. Eighty-four percent of patients reported feeling significantly better, 10% somewhat better, and 6% unchanged. In comparison, another study of 119 patients with chronic sinusitis reported that 80.2% of patients experienced relief after FESS.10 Interestingly, 8 of 10 patients who reported feeling “somewhat better” after MIST, and two of six patients who experienced no improvement, had previously undergone aggressive FESS elsewhere. This supports the opinion that aggressive FESS may have “irreversible adverse effects on nasal and sinus function.” The study also assessed whether there was any exacerbation of preexisting medical conditions, or an increase in surgical morbidity after MIST. The 100 patients presented a spectrum of preexisting medical conditions including hypertension, coronary disease, gastrointestinal disorders, diabetes, bronchitis and asthma, thyroid disorders, gout, stroke, renal disease, prostate disease, dysrhythmias, and others. Early medical complications (within 96 hours of surgery) following MIST included 12 patients with headache, 6 with postoperative sinusitis, 4 had nausea and vomiting, 3 had fatigue, and 1 each with ataxia, hyposmia, syncope, incontinence, and hypoxia. The ataxia and syncope were self-limited and appropriate evaluation was obtained. The nausea, vomiting, incontinence, and hypoxia all occurred in the recovery area following surgery and were self-limited. In addition to verifying the efficacy of MIST for the treatment of chronic sinusitis, the results highlight the fact that minimal medical/surgical morbidity is experienced by geriatric patients following MIST, making the procedure equally safe for the oldest and potentially most frail portion of the population. The findings of these studies are significant because they introduce several new concepts: • Due to a combination of minimally invasive mucosal-sparing surgery, and biocompatible, biodegradable middle meatal stents, synechia following MIST are rare.17 • Because MIST does not manipulate the primary maxillary sinus ostium, the latter remains in the oblique or horizontal plane making it less likely to be obstructed by a lateralized middle turbinate, whereas the final position of an MMA is in the parasagittal plane, making it much more vulnerable to obstruction by a lateralized middle turbinate. • Outcomes data has shown clinical equivalence, if not superiority, from MIST when compared with conventional FESS, thus excellent outcomes across the spectrum of disease can be achieved with less invasive surgery, and for the maxillary sinus, this means no antrostomy. The results of these peer-reviewed articles validate MIST as an effective surgical treatment option for chronic sinusitis. We advocate that MIST should be considered as the initial procedure for patients undergoing ESS for chronic sinus disease. This would minimize the number of patients who receive more surgery (i.e., an MMA) than is required. In our experience,15 the overall MIST revision rate is 6%, thus 94% of patients had appropriate surgery, with only 6% needing additional intervention, and this rarely included the need to perform an MMA. As in other medical fields, sinus surgery has evolved from open to less invasive surgical techniques. As recently as the 1970s, sinus surgery required external facial incisions and resulted in extensive removal of tissue and mucosa. It was hypothesized that diseased mucosa was the primary cause of the condition and should be removed. With the advent of first FESS, and then MIST, treatment of chronic sinusitis took an evolutionary leap forward. These procedures pioneered the use of endoscopes and powered surgical instruments allowing sinus surgery to be performed through the nostrils. One of the goals of FESS and MIST is to uncover the primary sinus ostia to improve sinus ventilation and drainage while preserving the natural birth membrane sinuses and their ostia. During contemporary FESS, the sinus ostia are enlarged with metal surgical instruments, which pose a risk to the mucosal cilia lining the sinus ostia. During MIST, the ostia are uncovered or exposed by marsupializing the transition space to a given sinus, but the ostia remain untouched. Enter sinuplasty, a new technology based on balloon catheter dilatation of the sinus transition space and its ostia with the ability to preserve birth membranes. To gain initial sinus access, the preshaped sinus guide catheter is introduced to the exit of the transition space of the target sinus under endoscopic visualization. A flexible sinus guide wire is introduced through the sinus guide catheter and gently advanced into the target sinus under fluoroscopic guidance. The sinus balloon catheter tracks smoothly over the guide wire and is positioned across the blocked ostium. Using fluoroscopy, or using sinus transillumination with a lighted guide wire, the position of the sinus balloon catheter is confirmed. It is gradually inflated to between 8 and 10 atmospheres of pressure to gently restructure and enlarge the blocked ostium. The balloon diameters range from 3.5 to 7 mm. The balloon is then deflated and removed, having enlarged the transition space and ostium to allow the return of normal sinus drainage and function. There is little to no disruption to the mucosal lining. This technology has been first evaluated in eight human cadavers revealing micro fractures of the bony framework of the sinus ostium, with no visible damage to the skull base or corresponding neurovascular anatomy. In a subsequent study of 125 patients (the CLEAR study), the technology was again shown to be safe with 90% of the treated ostia remaining patent at 6-month follow-up, with longer-term follow-up providing consistent results at 1 and 2 years postsurgery. Personal experience to date in 500 patients has demonstrated safety and similar effectiveness. • Always evaluate the preoperative CT for Haller cells, location and position of the uncinate process, size of the infundibular space, secondary ostia, osteoneogenesis, and bone erosion. • Always enter the infundibulum from the most inferior aspect of the hiatus semilunaris, what is called the “common final outflow pathway.” Note this entry point is usually lower than the position of the maxillary os itself, and so the path of your uncinectomy should be angled slightly superior as you move from posterior to anterior along the uncinate process with your backbiter. • Always follow your uncinate process as far anterior as you can to expose the maxillary os, which is usually located anterior and lateral along the floor of the infundibulum. However, be cautious not to extend your uncinectomy anterior to the anterior tip of the middle turbinate, or past the breakpoint on the lateral nasal wall to avoid orbital entry via the lamina. On occasion, the origin of the uncinate process is anterior to the origin of the middle turbinate; however, this is rare and is best addressed carefully with use of a 30-degree telescope to help assess this possibility. • If multiple natural ostia are encountered, leave them alone! The only time recirculation is clinically significant is when it occurs after a man-made antrostomy in the posterior fontanelle and is not connected to the primary os. Naturally occurring secondary os are not problematic as the ciliary flow has already been established around these openings, thus avoiding recirculation. • Remove as much uncinate process as possible, including superiorly to uncover the agger nasi cell. Inferiorly, you should be able to visualize the maxillary os with a zero- or 30- degree endoscope in all cases. Use of a short ball-tipped probe/seeker can be useful if the mucosa is polypoid and the os not immediately visible. Gentle probing of the os is acceptable with the seeker; however, routine use of a curved suction as a seeker with probing of the os is usually not advisable. If the os seems stenotic (which is rare), a balloon catheter can be used to dilate it to 5 mm. • Allow polypoid tissue to recover as reversibility is common in this area once the uncinate is removed and the physiologic and anatomic “bottleneck” is corrected. • Begin twice daily nasal saline irrigations the day after surgery and continue for 1 month. Nasal debridements are unnecessary in >98% of patients.
 The Philosophy of the Minimally Invasive Sinus Technique
The Philosophy of the Minimally Invasive Sinus Technique
 MIST: The Surgical Model
MIST: The Surgical Model
Preoperative Preparation
Intraoperative Procedure
Postoperative Care
 Outcome Studies
Outcome Studies
 Adjunctive Technologies—Sinuplasty
Adjunctive Technologies—Sinuplasty
The Minimally Invasive Sinus Technique for the Maxillary Sinus
Pearls
< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


