Chapter 22 The management of orbital disease in children
The relative frequency of the conditions causing proptosis in childhood varies considerably 1–8 depending, in part, on the source of the material. Series from eye hospitals3 are different from those from neurosurgical2 or pediatric units.6 Geographic factors vary: the major causes of proptosis in African children4 are different from those seen in Europe and North America. Series that rely solely on tissues specimens1,5,7,8 reflect the incidence of lesions that are excised surgically and exclude the many conditions that can be diagnosed and treated without biopsy or surgery, such as infantile periocular hemangioma, or those in which biopsy may be more conveniently obtained at another site of involvement, such as neuroblastoma or histiocytosis. In that sense, they are not helpful in formulating the differential diagnosis of an individual child with proptosis.
Orbital disease and age
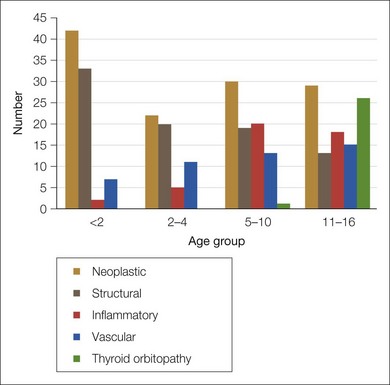
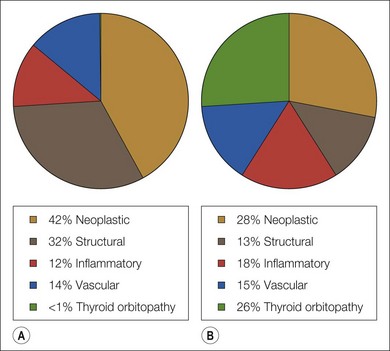
We have reviewed the clinical data of 326 children seen by the orbital service in Vancouver, Canada since 1976 (Table 22.1). This period includes the introduction of the computed tomography (CT) scan, a watershed in the non-invasive investigation of orbital disease. Neoplasia and structural abnormalities (including cysts) account for the great majority of children presenting with orbital disease (Fig. 22.1). This is quite different from adults, in which over 60% of presentations are due to inflammatory causes: structural abnormalities account for less than 15% of cases. However, the distribution of orbital disease in children aged over 11 years is similar to the adult pattern (Fig. 22.2).

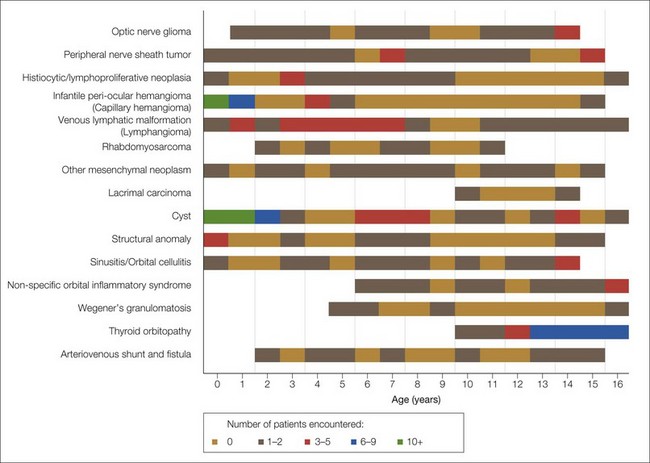
Fortunately, only a small proportion of the neoplasia can be considered malignant, which concurs with published series.6,7,9 Under 2 years of age, the major causes of proptosis are infantile hemangiomas and venous lymphatic malformations (lymphangioma), inclusion and dermoid cysts, and other structural abnormalities. Figure 22.3, which shows the distribution of the major diagnostic groups by age at presentation, indicates that while some lesions are distributed evenly throughout childhood (venous lymphatic malformation, varices, and arteriovenous malformations), others tend to occur within a specific age range. Seven patients with rhabdomyosarcoma were seen, whose ages ranged from 2 to 11 years. The seven patients with Langerhans cell histiocytosis ranged in age from 3 to 9 years. Infantile hemangioma was overwhelmingly more common in early infancy. Inflammatory conditions were increasingly frequent after the age of 5 years, especially orbital cellulitis, non-specific orbital inflammatory syndromes (6 years and over), and thyroid orbitopathy (11 years and over). It is noteworthy that there were two cases of lacrimal gland carcinoma and four of Wegener’s granulomatosis in this series, a reminder that, although rare, these potentially lethal conditions do occur in children.