There are three types of aging cataracts: nuclear, cortical, and posterior subcapsular. Nuclear cataract, the most common type, is a central lens opacification where the nucleus loses its transparency, changing from clear to yellow and sometimes brown. This phenomenon occurs due to deamidation of lens proteins through oxidation, proteolysis, and glycation, which accumulates into high molecular-weight particles that scatter incoming light. Cortical cataract, the second most common type is associated with liquefaction of lens fibers due to electrolyte imbalance, overhydration, and excess carbohydrate intake. Finally, posterior subcapsular cataract, the third and the least common type, is typically formed by the death of lens fiber nuclei and epithelial cells clustering at the lens posterior pole. Cataract development has been attributed to metabolic dysglycemia, retinal diseases, alcoholism, drugs, malnutrition, and smoking [5]. Most common symptoms of cataract include: cloudy or blurry vision, poor night vision, dimmed color perception, perceived glare and halos from headlights, lamps, or sunlight [7] (see Table 10.2 and Fig. 10.1).
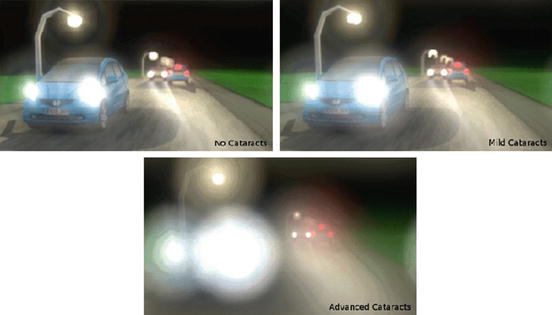
Table 10.2
Biochemistry of ARC (Age Related Cataract)
Damage to crystalline proteins/proteinases with aging in older lenses |
|---|
Oxidation |
Glycation (nonenzymatic glycosylation) |
Glyco-oxidation (oxidation of glycated proteins) |
Addition of lipids |
Cleavage/deamidation/racemization |
Accumulation of ubiquitinated proteins |
Inactivation of proteinases |
Aggregation of lens crystallins (cytotoxicity) |
Tissue dehydration/precipitation |
Fig. 10.1
Simulation of a cataract-affected view and its progression over time. Reprinted from [65] with permission from the Association of Computing Machinery, Inc.
10.2 Sunlight Protection
Sunlight consists of electromagnetic radiation, from infrared to visible light to ultraviolet. Eyes are protected by eyelid and facial structures such as eyebrows, cheekbones, and the nose. Yet eyes are still prone to high-energy ultraviolet (UV) radiation referred to as UVA, UVB, and UVC. UVB is blocked by the cornea and UVC, the most energetic with the shortest wavelength, is almost completely blocked by the ozone layer, UVA has the longest wavelength in the UV spectrum and penetrates deep within the skin and eye. Traversing the cornea, it can induce DNA damage of the anterior lens epithelial cells. Unprotected, exposure to such radiation damages the lens at all ages with infants and young children being particularly vulnerable. UVA damages human DNA indirectly by generating highly reactive chemical intermediates, such as hydroxyl and oxygen radicals [9].
Ecological studies suggest that cataract is more prevalent in countries with more sunlight exposure than in those with less sunlight exposure [10]. There are a higher number of cataract cases reported in countries like Israel and India compared with England [11]. An ecological study called the Beaver Dam Eye Study confirmed the association between UVB radiation exposure and cataracts in men only [12]. Another epidemiological study done by H. R. Taylor showed a significant association for cortical cataracts and UV radiation index. In this study, 838 watermen working on the Chesapeake Bay were surveyed. Taylor’s UV radiation index was based upon number of outdoor hours worked, work location, and attenuation due to spectacle use and hat cover. The study found an association between cortical cataracts and higher UV exposure and suggested that children require more protection against sunlight, specifically UV radiation since they generally spend more time outdoors than adults [13].
10.3 Caloric Restriction
Lifestyle is an important factor in ARC. Many studies evaluated caloric restriction and its benefit(s) to human health. Caloric and dietary restriction is defined as a nutritious diet with 40 % fewer calories compared with an ad libitum diet [14]. Dietary caloric restriction has been shown to delay cataractogenesis. Wang et al. concluded that caloric restriction slowed protein insolubilization and blunted the decline of the total soluble thiols, protein thiols, reduced glutathione, and ascorbic acid levels in the lenses of old Brown Norway rats. In terms of lens protein aggregation, this study described cataract development in three stages: (1) the precipitation of gamma-crystallin, (2) the insolubilization of beta-crystallin, and (3) the final precipitation of alpha-crystallin which was saturated with other denatured lens proteins. A major risk factor in pathogenesis of human cataract is oxidative stress. Caloric restriction is ostensibly beneficial in retarding oxidative stress in the human lens via up-regulation of endogenous antioxidant pathways [15].
10.3.1 Diabetes Mellitus
Chiu et al. explored the association of carbohydrate intake and glycemic index in early cortical and nuclear lens opacity formation. Some 417 female subjects of 53–73 years of age from the Boston’s Nurses’ Health Study provided dietary information via 5 semi-quantitative food frequency questionnaires over a 14-year period. Lens opacities were evaluated using the Lens Opacity Classification System III (LOCS III). The authors concluded that there was a positive association between early cortical lens opacities and the quantity (but not the quality) of carbohydrate intake in middle-aged women. They did not find any significant association between quantity or quality of dietary carbohydrate intake and nuclear lens opacities in middle-aged women [16].
Significantly, cataract is up to five times more prevalent among patients suffering from diabetes mellitus (DM). Diabetics develop all three subtypes (cortical, posterior subcapsular, and nuclear). Risk factors are duration of diabetes and quality of glycemic control. Early insulin treatment has been shown to delay cataractogenesis in patients with both type 1 and type 2 diabetes.
DM is associated with several other diseases, such as heart and vascular complications, neuropathy, retinopathy and dyslipidemia. Hyperglycemia leads to a number of pathogenic mechanisms, including but not limited to increased aldose reductase (AR) activity, nonenzymatic glycation/glycooxidation, activation of protein kinase C, oxidative–nitrosative stress, and poly (ADP-ribose) polymerase (PARP) activation. The lens, in comparison to other tissues of the human body, is avascular and therefore dependent on anaerobic glucose metabolism pathways, such as glycolysis and the pentose phosphate pathway. The lens receives nutrients and oxygen through the blood-aqueous barrier as it takes up glucose in an insulin-independent pathway. In diabetic patients, excess blood glucose enters the sorbitol pathway, in which AR catalyzes NADPH-dependent reduction of glucose to sorbitol, and sorbitol dehydrogenase (SDH) catalyzes NAD-dependent oxidation of sorbitol to fructose. By increasing sorbitol pathway activity, intracellular sorbitol accumulates and results in osmotic stress. Increased AR activity contributes to oxidative–nitrosative stress, nonenzymatic glycation/glycoxidation, mitogen-activated protein kinase (MAPK) and cyclooxygenase-2 activation, accumulation of cytosolic Ca2+, activation of NF-kappaB, and activator protein-1.
Although many mechanisms of diabetic cataractogenesis have been identified, there are no specific methods for prevention or management of diabetic cataracts apart from glucose control. Lifestyle changes, such as carbohydrate restriction, medication, smoking cessation, systemic and intraocular blood pressure management and nutrient supplementation, are all beneficial [17].
10.4 Plant Food: A Source of Nourishing Antioxidants and Cofactor Minerals/Vitamins
Diet-associated ARC is a crucial topic. Plant food containing antioxidants and cofactors fighting against free radicals that cause oxidative stress, are important to stay healthy and mitigate age-related processes. Exogenous and gene derived endogenous antioxidants protect the human body against aging and oxidative free radical assault. Free radicals, antioxidants and cofactors are the main focus of many human aging and supplementation studies. Due to new technologies and improvements in medicine, human life expectancy is increasing at a fast pace. This will not only raise the overall population, there will also be a larger older population in need of health and medical care. Therefore, having a balanced lifestyle in addition to a healthy diet with adequate nutrition is required for all of us.
Free radicals are paramagnetic molecules with unstable chemical configurations. Most free radicals are formed as a byproduct of carbohydrate, protein, and lipid metabolism. For example, Oxygen-free radicals (e.g., hydroxyl super-oxide) along with hydrogen peroxide are known as reactive oxygen species (ROS). Free radicals of oxygen and nitrogen – NOS are extremely and NOS reactive and react with macromolecules and nucleic acids. The amount of ROS being produced in the human body increases with age. This phenomenon in part explains age-associated increase in inflammation and myriad diseases such as neurodegenerative, cardiovascular, cataracts, DM, and cancer.
Antioxidants are any endogenous or exogenous molecules capable of stabilizing free radicals before they cause cellular damage. This protective system, particularly with endogenous antioxidants, decreases in power as humans age. Therefore, there is a greater need for the aged population to monitor their diet or take supplements of exogenous antioxidants. The most effective enzymatic antioxidants are glutathione peroxidase, catalase, and superoxide dismutase. Nonenzymatic antioxidants include vitamins E and C, thiol antioxidants (glutathione, thioredoxin, and lipoic acid), melatonin, carotenoids, and natural flavonoids.
Cofactors are molecules or ions that bind to the catalytic site of enzymes, accelerating biological reactions. Many antioxidant enzymes require metal and nonmetal cofactors such as copper (Cu), iron (Fe), selenium (Se), zinc (Zn), and vitamins B1 (thiamine), and B2 (riboflavin). Cofactors are essential for antioxidant functions, assisting in protection against oxidative damage by free radicals. Cofactor deficiency as well as unregulated and toxic levels of divalent metals can cause health complications, including cataract. Optimal cofactor intake is required for each individual to maintain optimal health.
Copper is a vital cofactor in many critical cellular reactions, including those involving cytochrome C oxidase and zinc-superoxide dismutase. Iron is an essential component of catalase enzymes for hemoglobin and myoglobin. As well as copper, excess iron and copper also has oxidative qualities, which, in contact with lipids, could cause oxidative stress. It has been reported that patients with high levels of iron and lipids are at higher risk of developing cancer. Selenium is another essential cofactor in multiform of glutathione peroxidases, which have been found to protect DNA and cellular oxidative damage. Selenium deficiency has been linked to DNA damage, neurodegenerative disease, cardiovascular diseases, cancer, and cataract. Zinc is another cofactor essential for antioxidant protection against vascular and immunological damage. Zinc has also been found to protect DNA and decrease the risk of cancer. It has also been shown to have a protective function for having a healthy skin, which is important in healthy aging. Copper and zinc are critical cofactors in bone matrix ingredients and synthesis, and the lack of these cofactors has been shown to be correlated with elderly osteoporosis and bone density loss. Vitamins such as thiamine (vitamin B1) and riboflavin (vitamin B2) are also considered as cofactors protecting against oxidative stress. The active form of vitamin B1, thiamine diphosphate, is used in important enzymes of oxidant stress defense. Vitamin B1 deficiency has been linked to neurodegenerative diseases and high levels of oxidative damage. The active form of vitamin B2, flavin dinucleotide, works as a co-enzyme for glutathione reductase and many other antioxidant enzymatic reactions. Evidence shows that vitamin B2 deficiency has been linked to cardiovascular complications and increased risk of developing cancer [18].
In terms of ocular tissue, Bruce H. Grahn et al. investigated the association between zinc and the eye. The authors found a significant concentration of zinc in the eye of most animal species, particularly the retina, retinal pigment epithelium, and choroid. Zinc has several known functions in the retina and retinal pigmented epithelium, such as altering synaptic transmission, regulating the rhodopsin reaction, modulating interactions between taurine and vitamin A, modifying photoreceptor plasma membranes, and acting as an antioxidant. Zinc deficiency can manifest in ocular complications such as altered vision, electroretinograms, oscillatory potentials, and, in severe cases, ultra-structural changes in the retina and retinal pigmented epithelium. The progression of degenerative retinal diseases are reduced by zinc supplements [19].
In another article, Cataracts as an outcome of zinc deficiency in salmon, the authors investigated zinc deficiency-related complications due to high intake of calcium, phosphorus, and phytate. This article concluded that a secondary deficiency of zinc has been associated with a high incidence of cataract in young salmon [20].
David L. Watts has explored the significance of deficiency and toxic levels of selenium in human and animal diets. The review paper, the Nutritional Relationships of Selenium, stated that selenium level constantly increased in the human lens from birth to old age. However, it also stated that lenses suffering from cataracts had sixfold less selenium content compared to that in healthy lenses in the same age group. It found that remarkably low selenium levels in the lens increased oxidative damage due to free radical species [21].
Endogenous antioxidants have recently been considered in cataract prevention, especially so for patients with frank and severe vitamin deficiency. Studies suggest that lens epithelial cell nuclear factor erythroid-2-related factor 2 (Nrf2) is an activator of endogenous antioxidants, preventing cataract. Notably, resveratrol (in red wine) and allicin (in garlic) are potent activators of Nrf2 [22].
From the oxidant stress side, homocysteine (related to hyperhomcystenuria, inborn errors of metabolism and dietary deficiency of abnormal methylation of B6, folic acid, and B12) within the endoplasmic reticulum (ER) was found to suppress NrF2, ostensibly resulting in cataract [23]. ER stress resulting from exposure of lens epithelial cell to homocysteine within fetal calf serum, resulted in significant degradation of Nrf2, within 24 h. The increased production of ROS decreased GSH reductase and catalase. Homocysteine exposure thus results in ER stress that suppresses Nrf2 dependent cellular antioxidant protection with subsequent death of lens epithelial cells. Nrf2 loss may also result from proteasomal degradation and increased cytoplasmic calcium. Thus high homocysteine concentrations induce ER stress, altering ROS generation, crystalline protein folding, and calcium balance. ROS regulation may help improve the lens epithelial cell Nrf2 pathway, reducing the rate of cataract formation [24].
10.4.1 Lutein and Zeaxanthin
There exist 600 known carotenoids in nature, with lutein and zeaxanthin as the two important dietary ocular xanthophylls found in both the lens and macula of the retina. Not surprisingly, the physiological concentration and function of these two nutrients are important in the prevention and management of both AMD and ARC. Lutein and zeaxanthin protect the eye from high energy blue light and possess powerful antioxidant activity [25].
Lutein and zeaxanthin are not endogenous and not synthesized by the human body. Therefore, there is great need for obtaining them through diet from dark leafy vegetables, such as spinach, kale, and broccoli, oranges, corn, and yellow and orange peppers [26].
The concentration of lutein and zeaxanthin in the macula of the retina can be quantified with instruments that measure macular pigment optical density (MPOD), which is a good indicator of visual function, eye health, and even overall systemic health [25]. The biochemistry of these two antioxidants is very similar. Zeaxanthin is a stereoisomer of lutein and it has a very similar mechanism of action to lutein. In the lens, they work by limiting lipid peroxidation, the primary cause for ocular and cardiovascular diseases.
Numerous studies illustrate the positive correlation between dietary supplements of lutein and zeaxanthin and reduced risk of AMD and ARC. A study by Seddon et al. with 356 subjects showed that the group who consumed 6 mg daily lutein and zeaxanthin had a 57 % decreased risk for developing AMD compared with those intaking 0.5 mg daily. Bernstein et al. showed that 4 mg daily supplementation of lutein increased macular pigment density, which is crucial for maintaining visual acuity and lowering risk of developing AMD [26].
The National Cancer Institute and U.S. Department of Agriculture recommend 5–6 mg daily lutein and zeaxanthin, which equals 5 servings of fruits and vegetables every day [25] (see Table 10.3).
Table 10.3
Nutrition, sources, roles and deficiencies in the United States
Nutrient | Main sources | Systemic role | Ocular role | RDA | % deficient in RDA intake | |
|---|---|---|---|---|---|---|
19–50 | >50 | |||||
B1 | Meat, fish, leafy vegetables, legumes, peas, whole grains | – Food and energy metabolism | Cofactor for antioxidant enzymatic reactions | M: 1.2 mg/day | M: 1.2 mg/day | 18.4 % (57 million) |
– Required for nervous system and muscle function | F: 1.1 mg/day | F: 1.1 mg/day | ||||
B2 | Meat, milk, eggs, green leafy vegetables, legumes, nuts | Body growth, red blood cell formation, releasing energy from carbohydrates | Cofactor for antioxidant enzymatic reactions | M: 1.3 mg/day | M: 1.3 mg/day | 10.9 % (34 million) |
F: 1.1 mg/day | F: 1.1 mg/day | |||||
C | Cantaloupe, citrus fruits, kiwi fruit, mango, papaya, pineapple, broccoli, brussels sprouts, spinach | Growth and repair of tissues | Located in aqueous compartments of lens membranes as an antioxidant and protect lens proteases from photooxidative destruction | M: 90 mg/day | M: 90 mg/day | 42.0 % (131 million) |
Repair and maintain cartilage, bones, and teeth immune system activity | F: 75 mg/day | F: 75 mg/day | ||||
E | Vegetable oils, nuts, seeds, green leafy vegetables | – Cellular health | Lipid soluble antioxidant concentrated in lens fibers, inhibit cataract formation by reducing photooperoxidation of lens lipids and stabilizing lens cell membranes | Adults: 15 mg/day | Adults: 15 mg/day | 86.4 % (271 million) |
– Immune system | ||||||
– Assist fertility | ||||||
Cu | Oysters other shellfish, whole grains, beans, nuts, potatoes, dark leafy greens | Red blood cell formation, health of blood vessels, nerves system, immune system, and bones | Cofactor for antioxidant enzymatic reactions | Adults: 900 μg/day | Adults: 900 μg/day | 15.8 % (50 million) |
Fe | Meat, oyster, fish whole grains, beans, broccoli, spinach | Structure oxygen-carrying proteins such as hemoglobin and myoglobin | (1) Role in cornea: completion of the citric acid cycle, production of ATP as well as an essential component of the rate-limiting enzyme in DNA synthesis | M: 8 mg/day | M: 8 mg/day | 10.5 % (33 million) |
F: 18 mg/day | F: 8 mg/day | |||||
Se | Meat, poultry, fish, eggs, grains | DNA repair, apoptosis, and the endocrine and immune system activity | Cofactor of glutathione peroxidases, an antioxidant enzymatic reactions | Adults: 55 μg/day | Adults: 55 μg/day | 8.5 % (26 million) |
Zn | Beef, pork, lamb, fish, nuts, whole grains, legumes, and yeast | Cell division, cell growth, wound healing, breakdown of carbohydrates, and immune system activity | Altering synaptic transmission, regulation rhodopsin reaction, modifier of photoreceptor plasma membranes, and antioxidant | M: 11 mg/day | M: 11 mg/day | 29.2 % (91 million) |
F: 8 mg/day | F: 8 mg/day | |||||
Lutein zeaxanthin | Lutein: spinach, kale, broccoli; zeaxanthin: orange, corn, and yellow/orange peppers | Prevent/limit lipid peroxidation | Increase macular pigmentation density | Adults: 5.8 mg/day | Adults: 5.8 mg/day | Not Determined |
Biological antioxidant | ||||||
10.4.2 Alcohol and Smoking
Smoking and alcoholism both have long-term destructive effects on human health, particularly in age-related diseases. The Blue Mountains Eye study investigated the effects of smoking and alcohol consumption on human lenses. The article, “Alcohol, Smoking, and Cataracts” by Robert G. Cumming et al. investigated the relationship between alcohol consumption, tobacco smoking, and cataractogenesis in a population-based cross-sectional study with 654 subjects. The authors concluded that smoking was associated with a higher rate of nuclear and posterior subcapsular cataract formation. Also, subjects abusing alcohol and smoking tobacco together showed a higher frequency of nuclear cataracts [27].
Another Blue Mountains study, “Alcohol Consumption and the Long-Term Incidence of Cataract and Cataract Surgery” by Gowri L. Kanthan et al. was a population-based prospective cohort study with 3,654 subjects aged 49 years and older. Interestingly, a U-shaped correlation between alcohol consumption and the long-term risk of cataract surgery was established. Subjects consuming over two standard drinks per day and subjects who abstained from alcohol consumption had a significantly higher prevalence of cataract surgery. In comparison, subjects consuming a moderate amount of alcohol (1 or less standard drink per day) had a 50 % lower incidence of cataract surgery [28].
Risk of smoking was investigated in the “Smoking and Risk of Age-Related Cataract: A Meta-Analysis.” The study concluded an association between long-term smoking and developing ARC, particularly nuclear cataracts. However, the results and the underlying physiological mechanisms require more investigation, although it has been established that smoke contains toxins as well as depressing serum ascorbic acid, a water soluble antioxidant found in high concentrations in all ocular tissues [29].
10.5 Systemic Diseases
10.5.1 Cardiovascular Complications
Several studies explored the association of aging cataractogenesis and systemic diseases such as cardiovascular complications. As mentioned, DM and high carbohydrate intake are recognized risk factors for ARC. However, hypertension and cardiovascular diseases are other systemic issues that have been investigated as well. Another Blue Mountains Study assessed the associations between DM, selected cardiovascular risk factors, and long-term incidence of cataract and cataract surgery. Three thousand six hundred and fifty-four Australians were initially selected for a 10-year longitudinal study. Age, gender, fasting glucose, blood pressure, and a few other factors were investigated separately. Results showed that baseline DM was associated with nuclear cataracts and impaired fasting glucose was associated with cortical cataracts. Subjects with higher body mass index (BMI) presented with posterior subcapsular cataract. Also, subjects taking anti-hypertensive medications had a higher incidence of cataract surgery with few associations also found between cardiovascular risk factors and long-term cataract development [30].
Free radicals can cause oxidative damage to lipoproteins and increase the risk of atherosclerosis. In this regard, Frank B. Hu et al. hypothesized that cataracts from free radical oxidative stress could be a marker for atherosclerosis, particularly coronary heart diseases. During a 10-year study on women aged 45–63 years with no known coronary disease, stroke, or cancer, the authors confirmed that cataract extraction was significantly associated with higher risk of coronary heart diseases and overall mortality [31].
10.5.2 Mortality
ARC and visual impairment are associated with reduced life expectancy and quality of life. A survey of visual impairment and blindness between 1996 and 2000 recruited 10,293 individuals from urban and rural clusters in Andhra Pradesh, India. Participants were followed in an effort to determine ocular risks factors associated with visual disability, cataract, and mortality. From this cohort study, 799 of 4,188 participants with visual problems had died (19.1 %) and 308 participants had migrated. Mortality in males was greater than in females a decade later. The study indicated that any type of cataract or history of cataract surgery increased the mortality rate. It further suggests that cataract is a marker of aging [32].
Another study comparing mortality risk in cataract patients, by degree of opacification, is instructive. One thousand eight hundred and sixty-four patients aged 64 years and older undergoing phacoemulsification surgery were followed for 5 years postoperatively. Of 901 patients with moderate and severe visual impairment before cataract surgery, 60.4 % showed no visual complaints, 15.5 % had mild problems, and 24.1 % of the patients remained with severe visual impairment 1 month postoperatively. While age-standardized mortality rates were not significantly lower in patients with mild or no visual impairment, correcting moderate and severe visual impairment in elderly patients with phacoemulsification surgery resulted in statistically significant lower mortality compared to that of un-operated patients [33].
The Blue Mountain Eye study cohort evaluated the relationship between cataract surgery and quality of life. In this study, 354 patients aged 49 years and above with visually significant cataract, underwent surgery and were examined 5 and 10 years later. Patients who underwent surgery had better vision and enjoyed significantly lower long-term mortality risk, than individuals with untreated cataract(s). Thus cataract surgery induced visual improvement associated with long-term survival. Other visual impairments were similarly associated with increased mortality [34].
However another study illustrates increased mortality rate among cataract surgery patients and cohorts following phacoemulsification. Data were collected for 933 consecutive patients in 2006 who underwent surgery between 2000 and 2001. The data were later negatively correlated with regional and standard mortality risk. This study is contrary to similar studies as cataract surgery is universally associated with improved survival and quality of life indices. Nonetheless, this illustrates the importance of continuous research and re-evaluation of medical knowledge in light of changes in population demographics and practice [35].
In summary, there is an increased mortality rate among patients with visual impairment in general and ARC specifically. Scientific evidence suggests that cataract is associated with deterioration of health status, as well as quality of life. Patients suffering from cataract and other visual impairments must seek medical care. Cataract surgery has the potential to permanently cure cataract related visual disability resulting in an improved quality of life.
10.5.3 Osteoporosis
Calcium is one of the essential minerals found abundantly in the human body. Calcium imbalance, particularly in the elderly, causes diverse physiological issues involving neurological, muscular, and skeletal tissues. Calcium assists electrolyte homeostasis in terms of cellular transport, renal function, enzymatic activation, and cellular division and communication. Hypercalcemia and hypocalcemia are related to symptoms such as nausea, vomiting, muscle weakness, sudden twitches, memory loss, depression as well as paresthesia in hands and feet, anxiety, seizure, and arrhythmias, respectively [36].
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


