2 The Eyelids
NORMAL ANATOMY
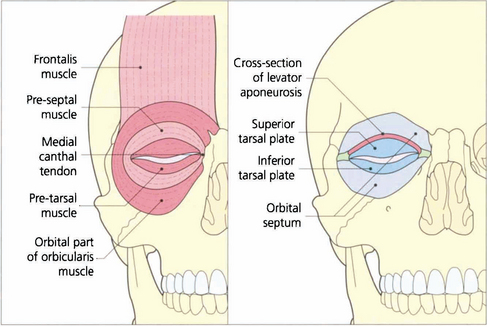
Fig. 2.1 Diagrammatic view of the structures of the normal eyelid. The orbicularis muscle can be divided into the pretarsal, the preseptal and orbital parts although these are not separate anatomically. The pretarsal and preseptal parts together form the palpebral section of the orbicularis muscle which is responsible for blinking and facilitates the drainage of tears (see Ch. 20) and the orbital part is responsible for forced lid closure. The grey line is where orbicularis oculi meets the lid margin. This visible line lies anterior to the meibomian gland orifices and posterior to the eyelashes. It is the plane at which the anterior and posterior lamella can be separated during surgery. Removal of the orbicularis muscle exposes the underlying tarsal plates and orbital septum. The levator aponeurosis is the tendon of the levator muscle which inserts between the orbicularis muscle bundles and is responsible for the eyelid skin crease.

Fig. 2.2 The pre-aponeurotic fat pad lies behind the orbital septum. If it is elevated, the levator palpebrae superioris muscle with its aponeurosis is seen. Whitnall’s ligament (the superior suspensory ligament of the globe) is a thickening in the aponeurosis that helps to support the aponeurosis and the upper lid retractors. It runs from the periosteum of the lacrimal gland fossa to the trochlea of the superior oblique muscle. The inferior aponeurosis is the forward extension of the connective tissue from Lockwood’s ligament (the inferior suspensory ligament of the globe) and is continuous posteriorly with the sheath around the inferior rectus muscle (see Fig. 2.5).
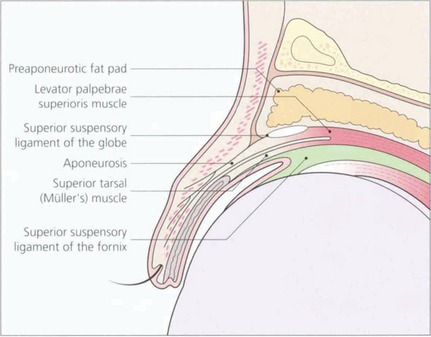
Fig. 2.3 The upper lid structures can be compared in diagrammatic and histological vertical sections. The levator palpebrae superioris muscle inserts into the anterior lamella and the posterior lamella (Müller’s muscle), both of which are responsible for lifting the eyelid. The connective tissue between the levator muscle and the superior rectus muscle (the common sheath) extends forward to support the upper conjunctival fornix (superior suspensory ligament of the fornix).
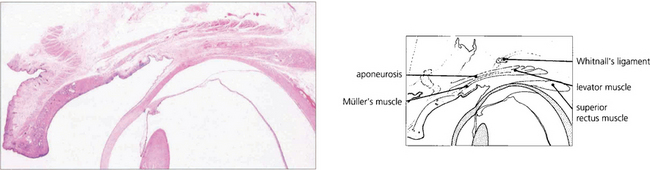
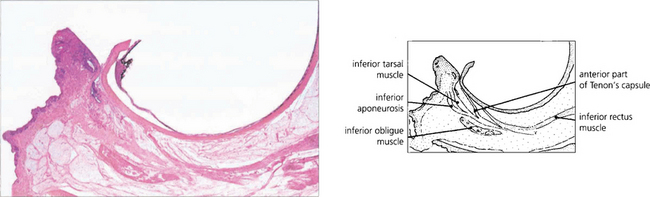
Fig. 2.4 Histological section of the upper lid corresponding to the cross-sectional diagram of Fig. 2.3.
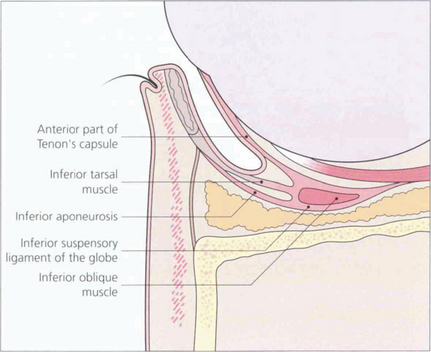
Fig. 2.5 Sections of the lower lid show the arrangement of the lower lid retractors. A condensation of fascia around the inferior oblique muscle forms the inferior suspensory ligament of the globe (Lockwood’s ligament). This is analogous to Whitnall’s ligament in the upper eyelid. It is attached medially and laterally in the region of the canthal tendons and can support the globe if the orbital floor is removed. The inferior aponeurosis extends forwards from Lockwood’s ligament with the inferior tarsal muscle (analogous to Müller’s muscle in the upper lid). These are the lower lid retractors which are responsible for depressing the lower eyelid on downgaze due to their connection with the inferior rectus muscle. A forward extension of the connective tissue associated with the lower lid retractors forms the inferior suspensory ligament of the fornix and anterior part of Tenon’s capsule.
CONGENITAL EYELID ABNORMALITIES
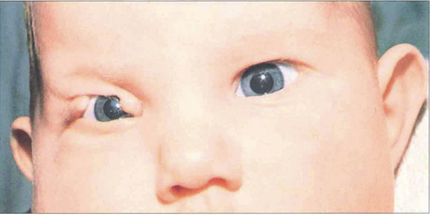
Fig. 2.7 Congenital lid colobomas are the result of a failure of normal development of the eyelid and closure of the facial clefts. Urgent repair is required only if the defect is so severe that the cornea is likely to suffer permanent damage from exposure.

Fig. 2.8 Epicanthic folds are abnormal folds of skin at the medial canthus. They are common in childhood, especially in children of oriental origin, but they may also be acquired as a result of tissue loss from trauma. Congenital epicanthic folds frequently give an appearance of pseudostrabismus (see Ch. 18). They usually become less obvious with age but, if they persist, both congenital and acquired folds can be treated by a variety of plastic surgery procedures.

EYELID MALPOSITION
All forms of eyelid malposition may be congenital or acquired.
ENTROPION
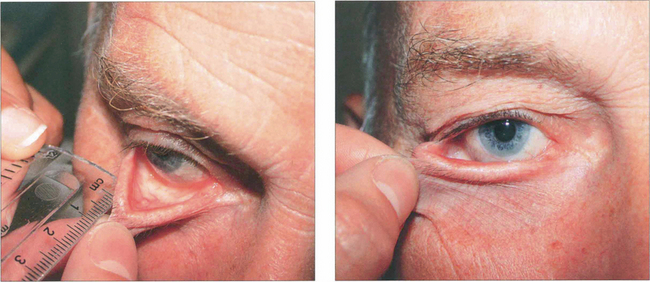
Fig. 2.10 Horizontal lower lid laxity is assessed by grasping the lower lid skin and applying gentle traction away from the globe. (a) The extent to which the lid can be lifted off the globe is measured in millimetres; more than 6 mm is considered abnormal. (b) Laxity of the medial canthal tendon is assessed by gently pulling the lid laterally. The position of the punctum in relation to the limbus or pupil in primary gaze is then recorded. Lack of a lower lid skin crease in downgaze implies disinsertion of the inferior retractors.

Fig. 2.11 Congenital lower lid entropion is caused by hypertrophy of the skin and underlying orbicularis muscle. A mild degree of this hypertrophy is common in young children (epiblepharon) and, rarely, the eyelid margin itself inverts (congenital entropion). Should this fail to improve with age and cause irritation of the eye, it is corrected by the excision of the hypertrophic skin and underlying orbicularis muscle.
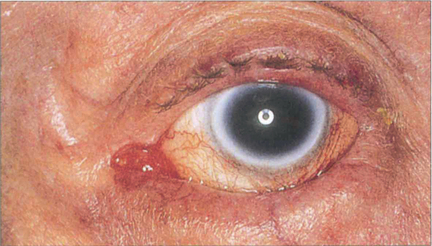
Fig. 2.12 Involutional entropion is a common condition caused by ageing changes affecting the orbicularis muscle, the lower lid retractors, the tarsal plate, the medial and lateral canthal tendons and the orbital fat. A variety of operations has been described to correct various combinations of these defects. These include sutures or incisions designed to prevent the upward movement of the preseptal muscle, tightening the lower lid retractors, eversion of the upper border of the tarsal plate and horizontal lid and canthal tendon shortening procedures.

Fig. 2.13 Cicatricial changes can affect the posterior lamella of either the upper or lower lid and lead to entropion. This patient has scarring and shrinkage of the tarsal plate and conjunctiva. Common causes include trauma, acid and alkali burns, trachoma and other chronic conjunctival inflammations such as chronic staphylococcal lid disease, ocular pemphigoid or Stevens–Johnson syndrome. It may be possible to correct a cicatricial entropion with an everting procedure and rotation of the tarsal plate but if there is a marked degree of lid retraction a posterior lamellar graft will be required to lengthen the posterior lamella.
ECTROPION

Fig. 2.14 Congenital ectropion in neonates and very young children may be caused by crying and spasm of the orbicularis muscle. This does not usually require any treatment. If there is a shortage of skin, as in the case illustrated here, skin replacement is necessary with a graft or flap.
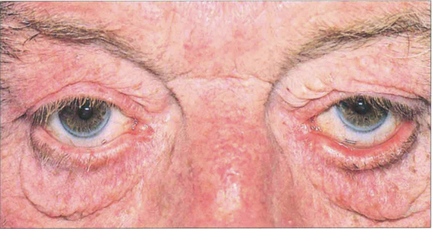
Fig. 2.15 Involutional lower lid ectropion is caused by a generalized laxity of all the lid tissues aggravated by gravity. Various operations have been described to correct the condition; most of these involve a horizontal shortening procedure of one or both lamellae or tightening of the canthal tendons with or without the removal of excess skin and orbital fat. Chronic exposure may cause conjunctival keratinization, punctal stenosis and chronic infection.

Fig. 2.16 Cicatricial lower lid ectropion may be caused by any condition that leads to a shortage of skin. This patient fell off his bicycle and lost skin; the resultant scarring caused a cicatricial ectropion. Surgical correction involves excision of the scar tissue, and replacement skin grafting. The lid must be shortened at the same operation if it has been stretched excessively by the scarring.
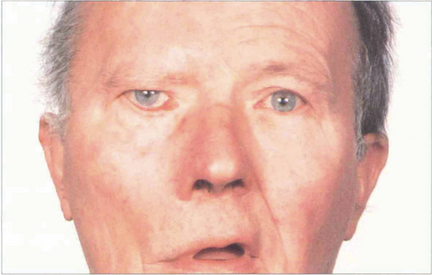
Fig. 2.17 Paralytic ectropion is caused by weakness of the orbicularis muscle (seventh nerve palsy) and subsequent lid laxity. Corneal exposure may be a problem, particularly if there is reduced trigeminal sensation (e.g. with a cerebellar pontine angle tumour such as acoustic neuroma). Bell’s phenomenon protects the cornea on forced eyelid closure, but is not always present. The cornea can be protected by transient ptosis induced by botulinum toxin if recovery of the seventh nerve palsy is expected. Medial canthalplasty and a lateral canthal sling may help, and a variety of other procedures such as fascia lata slings may be useful. The loss of brow wrinkling indicates this patient has a lower motor neurone seventh nerve palsy.
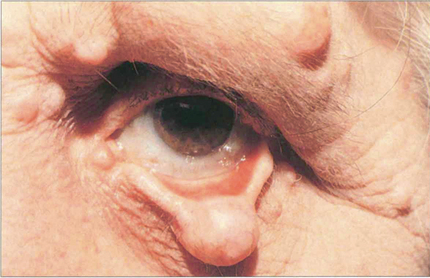
Fig. 2.18 Any form of lump on the lower lid can lead to a mechanical ectropion. The patient illustrated here has a localized neurofibroma of the lower lid. Treatment involves the excision of the tumour and correction of any induced horizontal laxity of the lid.
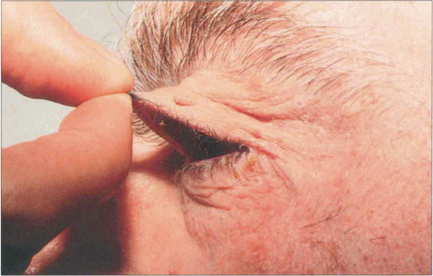
Fig. 2.19 The characteristics of the floppy eyelid syndrome are easy evertion of the upper lid and a chronic papillary conjunctivitis (which is caused by the mechanical abrasion of the upper tarsal conjunctiva on the lower lid lashes). It is associated with obesity and sleep apnoea and is a risk factor for cardiovascular and cerebrovascular disease. Patients need investigation for these underlying conditions.
PTOSIS
Blepharoptosis (ptosis) is a reduction in the vertical palpebral aperture due to descent of the upper lid as a result of pathology involving the eyelid retractors. A useful classification of ptosis can be made by considering pseudoptosis and congenital or acquired ptosis (Table 2.1
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


