The Eye and Sports Medicine
Paul F. Vinger
The ideal scenario for a sports (or any other) eye injury is for it never to have happened. Prevention, effective in terms of both injury reduction and cost savings to society,1,2,3,4,5,6 should be part of the core curriculum of anyone who prescribes, manufactures, or dispenses eyewear, as well as those in the capacity of formulating and implementing rules in the athletic environment.7 According to the Centers for Disease Control and Prevention, “Injury is probably the most unrecognized major health problem facing the nation today, and the study of injury presents unparalleled opportunities for reducing morbidity and mortality and for realizing significant savings in both financial and human terms—all in return for a relatively modest investment.”8 By following the guidelines for specific sports presented in this chapter, eye care professionals, sports officials, and participants will significantly reduce the risk of eye injuries without changing the essential nature or appeal of sports.
EPIDEMIOLOGY
Without knowledge of the incidence and severity of sports-related eye injuries, it would be difficult to attempt injury reduction since there would be no way to determine whether preventive methods were indicated or if they had an adverse or beneficial effect. A major potential pitfall in studying epidemiologic data is that the data obtained may reflect only the risk of a sport and not the benefits that may or may not justify the risk.9 The objective is to reduce preventable eye injuries to the minimum consistent with retaining the benefits—the fun and appeal that draw participants into the sport. It is possible to achieve this goal most of the time after the incidence and mechanism of eye injuries are ascertained and a committee representing all concerned with the sport—athletes, coaches, officials, and the medical profession—meets to solve the problem.
In 1991, the National Institutes of Health Conference on Surveillance Strategies for Sports Injuries in Youth recommended the creation of a universal database,10 yet two decades later there still is no system that records all sports eye injuries with a numerator (injuries, injury details, and use of protective equipment) and a denominator (participants, exposures, player skill) from which the injury risk to both the individual and society can be calculated. In the absence of such a system, the incidence of sports eye injuries and the effect of injury prevention programs must be approached either from studies that emphasize the risk to society and attempt to measure the total number and severity of injuries in a given population or from the study of a small controlled population from which risks to the individual can be estimated.
It is essential to realize that injuries are not accidents. Instead, they have definite patterns and distinct nonrandom characteristics.11,12 By carefully evaluating the underlying mechanisms, patterns, and rates of injury in a given sport, it is possible to design and implement extremely effective preventive programs.
RISK TO SOCIETY
Although incomplete, the data show that eye trauma is a major public health problem,13,14,15 of which sports comprise a significant proportion.3 Sports and recreation accounted for 10% of all hospital-treated eye injuries in Dane County, Wisconsin, in 197916 and 65% of all eye injuries to children in Israel from 1981 to 1983.17 Sports-related injuries were responsible for 60% of hyphemas and 10% of open-globe injuries in 3184 patients seen in the Massachusetts Eye and Ear Emergency Room over a 6-month period.18 Approximately one fourth of all trauma admissions to the Manchester Royal Eye Hospital in 1987 and one sixth of all trauma admissions to the Wills Eye Hospital over a 3-year period were secondary to sports-related injuries.19,20,21 Sports-related injuries (BB gun, golf, basketball) resulted in four enucleations in Olmstead County, Minnesota, between 1956 and 1988.22 BB and other sports injuries are common in children.21,23 In 11- to 15-year-old children, sports and recreational activities accounted for 27% of all eye injuries.24 Injuries result in visual acuity of less than 20/200 secondary to the development of amblyopia in the injured eye in more than 40% of children injured before the age of 10 years.25 The vast majority of injured players were not wearing any form of protection at the time of injury.4,26,27
Regional injury data often reflect the local popularity of a sport and do not necessarily reflect the risk to an individual participant. Playing with bow and arrow and gillidanda accounted for most of the sport injuries (47.2%) in northwest India,28 but neither of these activities appear in the data from the United States and Canada. From a societal perspective, the focus of prevention must vary from one location to another. However, basic mechanisms of injury are often similar for different sports.
Data Sources
There are several sources of injury data, some more useful than others:
The National Safety Council system and state data collecting systems have been of little value in the study of sports-related eye injuries because their data are difficult to obtain and are often inconsistent. Gathering of statewide data29 from hospital records is often impeded by the method of hospital record keeping, which often fails to identify the cause of injury or the circumstances surrounding the injury.
The National Athletic Injury/Illness Reporting System (NAIRS) has, in the past, obtained useful data by following injury rates in participating schools.30 However, the data are no longer available.
In 1985, The Centers for Disease Control (CDC) consolidated its nonoccupational injury research efforts into the Division of Injury, Epidemiology, and Control. The reports on eye injuries thus far have not been detailed enough for use in monitoring sports eye injuries.
The National Electronic Injury Surveillance System (NEISS) was established under a 1973 congressional mandate that established the U.S. Consumer Product Safety Commission (CPSC) to protect the public from unreasonable risks of injury and death associated with consumer products.31 NEISS is the core of CPSC’s Bureau of Epidemiology and currently comprises 100 hospital emergency departments that make up a stratified sample of all hospital emergency departments throughout the United States and its territories. NEISS data—categorized by body part, product, and activity—are good for estimating the total social cost of injuries that affect large segments of the population. NEISS is limited because only emergency department visits related to injuries caused by products are recorded as the basis for projections of a national probability. Since specialty eye hospitals and private ophthalmologists’ offices, where most of the sports-related eye injuries are seen, are not included in the sample, NEISS data must be viewed with caution. For example, the extreme eye injury hazard of boxing is not apparent from NEISS data. Yet national trends (e.g., the large number of basketball and baseball eye injuries) are often apparent from these data (Table 1).
The National Eye Trauma System (NETS) is a consortium of approximately 50 regional eye trauma centers that prospectively gathers information on the etiology, treatment, and final results of open-globe eye injuries. However, most sports-related eye injuries are caused by blunt objects and do not penetrate, perforate, or rupture the globe, and thus are not recorded. Despite the fact that the consortium misses most sports-related injuries, it is astounding that 14.1% of all injuries in the NETS database are from sports. As expected, injuries caused by projectiles (38.1% of reported recreational injuries were due to BB/air guns) lead the NETS list of perforating injuries due to sports.2,32
The United States Eye Injury Registry (USEIR) was formed in December 1988, modeled on the Eye Injury Registry of Alabama, which began in 1982. USEIR, now a federation of 40 state registries and the United States Military Eye Injury Registry, collects and disseminates comprehensive data on the occurrence of serious (involving permanent or significant structural or functional changes to the eye) ocular injuries. USEIR provides data on a broad spectrum of eye injuries, including blunt trauma and chemical injuries that are frequently seen only in ophthalmologists’ offices. Because of underreporting by ophthalmologists, USEIR captures approximately 0.3% of sports and recreational eye injuries (about 400,000 in NEISS and 1,300 in USEIR over 10 years).33 Table 2 is a summary of USEIR sports eye injury data.
Table 1. Estimated Number of Eye Injuries Treated in Hospital Emergency Departments | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 2. USEIR Sports and Recreation Eye Injuries December 1988 to September 1999 and Jan 2000 to Jan 2010 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Data collected by the cooperating ophthalmologists of the Canadian Ophthalmological Society (COS)4 under the leadership of the late Tom Pashby (March 23, 1915–August 24, 2005), have been useful for following trends in sports-related injury and the results of intervention with rules changes and/or protective devices. Since, like USEIR, the COS system depends on the voluntary reporting of cases by individual ophthalmologists, the reported cases are an indeterminate small percentage of the actual injuries. Without Pashby’s leadership, data collection and reporting have atrophied and no update is available.
Sporting Goods Manufacturers Association (SGMA) International compiles the most reliable estimates of sports participation in the United States.34 Data for specific sports are included in the discussions of individual sports. SGMA International details participation trends in 103 fitness, sports, outdoor, and recreational activities, based on a nationally representative sample of 14,276 adults and children. Sports participation falls into approximately three fairly equal groups: 86.1 million participate frequently; 83.6 million participate occasionally; 81.3 million do not participate. Combining these data with the data of NEISS gives a somewhat better perspective. The fact that soccer participants increased from 2.3 million in 1990 to 4.3 million in 2001 suggests that the increase in total soccer eye injuries (1492 in 1990 to 2153 in 2001) may be due to an increase in players at risk rather than a change in incidence.
RISK TO THE INDIVIDUAL
More important to the athlete than the injury statistics noted previously is the risk of a specific sport to an individual participant. Despite the lack of an ideal data collecting system, it is possible to ascertain the eye injury potential of various specific sports and follow the results of intervention, with rules changes or protective equipment, by means of limited, specifically designed studies.35
The National Collegiate Athletic Association (NCAA) Injury Surveillance System (ISS) was developed in 1982 to provide current and reliable data on injury trends in collegiate sports.36 The NCAA was established in 1906 in response to the concerns of Theodore Roosevelt for college football injuries and deaths; thus, at first, only football data were collected. The ISS has expanded to also include wrestling (men’s); basketball, soccer, lacrosse, and gymnastics (men’s and women’s); and field hockey, volleyball, and softball (women’s). Participation is limited to the 977 NCAA member institutions with ISS participants picked at random to have a minimum 10% representation of each NCAA division (I, II, and III). Data from the NCAA do not record every injury but are a sampling that is representative of the total population of NCAA institutions sponsoring a particular sport. ISS gives the eye injury rate per 1,000 exposures,37 but it is difficult for many to judge risk unless the NCAA data are put into more understandable terms. The NCAA incidence figures can be multiplied by the average exposure (number of games and practices) to give an easily understood risk to the individual per season and per school career—8 years high school and college (Table 3).
Table 3. Eye Injury Risk, NCAA | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
It has been more than 20 years since the National Society to Prevent Blindness (NSPB, now called Prevent Blindness America) made recommendations that sports-related eye injury data gathering fulfill the following criteria: (i) to permit population-based comparisons involving a known denominator; (ii) to record demographic data and details of the injury at the time of presentation to the medical facility; (iii) to record the diagnosis of the physician at the time of examination; and (iv) to record the final outcome of the injury.3 As can be seen from the data-gathering systems presented, data collection has a long way to go to realize these recommendations.
The analysis of input from many reporting sectors is needed to comprehend the magnitude of sports injuries, the need for protective programs, and the effectiveness of implemented programs. From the preceding and the data to follow, it is possible to approximate the eye injury risk to the unprotected participant from selected sports (Table 4).
Table 4. Sports Eye Injury Risk to the Unprotected Player | |||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
ECONOMICS OF EYE INJURIES
The social cost of eye trauma, the most common ophthalmic indication for hospitalization, is enormous. National projections estimate annual U.S. hospital charges of $175 million to $200 million for 227,000 eye trauma hospital days.38 Eye injuries seen in 6 months in one emergency department are responsible for direct and indirect costs totaling $5 million and a loss of 60 work-years.18 The average societal cost for an eye injury to a child younger than the age of 15 playing basketball is $3,996.39 It is estimated that of the 1.6 to 2.4 million Americans who sustain eye injuries each year, 40,000 will be legally blinded in the injured eye. About one third of these injuries result from sports.40 Since essentially all sports-related eye injuries are preventable, the potential economic savings resulting from the prevention of these injuries is great. There is no question that prevention of traumatic sports-related eye injuries is cost-effective.41 In 1980 dollars, the hockey face protector saves society $10 million a year by preventing approximately 70,000 eye and face injuries in 1.2 million protected players.42
Total expenditures for preventive health care amounted to less than 2.5% of total health care expenditures with less than 0.5% spent on health education.43 Despite the fact that injuries are one of the leading causes of physician and hospital visits, the amount allotted by Congress and the National Institutes of Health (NIH) for trauma research is less than 1% of the money allotted for cancer and heart disease.11
MECHANISMS OF EYE INJURIES
The analysis of trauma is commonly expressed in International System of Units (SI), which is the worldwide standard.44 Since it is hard for many of us to visualize what some SI units actually measure (Is it very dangerous to collide with a football player who weighs 200 N at 5 m/s?), more understandable units, such as miles per hour (mph), will be used when appropriate. It is easier for most of us to grasp the speed of a baseball when the velocity is expressed as 75 mph rather than as 33.53 m/s.
The severity of an eye injury is correlated with the total impact force, expressed in newtons (N), and the impact force onset rate, expressed in newtons per millisecond (N/ms), and the kinetic energy, expressed in joules (J) of an impacting object. There is an eye-injury progression from chamber angle damage to peripheral vitreoretinal damage to ruptured globe as the force increases and the time to maximum force decreases.45 If we slow the velocity of a BB (0.345 g) to 29 mph (13 m/s; 43 ft/s), the energy will be less than the kinetic energy of 0.03 J required for an ocular contusion and there will be no eye injury. However, when fired in the horizontal direction from a height of 5 feet, the BB would travel only 24 feet.46 As the BB velocity increases, the injuries get more severe: 62.3 m/s (205 ft/s) will result in injury at the vitreous base and retinal tear; 72.0 m/s (236 ft/s) penetrates the globe; 124 m/s (408 ft/s) penetrates skin, bone, and moderate tissue.46,47
Test devices48 and mathematical models45 have been devised for the laboratory testing of various products, such as toys, to access the potential for eye injury. The force onset rate needed to produce clinically detectable contusion injury by a blunt object is approximately 750 N/ms. Some toy dart guns (896 N/ms) that propel suction cups exceed this level, whereas most toy Ping-Pong ball shooters (428 N/ms) do not.49 Computer modeling using finite element analysis has led to better analysis and understanding of the mechanisms of eye injury (Fig. 1).50,51,52,53
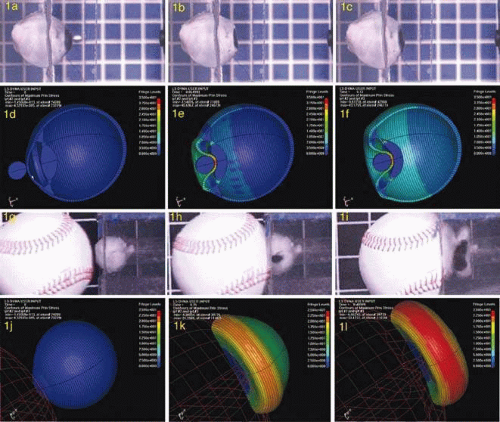 Figure 1. Finite element analysis correlated with motion analysis of impacts on human eyes. A–C. BB, moving right to left at 92.0 m/s (301.8 ft/s; 0.58 J) impacting a human cadaver eye held in an artificial orbit with clear gelatin. The sequence will be continued in the section on BBs to follow. D–F. Finite element analysis (FEA) of the BB impact to a point just before globe penetration. G–I. Baseball, moving left to right at 41.2 m/s (92.2 mph; 124.3 J) impacting a human cadaver eye held in an artificial orbit with clear gelatin. Note globe rupture (dark area) at equator of the globe starting in H and enlarging in I. See Figure 5 for the baseball rebound. J–L. Finite element analysis (FEA) of the baseball impact to a point just before globe penetration. This FEA model has potential usefulness as a simulation tool for ocular injury, and it may provide useful information for developing protective measures against sports, industrial, and traffic ocular injuries. (Courtesy of Stefan Duma and Joel Stitzel. Virginia Tech Impact. Biomechanics Laboratory [duma@vt.edu].) |
Many protectors (such as football helmets) for sports and some protective eyewear54 prevent or reduce injury by decreasing the force onset rate and the peak force by spreading the total force over time. However, the injury as related to force onset rate applies only to total forces in a limited range, which has not yet been determined.
INJURY CLASSIFICATION
Sports eye injuries can be classified in accordance with the Birmingham Eye Trauma Terminology (BETT) in which all terms relate to the whole eyeball as the tissue of reference.55 Injuries may be as follows:
Open-globe injury in which there is a full-thickness wound of the eye wall:
Rupture: wound caused by a blunt object, eye ruptures at weakest point (“inside out” mechanism)
Laceration: wound caused by a sharp, or small high-velocity, object at site of impact (“outside in” mechanism):
Penetrating. Each entrance wound caused by separate agent; includes intraocular foreign body
Perforating. Entrance and exit wound caused by same agent
Closed-globe injury in which there is no full-thickness wound of eye wall:
Contusion:
Due to direct energy delivery by the object
Due to changes in the shape of the globe
Lamellar laceration: partial-thickness wound of the eye wall
Open-Globe Injuries
The eye wall (the cornea and the sclera) can be modeled as the union of two thin-walled (approximate 0.5-mm wall thickness) spheres (radii 8 mm and 12 mm) with the centers 5 mm apart.56 At the junction of the optic nerve sheath, which may be represented by a cylinder (radius 2 mm), the larger (scleral) sphere is perforated by multiple openings, the lamina cribrosa.57 However, the eye wall is not of uniform thickness,58 is significantly thinner in myopic eyes,59 and becomes less elastic with age.60 The eye wall tends to rupture in three specific locations: (i) where the radius of curvature changes at the limbus; (ii) where the sclera is the thinnest, near the equator behind the ocular muscles; and (iii) where the sclera is perforated at the lamina cribrosa.56
Even with the best surgical techniques, approximately 50% of children with open-globe injuries recover good visual acuity.61
Rupture
Ragged rupture of the globe secondary to injury by a blunt object significantly reduces the likelihood of recovery of useful vision.13,62,63,64,65 Only 7 of 13 ruptured eyes regained counting fingers or better vision.66 Rupture of the globe occurs when the intraocular pressure is greatly elevated or when a blunt external force is applied to the eye quickly. The energy required to rupture the eye varies with the dimensions and the properties of the impacting object (Table 5). Figure 2 shows a matched pair of cadaver eyes impacted with baseballs that had similar physical properties—except for the ball hardness. Impact with a major league baseball (143.9 g) at 55 mph ruptures the globe at 3 ms. Impact with a softer ball (146.5 g) at 74 mph does not rupture the globe, despite the fact that the softer ball delivered more energy (80.2 joules) than did the harder ball (43.5 Joules).67 The harder baseball causes extreme flattening of the globe (2 ms) immediately followed by rupture at the limbus (3 ms). After the ball has totally rebounded from the eye and orbit, the ocular contents continue to be extruded by the retained energy in the globe. When compared to the softer baseball that does not rupture the globe, it is apparent that the harder ball delivers energy faster, deforms the eye more, and rebounds faster. The softer ball has a lower peak force and slower force onset rate (peak force 3,208 N; onset rate of 2,686 N/ms) than the harder ball (peak force 3,768 N; onset rate of 3,486 N/ms). It appears that the slower application of force allows the globe to retract into the orbit and undergo less compression than when the force is applied faster. The rupture pressure of a healthy human eye varies with force onset rate and is in the range of 2,000 to 4,400 mm Hg.68,69
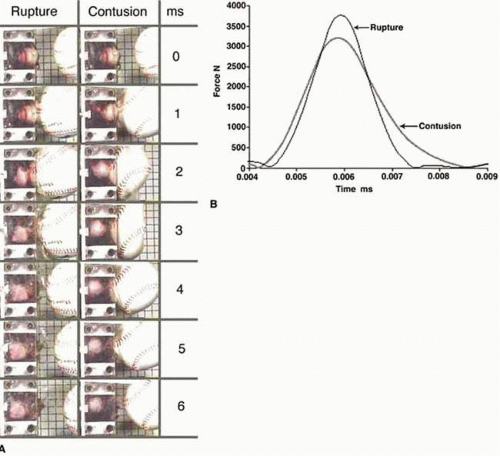 Figure 2. Rupture and contusion related to time in milliseconds (ms) and force onset rate. |
Table 5. Globe Rupture: Correlation among Intraocular Pressure, Object Hardness, Size, and Kinetic Energy* | ||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||
The sports that cause ruptured globes to unprotected players typically use a stick with a blade end that fits into the orbit (hockey, field hockey, golf, polo), a small soft fast projectile (BB, paintball), a soft or hard ball that deeply penetrates the orbit (squash, golf), a hard projectile that partially enters the orbit with great force (hockey, baseball, softball, cricket, field hockey, polo), or one in which there is the potential of contact with a body part that enters the orbit with force (basketball, football, soccer, rugby, boxing, martial arts).
Prior Surgery or Eye Disease
An eye that would have had a closed-globe injury may sustain an open-globe injury (rupture) because surgery has weakened the eye wall.70 Deeper, longer incisions, especially in the cornea, permanently weaken the eye wall and predispose the eye to an open-globe injury. Table 6 lists the approximate risk from various surgical procedures. All patients who have had surgical procedures that weaken the eye wall should be advised that eye protection is essential when there is the probability of impact.71 The concept that a ruptured globe is a “safety valve” that prevents contusion injuries cannot be supported by injury data (Fig. 3).
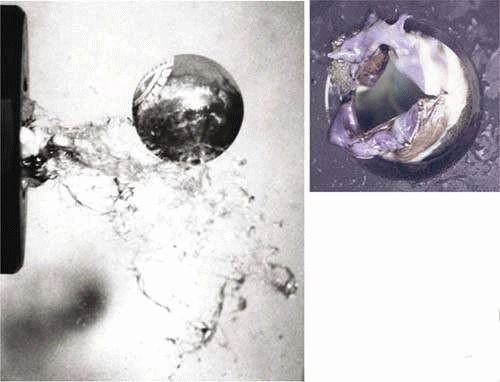 Figure 3. Total extrusion of RK eye contents. Squash ball impact at 90 mph. |
Table 6. Predisposition to Traumatic Ruptured Globe after Eye Surgery | |||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Laceration
Perforating injuries, in which the same agent causes an entry and an exit wound, are usually due to a high-speed projectile (air rifle/BB, firearm, shrapnel) or a slower sharp projectile (shattered eyewear, fishhook, tip of ski pole, arrow, dart). There are few data on the energy required to cause perforating injuries, which are similar to but more severe than penetrating injuries.
Penetrating Injuries
The same agents that cause perforating injuries result in penetrating injuries or intraocular foreign bodies when there is sufficient energy to penetrate the eye wall but not enough energy to exit the globe. A knife-edged missile is in a class by itself for ease of penetration. The mechanical advantage of the cutting edge is exerted until the hole it makes is the full diameter of the missile. A 20-gauge knife-edged missile penetrates the globe with a momentum of 17 mg·ms72 as compared to the momentum of 24,840 mg·ms as the no-penetration value for the BB.47
The energy present in many sports is capable of causing severe eye injury and often exceeds the capacity of ordinary eyewear to withstand the impact and protect the eye. Frequently, the lacerating instrument is a fragment of the athlete’s own spectacle lens. Thus, the wrong eyeglasses can convert blunt trauma into penetrating ocular injury and permanent visual impairment73,74,75 Globe laceration caused by spectacle lens shatter has a poor prognosis and is underestimated. Keeney76 found 491 cases of spectacle glass injuries resulting in 369 ocular injuries and 37 lost eyes. Over a 1-year period, 3.6% of 446 cases of penetrating ocular injury in Canada were due to shattered spectacle lenses—40% of the shattered lens injuries were to adult male amateur athletes.77 Between 1978 and 1986, at least 21 racket sport players sustained serious ocular injuries when their prescription glasses (hardened glass or plastic, but not polycarbonate or TriVex) shattered.78,79 Of 298 eyes injured by shattered spectacle lenses in a nonindustrial setting, 157 suffered significant damage and 27 were lost. Sports accounted for 53 (17.8%) and BBs for 16 (5.4%) of the shattered eyeglasses.80 Sixteen of 635 work-related penetrating eye injuries resulted from shattered streetwear spectacle lenses.81 One of the two penetrating ski eye injuries reported to NETS was the result of dress spectacles shattering on impact from the handle of a ski pole. Two soccer players had significant structural changes to their lids and globes when the ball shattered streetwear glasses.82 A homemade “potato gun” caused a sight-threatening corneal laceration when the spectacle lens worn by a 14-year-old boy shattered.83
Since approximately half of the population wears eyeglasses,84 the prescription of the appropriate spectacle lens (Fig. 4) can protect a huge segment of the population, whereas an incorrect recommendation by the practitioner exposes the patient to the risk of a shattered lens, a perforated globe, and the good chance of permanent disability.85
 Figure 4. Impact resistance of eyewear lenses. Top row. BB impacts on (A) polycarbonate, (B) glass, (C) allyl resin plastic (CR-39), (D) high-index (1.6) plastic lenses. Center row. Baseball impact on industrial safety lenses (left) polycarbonate at 169 ft/s (note flattening of baseball), (center) glass, chemically tempered at 142 ft/s, (right) allyl resin (CR-39) plastic at 137 ft/s. Bottom row. A 500-g high-mass Z87 test object from left to right onto TriVex, polycarbonate, CR-39, high-index (1.6), and Spectralite lenses. All lenses 2 mm thick plano. Mass dropped from 75″ (9.34 J) onto TriVex and polycarbonate, which did not shatter, and from 50″ (6.23 J) on the other lenses, which shattered. (Bottom row courtesy of Nancy Yamasaki.) At velocities expected in typical sports, glass, allyl resin, and high-index plastic lenses shatter, whereas polycarbonate (and also TriVex) remain intact. |
Apart from shattered eyewear, the principle causes of intraocular foreign bodies seen in sports are BBs, shotgun pellets, and fishhooks.
CLOSED-GLOBE INJURIES
Contusion
Nonpenetrating trauma results in a wide variety of tissue damage involving chamber angle deformities and injury to the retina, choroid, vitreous, and lens. The injury to the eye depends on the maximum force, the time to the maximum force, the area of contact, and the properties of the impacting object. The expansion of the eyeball perpendicular to the direction of impact has been proposed as the major cause of the contusion injuries that result from blunt trauma (Figs. 1 and 2). When a small, high-velocity object (such as a BB) hits the eye on the cornea, the entire eye deforms, and the weakest portion of the retina (upper nasal) often fails.47,86 When a large object (such as a soccer ball) hits the eye (especially in younger players where the orbital rims are less developed), more energy is directly transmitted to the exposed temporal retina while the nasal retina is protected by the nose. A suction component87 (Fig. 5, Table 7) most likely adds to the distortion of the globe anatomy that causes stresses resulting in tearing of structures in the anterior88 and posterior89 segments of the eye. This extreme distortion in the anatomy results in tearing of internal ocular structures (sphincter pupillae, peripheral edge of the iris, anterior ciliary body, attachment of the ciliary body to the scleral spur, trabecular meshwork, zonules, attachment of the retina to the ora serrata, and the Bruch membrane) that are resistant to stretching when the globe undergoes the deformations induced by the force of the impact.88,90 Because there frequently is a long interval between ocular contusion and the appearance of retinal detachment, and retinal breaks are formed at the time of injury, it is essential to examine the peripheral retina of all eyes that have had a contusion injury.91 Blunt trauma may cause transient high myopia by anterior shift of the lens-iris diaphragm and thickening of the crystalline lens.92 Hyphema may be caused by the shock wave of a pure blast injury.93
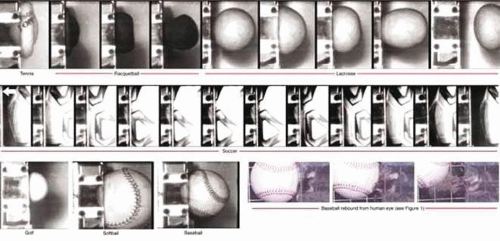 Figure 5. Orbital penetration and suction effect. The penetration, into an artificial orbit, of tennis ball, racquetball, lacrosse ball, golf ball, softball, baseball, and soccer ball. Adjacent frames are at intervals of 1 ms. The frames with the human ruptured eye are a continuation of the sequence depicted in Figure 1G–I. Note the suction effect of the ball on the ocular contents as the ball rebounds. (All balls traveling right to left except baseball impacting human cadaver eye, which is traveling left to right.) |
Table 7. Orbital Penetration and Penetration Duration (Orbital Contact) of Sports balls | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
A blow by a blunt object smaller than the orbital opening, such as a BB, paintball, golf ball, finger, or hockey stick, will transmit great forces to the globe. To produce eye injury, less energy is required with high-speed and small-mass missiles (BB shot) than with low-speed and large-mass missiles (soccer ball).
A blow by a blunt object larger than the bony opening, such as a tennis ball, elbow, or fist, has some of the energy absorbed by the surrounding bones, soft tissues, and orbital floor, which may fracture. There is a high incidence of internal ocular injury in these cases.94 The concept that an impacting object with radius of curvature greater than 2 inches (4-inch diameter) rarely causes eye injury because the ball delivers most of its energy to the orbital rims95 is incorrect. Large balls (such as soccer balls) and boxing gloves deform significantly on impact, allowing a small “knuckle” of the ball or glove, with a smaller radius of curvature, to enter the orbit and impact the globe. It is only by experiments using high-speed photography, coupled with injury data, that the true mechanism of injury can be elicited and appropriate protective devices designed.
Lamellar Laceration
The primary lamellar laceration potential from sports is the dislocation of a LASIK (laser-assisted in situ keratomileusis) flap. All patients who have had LASIK should be warned of this potential complication33,96,97,98,99,100 and be advised of appropriate protection, lest their flap be dislocated by a finger while playing basketball,101 or by a tree branch.102
INJURIES TO HIGHER VISUAL PATHWAYS
Blows to the skull with direct or indirect injury to the visual pathways may result in permanent or temporary visual loss.103,104,105,106,107,108,109,110 The huge forces required to produce these injuries can be encountered in many sports (e.g., collision sports, skiing, cycling, motor sports).111,112,113,114 With high-energy loads, eye protection must be considered as part of an integrated eye/face/head/brain protection system.
PRINCIPLES OF PREVENTING SPORTS-RELATED EYE INJURIES
There is a sequence of events that decreases the eye-injury risk of a sport to the individual player.
Those involved with a particular sport see various injuries and get an impression that the sport has a high risk of eye injury.
Data on the incidence and severity of injuries are collected to confirm or deny the initial clinical impression. This data collection may involve the establishment of special study groups and usually takes several years before the risk is confirmed or denied to the satisfaction of those involved with the sport.
If the initial impression is confirmed by the data, then a study of the sport and eye injury mechanisms (usually done simultaneously with no. 2) is conducted. This determines whether rules changes alone (e.g., eliminate fighting and high sticking in hockey) will reduce eye injuries to an acceptable level, or whether protective devices (e.g., hockey face shields) are necessary.
If protective devices are necessary, then performance standards must be written to ensure that the protective devices will meet the visual requirements of the game while reducing the probability of injury to a specified level.
In addition to the development of standards, certification councils must be established to ensure that protective devices sold to the athletes meet the standard requirements.
If needed, rules changes are implemented.
Data collection is continued to document the effect of rules changes and protective equipment on eye injuries and also the effect of the changes on injuries to other areas of the body. (For example, there was concern that the use of total head protective devices for hockey players might increase injuries to the neck. Extensive studies on change of center of head mass, skating attitudes,115,116 and analysis of all neck injuries to both protected and unprotected players have shown no increase of neck injury risk due to the protective device.117 However, the referees and coaches must enforce the rules of the game and not allow the level of violence to offset the effects of injury prevention programs.
Adjustments in rules/standards/protective devices are made as data collection shows the need for modification. It may turn out that serious injuries are impossible to prevent, since in protecting one area of the body injuries may be transferred to another. Then society must decide whether it is possible that the sport as it now exists presents too high a risk and should be banned. (For example, the once popular, but dangerous, sport of jousting would not be permitted a return, but what criteria should we use in deciding whether to ban an existing sport with significant risk to the athlete, such as boxing?)118
DISTRIBUTION OF FORCES
Forces are best dissipated if they are transmitted over a wide area and the duration of time over which the force is allowed to act is lengthened.119 If possible, the best area for distribution of forces when one tries to protect the eyes is the frontal bones. These bones are the sturdiest about the orbit and have the tendency to transmit energy into the mass of the face by the lateral orbital margins.120,121,122
Whenever a large force is transmitted anywhere on the head, the prime consideration must be the ultimate dissipation of this force as it relates to the brain. It is senseless to protect an eye if in so doing the damaging forces are transmitted directly to the brain. All protective devices for the head and face thus require two areas of consideration: First, is the primary area of concern (e.g., eye, face, teeth) protected? and second, is the transmission of forces such that there is no added risk to the brain? In collision sports such as hockey or football, this result is best achieved by mounting a face protector on a properly designed helmet. In this manner, the desirable goal of total head (not isolated eye, face, teeth, etc.) protection is achieved. Helmet design must be monitored by comparing predicted force116,119 with actual measurements of injury to real players in action.123
Sports with less energy potential require less protection. A squash ball has little potential for injuring the brain; therefore, attention need only be directed toward protecting the eye. In this case, one might consider it acceptable to transmit the forces to the frontal bone (best) or even less desirable areas (the bridge of the nose, the lateral or infraorbital rims) and still achieve good eye protection. One could accept a cut on the cheek, a broken nose, or even a fracture of the zygoma as far preferable to the potential loss of the eye.
EYEWEAR STANDARDS
The best sports standards are performance standards that specify how a protector must perform (e.g., visual fields, impact resistance, distribution of forces) rather than design standards that contain certain design elements that may or may not relate to performance. By and large, design standards are unnecessarily restrictive, tend to stifle the introduction of better, more innovative protector designs, and are more likely to encounter antitrust problems than performance standards.124
It is clear to those who write standards that one cannot tell how a protector will perform until it is tested under game conditions or conditions that approximate game conditions.125 If those who write standards and test protectors cannot tell how a protector will perform until the protector is tested, it is obvious that the untrained consumer will be unable to determine which products will provide adequate protection with minimal impact on performance by inspection in the retail shop. Severe eye injuries in sports can be prevented by writing performance standards that specify the protector’s energy attenuation and visual requirements followed by certification of the protective equipment produced by manufacturers.126 Sports regulatory bodies must mandate the use of equipment that passes the standard requirements, and governing bodies must legislate against uncertified products gaining access to the marketplace.127
Test requirements of relevant eyewear standards are listed in Table 8.
Table 8. Standards and Test Energies | ||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
ASTM International
Most sports eyewear standards writing in the United States comes under the jurisdiction of the American Society for Testing and Materials (ASTM). The largest of the approximately 400 standards-writing bodies in the United States, ASTM is neither a government nor a manufacturer’s organization but a nonprofit corporation organized in 1898 for development of voluntary standards arrived at by consensus, with strict guidelines for due process, among all interested parties.128,129
ASTM committee F-8 on sports safety standards and sports safety was formed in 1968 to address the sharp increase in head and neck injuries in football.130 ASTM F-8 now has subcommittees that write standards for many sports, including gymnastics, golf, archery, wrestling, fencing, trampolines, fitness products, racket sports, hockey, and baseball, as well as groups concerned with the more general problems of medical aspects and biomechanics, playing surfaces, headwear, footwear, padding, statistics, warning labels and signs, the female athlete, and eye safety.
Standards are designed to be revised as experience is gained. No matter how well the protector performs on paper or in the testing laboratory, it is only the use by thousands of players and continued injury monitoring that prove the protective value or demonstrate the failures of a particular design. For this reason, the ASTM mandates review of every published standard every 5 years. Other standards organizations (e.g., Canadian Standards Association [CSA],131 American National Standards Institute [ANSI], Deutsches Institut für Normung, International Organization for Standardization) operate under various bylaws.
At present, ASTM has completed the following standards for sports eye protectors:
ASTM F803 Eye protectors for selected sports (racket sports, women’s lacrosse, field hockey, baseball, basketball)
ASTM F513 Eye and face protective equipment for hockey players
ASTM F1587 Head and face protective equipment for ice hockey goaltenders
ASTM F1776 Eye protectors for use by players of paintball sports
ASTM F910 Faceguards for youth baseball
ASTM F2713 Standard specification for eye protectors for field hockey
ASTM F659 Standard specification for skier goggles and face shields
ASTM F2530 Standard specification for protective headgear with faceguard used in bull riding
ANSI
ANSI writes standards for protective eyewear in the United States with the exception of sports eyewear. It is the central body responsible for the identification of a single, consistent set of voluntary standards called American National Standards and is the U.S. member of international standards organizations. ANSI follows the principles of openness, due process, and a consensus of those directly and materially affected by the standards.
ANSI standards for eyewear are as follows:
ANSI Z80.5 Requirements for ophthalmic frames
ANSI Z80.1 Prescription ophthalmic lenses—recommendations
ANSI Z80.3 Requirements for nonprescription sunglasses and fashion eyewear
ANSI Z87.1 Practice for occupational eye and face protection
The ANSI Z80 standards are for dress eyewear, also called streetwear spectacles. The test requirements are minimal and geared to the desire for a diversity of styles in fashion eyewear. Streetwear spectacles are not appropriate for work or sports with impact potential. Impact-resistant polycarbonate or TriVex lenses should be used for dress eyewear. Streetwear frames are often fragile and have poor lens retention properties. Significant eye injuries have resulted from frame failure. Yet a streetwear frame with an impact-resistant polycarbonate or TriVex lens does give protection from low-impact injuries, such as a fishhook or a snapping twig.
The ANSI Z87.1 Industrial eye protectors are not satisfactory for sports for which there are ASTM standard specifications (Fig. 6). Yet ANSI Z87+ eyewear, designed to stop small high-velocity fragments, is an excellent choice for moderate-impact sunglasses and eyewear for shooting, fishing, cycling, and other activities that involve the potential of impact with a small fragment.
 Figure 6. ANSI Z87 spectacle failure with squash ball at 90 mph. |
Department of Defense
Military eyewear will be coordinated under a single umbrella program called the Military Eye Protection System (MEPS; http://www.dod.mil/) in which testing is done with fragment-simulating (T-37) projectiles (Fig. 7), either 0.22 caliber, 17 grain (1.1 g) at 168 m/s (550 ft/s) or 0.15 caliber, 5.8 grain (376 mg) at 195 m/s (640 ft/s). Sun, wind, and dust goggles (MIL-V-43511); ballistic/laser protective spectacles (MIL-PRF-44366B); and special protective eyewear, cylindrical system with interchangeable lenses (MIL-PRF-31013) standards ensure eye protection from most fragments anticipated in military combat. Although this eyewear has not been tested for sports use, it would provide excellent protection for the hunting and shooting sports but not for sports for which specific ASTM standards apply (such as paintball, hockey, and sports covered under ASTM F803.)
 Figure 7. Military fragment simulators and ANSI high-velocity test object. Left. military 0.15 caliber. Center. military 0.22 caliber. Right. ANSI 1/4″ steel ball. |
NOCSAE
The National Operating Committee on Standards for Athletic Equipment (NOCSAE; http://www.nocsae.org) has standards for baseball, football, and lacrosse helmets; baseballs and softballs; and face shields for football and men’s lacrosse.
Current NOCSAE standards include the following:
Standard Drop Test Method and Equipment Used in Evaluating the Performance Characteristics of Protective Headgear. NOCSAE Doc. 001-00m02
Standard Performance Specification for Newly Manufactured Football Helmets. NOCSAE Doc. 002-96m98
Standard Performance Specification for Recertified Football Helmets. NOCSAE Doc. 004-96m98
Standard Projectile Impact Testing Method and Equipment Used in Evaluating the Performance Characteristics of Protective Headgear, Faceguards, or Projectiles. NOCSAE Doc. 021-98m02
Standard Performance Specification for Newly Manufactured Baseball/Softball Batter’s Helmets. NOCSAE Doc. 022-98m02
Standard Performance Specification for Newly Manufactured Baseball/Softball Catcher’s Helmets with Faceguards. NOCSAE Doc. 024-98m02
Laboratory Procedural Guide for Certifying Newly Manufactured Football Helmets. NOCSAE Doc. 003-96m02
Laboratory Procedural Guide for Recertifying Football Helmets. NOCSAE Doc. 005-96m02
Laboratory Procedural Guide for Certifying Newly Manufactured Baseball/Softball Catcher’s Helmets with Faceguards. NOCSAE Doc. 025-98m02
Troubleshooting Guide for Test Equipment and Impact Testing. NOCSAE Doc. 100-96m97
Equipment Calibration Procedures. NOCSAE Doc. 101-00m02
HEADFORMS
Headforms are necessary for testing and development. Headforms may be impacted without injury and give consistent results. Choosing the proper headform is essential to any protector design or testing. The anthropomorphic features, hardness, and energy-absorbing characteristics all affect test results. Comparison of the results on the test headform with those actually achieved on the human head are essentia1.132,133 The Canadian headforms, which are based on actual physical and radiologic measurements of thousands of heads,134 are better proportioned for eyewear testing and design than the commonly used U.S. headforms (Alderson 5, 50, and 95 percentile), which are based on projections made from measuring a sample of military men. NOCSAE revised its test forms with anthropomorphic measurements based on CSA data.
Equipment Certification Councils
Some manufacturers lie and falsely advertise that products pass a standard, when in fact they do not. Major manufacturers of industrial135 and sports eyewear fall into this category. Sports protectors, certified by the manufacturer to meet the standard specifications of ASTM F803 (in advertising, with hangtags, and labeling on the packaging), have not met the standard specifications when I and others have tested them, and one that failed resulted in significant injury to a racquetball player. In the United States, manufacturers made certain that the ANSI Z87 industrial standard allows the manufacturer alone to certify that their products conform to the standard specifications. In Canada, the CSA acts as both the standards writer and the certifying agency for industrial and sports protectors—a far better system for the safety of the users.
It is only certification, or documented testing by a certified test laboratory, that gives the user the assurance that the protector will afford reasonable protection. A sports equipment certification council is composed of coaches, participants, scientists, physicians, manufacturers, and administrators. Its purpose is to seek out and select codes and standards, including test methods and procedures, for equipment used in athletic, sporting, recreational, and leisure time activity. In addition, the council identifies and publishes all factors associated with safety, whether it be protective equipment, playing surfaces, rules, attitudes, officiating, training, conditioning, or administration.136 The Council will usually have a seal (Fig. 8) that manufacturers affix to a protective device that is assurance to the consumer that a product meets the specifications of a performance standard (Fig. 9).
 Figure 8. Certification seals. |
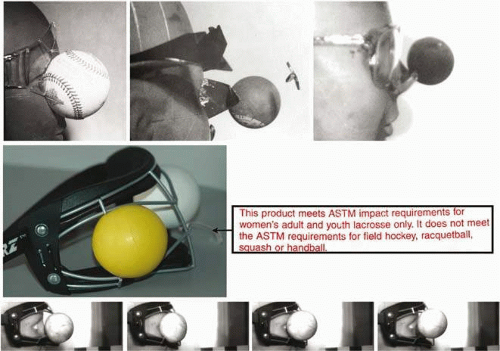 Figure 9. Buyer beware of uncertified products, advertised for sports, that do not protect. Each of these products was advertised as a protective device for the sports depicted (baseball, squash, women’s lacrosse). None of the major U.S. distributors of these products would produce evidence that the product was tested by an independent laboratory, but gave assurance that “rigid tests” were done by the manufacturer. Each product failed when tested to ASTM F803 for the advertised sport. None of the manufacturers recalled their product when informed of the test results. The women’s lacrosse “protector” (row 2) allowed lacrosse balls through right and left eye openings with little finger pressure, despite the centrally placed hang tag with the false claim of compliance to the standard specifications of ASTM for women’s lacrosse. When actually tested to the standard, motion analysis revealed severe eye contact with the lacrosse ball (row 3). |
HECC
The Hockey Equipment Certification Council (http://www.hecc.net) is an independent, nonprofit organization that was established in 1978 through the joint efforts of the Amateur Hockey Association of the United States and a number of interested volunteers. HECC certifies ice hockey equipment, including helmets and face shields; selects codes and standards to certify playing equipment and facilities; monitors the effectiveness of its certification program; and promotes research pertaining to the prevention and reduction of ice hockey injuries. HECC is extremely effective in fulfilling its mandate of reducing injuries in hockey.
PECC
The Protective Eyewear Certification Council is unfortunately not operating at this time (May 2010). When it was operational, PECC certified protectors complying with ASTM standards (except for ice hockey). Since the infrastructure is in place, it should be easy to get up and running—if the manufacturers and sports officials will cooperate and support the program.
CSA
The Canadian Standards Association (http://www.csa.ca) certifies products complying with the Canadian racquet sport and ice hockey standards, which are similar to the ASTM standards.
Certified Testing Laboratories
Although not true certification councils, certified testing laboratories are a good option for eye care professionals, sports officials, and users to be certain the protector meets standard requirements. A testing laboratory must be able to provide evidence of the successful completion of the American Association for Laboratory Accreditation (A2LA; http://www.a2la2.net/) evaluation process to perform the tests that are specified in the standards. A manufacturer should be able to supply a test report from an A2LA-certified laboratory on request from a potential user of their product.
OBSOLESCENCE IN PROTECTIVE EQUIPMENT
Protective equipment is obsolete when it no longer provides adequate protection, cannot be purchased under normal circumstances, is no longer in the desired style, is unreconditioned “hand me down” equipment, or is worn out, broken, or ill-fitting.136 As injury data result in standard modification, certification councils must publish a list of equipment that has become obsolete by newer advances, and this obsolete equipment must be discarded.
GUIDELINES FOR SPORTS PARTICIPATION
The American Academy of Pediatrics classifies sports into three main categories (contact/collision, limited contact/impact, and noncontact)137,138,139 and suggests that some sports are contraindicated for the one-eyed participant. The traditional contraindications to athletic participation are more appropriate to the systemic, musculoskeletal, cardiac, respiratory, paired-organ, and central nervous systems than to the eye. Whereas musculoskeletal injuries and cerebral concussions are inevitable in contact/collision sports (such as rodeo) and are rare in noncontact sports (such as golf), eye injuries may be more common and severe in the “safer” sport. The recommendations of the American Academy of Pediatrics may be considered overrestrictive as society becomes more aware of the civil rights of athletes and the need to allow the disabled to participate in sports.140,141,142 It is apparent that more realistic guidelines for participation in sports by persons with various ocular disabilities and ocular diseases could be devised. Although such a list is dependent on reliable injury data that are not available at this time, there was sufficient information for the International Federation of Sports Medicine to release a position statement on eye injuries and eye protection in sports, which should help reduce eye injuries worldwide.143
THE ONE-EYED ATHLETE
Severe eye injury to a child can result in posttraumatic stress disorder, even if the vision is restored to reasonable levels after surgery.144 The emotional, psychological, and legal impacts of severe eye injuries are often neglected, but attention to them is essential in the management of all patients who have suffered severe injury—especially that involving the loss of an eye.145 The risk of becoming blind is markedly higher for the amblyopic patient (1.75 ± 0.30 per 1,000) than for the general population (0.11 per 1,000 for children, 0.66 per 1,000 for adults). Trauma (work, sports, violence, accidents) causes more than 50% of the resultant blindness.146
How can we define one-eyed? For the purpose of recommending extra safety precautions, a person is functionally one-eyed when loss of the better eye would result in a significant change in lifestyle owing to the poor vision in the remaining eye.147 A person certainly should be considered functionally one-eyed if his or her best-corrected vision in the involved eye is 20/200 or less, with the other eye found normal by an ophthalmologist. On the other hand, most of us would function fairly well with 20/40 or better vision in the remaining eye. More difficult is advising patients with between 20/40 and 20/200 best-corrected vision in the affected eye. The loss of the ability to drive a vehicle legally in most states would be a handicap to most persons. The inability to drive would significantly interfere with the jobs available to a youngster when he or she is older, and studies would be more difficult throughout the school years. Therefore, a child should be considered functionally one-eyed when the best corrected vision in the poorer eye is less than 20/40, and an adult is functionally one-eyed if he or she believes the level of vision in the poorer eye would interfere with life or livelihood if the better eye were lost.148 Functionally one-eyed athletes (and their parents in the case of minors) must be well informed of the potential long-term consequences if the better eye were lost. They should also be informed of the risks of injury (without and with various eye protectors) and the possibility of repair of injuries typically seen with the sport in question.
It is only by full discussion of the potential serious long-term consequences of injury to the better eye that the ophthalmologist, the athlete, and the parents can agree on the wisdom of participation in a particular sport as well as the level of protection necessary for the better eye. The most effective protection is possible only when the athlete understands the risks and is anxious to cooperate in the effort to protect the eyes while still allowing participation and enjoyment of the preferred sport. Having the athlete wear an occluder over the better eye for several days will allow him or her to better evaluate the ability to function with the poorer eye. Usually, if the athlete is sincere and honest with himself or herself, it is fairly easy to reach agreement among the athlete, parents, ophthalmologist, and sports officials as to whether the athlete is functionally one-eyed.
As protective devices improve and effective sports eye protectors are developed, more and more sports become quite safe even for the one-eyed athlete.149 The division of sports into contact/collision (boxing, field hockey, football, ice hockey, lacrosse, martial arts, rodeo, soccer, wrestling); limited contact/impact (baseball, basketball, bicycling, diving, high jump, pole vault, gymnastics, horseback riding, ice and roller skating; cross country, downhill, and water skiing; softball, squash, handball, volleyball); strenuous noncontact (aerobic dancing, crew, fencing, discus, javelin, shot put, running, swimming, tennis, track, weight lifting); moderately strenuous noncontact (badminton, curling, table tennis); and nonstrenuous noncontact (archery, golf, riflery)150 tells little of the risk of eye injury. From an eye injury perspective, it is far more dangerous to play badminton (moderately strenuous noncontact) without an eye protector than to play ice hockey (contact/collision) with a full-face mask.
Any banning of athletic participation in certain sports should be based on guidelines using an experiential framework rather than tradition or anecdote.151 The athlete deserves a true discussion of the risk of eye injury involved in a chosen sport. The outright ban, by some schools, of the one-eyed from participation in collision and contact sports, while the one-eyed students are permitted to play more dangerous (to the remaining eye) sports, such as tennis, is not prudent and should be re-evaluated. Unless the athlete is especially gifted in a particular sport, or has psychological reasons to participate in a chosen sport, a safer sport (e.g., track and field, gymnastics) should be encouraged and will usually be chosen. The American Academy of Pediatrics recommendations now take into account that with adequate protection, the one-eyed individual may participate in most sports.150 The medical/school committee should specify that the one-eyed athlete follow the safety guidelines presented in this text or modified in the future.
At this time, the only sports absolutely contraindicated for the functionally one-eyed are boxing and full-contact martial arts, since the risk of serious injury is very high and there is no known effective eye protector. Wrestling and the noncontact martial arts, while they have a lower incidence of eye injury, also do not have effective eye protection available and should be strongly discouraged for the functionally one-eyed and banned for the monocular athlete. If the player, parents, and possibly their lawyers are persistent and insistent after an informative discussion, they should be required to sign appropriate waivers as dictated by the school committee. The waiver has a dual purpose: It helps ensure that the athlete will wear appropriate protective devices for practices and games, and it often affords the only possible legal protection for school committees and members of sports-medical committees faced with the dilemma of the one-eyed athlete who insists (or whose parents insist) he or she play a sport with high risk of eye injury, such as wrestling, for which there is no adequate known protection. The best medical advice says that the functionally one-eyed athlete should not, but it seems that there may be confusion in the law.152 The Massachusetts law reads, “the health and safety of each student must be paramount in every phase of the instructional physical education program,” and also “each school shall provide equal opportunity for physical education for all students.”153 Federal law states, “students who can participate in regular physical education programs for all or some aspects of physical education must be placed in such programs.”154 The physician becomes hard put to prove that he or she is not discriminating against the disabled by excluding the one-eyed student from some sports.155
From a performance standpoint, the one-eyed can usually function quite well in most sports, adding very little risk to cause other injuries because of the monocular condition. Ocularists (makers of prosthetic eyes), who deal with many one-eyed people, are aware of this fact;156 however, ocularists should also have expertise in available eye protection and give appropriate recommendations to the patient. The reinforcement of the protective message is very important. If the athlete is informed of the need for protection, and also given specific advice by the ophthalmologist, optometrist, optician,157 and ocularist, there is a far greater likelihood of protection compliance.
PROTECTIVE DEVICES
Fortunately, most sports-related eye injuries are preventable with properly designed equipment. The following is a practical guide for sports eye protection so that persons whose responsibilities involve the eye in athletics can easily determine the protective equipment they should recommend or provide.158 A protective device should prevent damaging forces from reaching the eyes by dissipating potentially harmful forces over time and area. This theory is simple enough, but the practical application can be difficult. As soon as design is begun on a protective device for a sport with an ocular hazard, many problems arise. What forces are involved in this sport? Are they high-velocity, low-mass (hockey puck); low-velocity, high-mass (player sliding into a goal post); or a combination of high-velocity and high-mass (bicycle racer collision)? Does a protector have to be designed differently for each type of force? How? Where on the head will the forces be transmitted, and how will it be done? Will the player be killed or suffer brain damage if the force is transmitted to his or her brain through the protective device, rather than being dissipated into broken facial or orbital bones as was the case before the protector? Will the protector change the form or appeal of the game? What about the design, player acceptance, expense, weight, interference with vision, product liability, and full disclosure to the consumer?
These questions cannot be answered by any one individual, since expertise at many levels and different areas of interest is required. The best way to design and build a protective device is by the development of a performance standard as discussed previously.
Various kinds of eye protection and different brands of sports goggles vary significantly in the way they fit. An experienced ophthalmologist, optometrist, optician, or athletic trainer can help an athlete select appropriate protective gear that fits well and looks good. The best-designed protective device, if it does not appeal to the tastes of the player, will remain on the dealer’s shelf. Sports programs should assist indigent athletes in the evaluation process and in obtaining protective eyewear.
Criteria for Protective Eyewear
Proper fit is essential. Protective eyewear will be worn only if it is comfortable and allows good vision. Helmets should have a properly fastened chinstrap for optimal protection. The athlete should be fit with a protector that feels comfortable and fits snugly. A good test for a snug fit is to lightly run a finger around the perimeter of the eye protector. There should be no gaps large enough to permit the finger to lightly touch the eye. The user should compare several protectors for comfort, vision, and fit. Antifog treatment is often factory applied or may be applied by the user.
Protectors with clear lenses (plano or prescription) should have impact-resistant polycarbonate or TriVex lenses. If for some reason polycarbonate or TriVex lenses cannot be used, the athlete who participates in an eye-risk sport should either
wear contact lenses plus an appropriate protector as listed in Table 9 and Figure 10, or wear an over-the-glasses eye guard that conforms to the specifications of ASTM F803 for sports for which an ASTM F803 protector is recommended.
For sports requiring a face mask or helmet with an eye protector or shield, functionally one-eyed athletes should also wear sports eye protectors that conform to the requirements of any sport specified in ASTM F803 to maintain some level of protection if the faceguard is elevated or removed (as in ice hockey or football by some players on the bench).
Contact lenses offer no protection. Therefore athletes who wear contact lenses must also wear appropriate eye protection.
Athletes must replace sports eye protectors that are damaged or yellowed with age, because they may have become weakened.
 Figure 10. Safety recommendations. 1. Eyewear should be fabricated with highly shatter-resistant polycarbonate or TriVex lenses unless there is a specific reason for another lens material. Children, functionally one-eyed people, and active adults require polycarbonate or TriVex lenses. 2. For sports that have the potential for eye contact, use eyewear that is certified to ASTM F803 (racquet sports, women’s lacrosse, baseball, and basketball) or ASTM F2713 (field hockey). For other sports, such as soccer, protectors should meet or exceed ASTM F803 standard specifications for squash. Prescription sports eyewear requires 3-mm-thick polycarbonate lenses. 3. Sports with high impact, such as ice hockey, men’s lacrosse, and youth baseball (batter/base-runner) require a face shield mounted on a helmet designed for the sport. Paintball protectors must conform to the requirements of ASTM F1776. 4. People working with exposure to flying chips or with power tools should use protectors that meet ANSI Z87.1 specifications. Goggles are the safest. Only polycarbonate or TriVex lenses should be used. 5. Many workplace activities, such as using a chain saw, require, in addition to safety glasses or goggles, a helmet with a face shield designed for the activity. 6. Sunglasses should conform to the previous safety recommendations. Sunglass lenses should attenuate blue light, which is potentially hazardous to the macula. Gray, amber, or brown lenses are preferred. Blue-colored sunglass lenses that transmit blue light should not be used. |
Table 9. Recommended Eye Protectors for Selected Sports | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Classification of Sports Eyewear
Sports have very different eye, face, and head–brain risk, and thus require specifically designed protective equipment, The equipment can be classified into the following:
A helmet with an integral face protector for sports that combine very high energy with a significant potential for eye contact (football, men’s lacrosse, youth baseball batter/base runner, baseball catcher, polo, ice hockey, automobile and motorcycle racing, downhill ski racing).
A helmet with separate eyewear for sports with a significant brain injury potential, but less potential eye contact (riding a bicycle, horse, or motorcycle). Note: Many motorcycle and some bicycle activities require a helmet with an integral face protector.
A face-supported protector for sports that have significant eye and face danger but less potential for brain injury (paintball, fencing, baseball behind-the-plate umpire).
An eye protector that conforms to the requirements of ASTM F803 for sports that pose mainly an eye injury risk (racket sports, basketball, women’s lacrosse, field hockey, baseball fielders). It is recognized that baseball, women’s lacrosse, and field hockey also have head and face injury potential, but, other than the helmet-mounted face protectors for youth baseball batters, base-runners, and catchers, full face protection has not been accepted by most players and sports officials of these sports.
Eyewear that conforms to the military fragment or the high velocity ANSI Z87 test requirements for the shooting sports.
Fashion eyewear when there is negligible eye injury risk. There are several types of clear material (glass, allyl resin, high-index plastic, acrylic, polycarbonate, and TriVex) from which prescription or nonprescription (plano) lenses may be fabricated. Polycarbonate and TriVex are the most shatter-resistant lens materials and are recommended for all eyewear.
Sunglasses for Sports
The improper choice of sports sunglasses may be hazardous and degrade visual performance.159 Both visible and ultraviolet light can result in eye injury, which may be minimized with the use of appropriate sunglasses. It is controversial whether or not short-wavelength visible (<510 nm, blue) light increases the tendency to macular degeneration, but there is evidence that chronic exposure to sunlight is associated with the development of early age-related maculopathy.160,161,162,163 Exposure to ultraviolet light causes cataracts,164,165,166,167,168 corneal changes (climatic droplet keratopathy, pinguecula, pterygium, and acute photokeratitis),169—171 uveal melanoma,172,173 premature skin aging and sunburn,174 and skin cancers (basal cell carcinoma, squamous cell carcinoma, melanoma)173,175 Even relatively brief exposure to viewing the sun when high in the sky (zenith greater than 60%) may result in solar retinitis due to photochemical injury from intense short-wavelength (blue) and ultraviolet (UV) radiation.176,177,178 Many clinicians have the impression that herpes simplex keratitis and recurrent corneal erosion may be precipitated by exposure to sunlight.
Reflected UV light also must be considered. Fresh snow reflects about 80%, older snow more than 50%, clean white sand about 30%, water 5%, and earth and grass less than 5% of the ambient ultraviolet light. Thus the greatest UV light exposure occurs at high altitude on a field of fresh snow. Mountaineers, skiers, sailors, and lifeguards are exposed to large doses of visible and ultraviolet light, at times in situations in which there is the potential for injury from impact, in adverse conditions of high wind or dust. The inability to see well because of photokeratitis, windburn, corneal foreign bodies, or traumatic injury from shattered spectacles may be life threatening as well as eye threatening; therefore the proper choice of sunglasses is essential. Dark sunglasses permit one to be comfortable in bright light without squinting. However, one must be certain that the glasses have adequate absorption in the toxic UV and blue light ranges.179 Wearers and those observing them should be aware that the reflection from the front surface of mirrored sunglasses may result in severe sunburn to the nose unless extra protection is used.180
Sunglasses are especially important for those who have had cataract surgery. Removal of the lens of the eye exposes the retina to wavelengths greater than approximately 300 nm. In the 325- and 350-nm UV radiation range, the retina is approximately six times more sensitive to damage than to short-wavelength visible radiation of 441 nm. Since untreated polymethyl methacrylate intraocular lenses (IOL) absorb UV radiation only less than 300 to 320 nm,160 many intraocular lenses, classified as UV protective, offer less than optimal protection,181 and because it is not known how long the UV filter on UV-absorbing IOLs lasts, it is prudent for all aphakic or pseudophakic athletes to wear sunglasses that absorb 99% of light less than 470 to 500 nm.
Athletes who want maximum UV light protection should wear a hat with a brim, which reduces ocular exposure by half,182 and close-fitting sunglasses that absorb UV when in conditions in which athletes could get sunburned.183 There is considerable variability in the quality of sunglasses184 that is of concern in children’s sunglasses185 since children frequently spend more time in the sun. Damage to the lens (and possibly retina) from UV is cumulative, and the crystalline lens of children transmits more short-wavelength visible radiation and UV light to the retina than does that of the adult.160
Even with darkly tinted glasses, there is no way to predict by gross visual inspection which lenses effectively filter reasonable quantities of the near infrared light (700–800 nm) and near UV light (300–400 nm) that are not visible to the human eye. Cost, color, and lens composition are unreliable indicators of adequate filtration. In one study, 53% of glass and 11% of plastic lenses had an unfavorably high near UV light transmission peak greater than 25%.186 Eighty percent of the amount of infrared light present in daylight is transmitted to the retina. Although the infrared light present in daylight is not toxic in itself, some believe that infrared light may contribute to damage from UV light and lower wavelengths and may contribute to ocular discomfort of fatigue. Since infrared light contains no useful visual information, it is probably wise to filter it out.160 UV light absorption is quite different for various lens materials.187
The vast majority of sunglasses sold for sports use are deficient in impact resistance. A sports sunglass should prevent rather than contribute to injury. The combination of lens and frame must prevent ocular contact by either the missile or the sunglass lens. Manufacturers should state the sports for which the sunglass is intended. Safety requirements are the same as for protective eyewear with clear lenses. Manufacturers should be required to provide the following information, in a statement easily understood by the consumer, on all sunglasses sold for use in sports: the standard specifications to which the sunglass conforms, the percent of visible light transmitted through the lens, the percent of UV light and infrared light (wavelengths specifically stated) transmitted through the lens, and additional treatments or coatings (for example, polarization) to reduce glare.
The ideal sports sunglass should have the following characteristics:
UVB (280–315 nm)—less than 5% transmittance; less than I% transmittance for wavelengths less than 310 nm.
UVA (315–400 nm)—less than 10% transmittance, and absolutely less than maximal visible light transmittance; for aphakic athletes, less than 1% transmittance.
Blue light (400–500 nm)—less than 10% transmittance and absolutely less than the maximal visible light transmittance. A blue light transmittance of 25% to 50% of the peak visible transmittance would be desirable.
Long-wavelength visible light (500–760 nm)—less than 15% transmittance for bright conditions, such as sand or snow.
Infrared (above 760 nm)—filtration desirable but not essential.
Allow color discrimination sufficient to recognize traffic signals.
Have side shields and either a rim across the top or be used in conjunction with a brimmed hat to protect against oblique incident radiation in very bright conditions.
Have the option of polarization to decrease glare from water for those fishing and boating.
Have aerodynamic efficiency to combat the drying effects of wind in speed and wind sports (e.g., cycling, yachting, mountaineering, skiing).
Be lightweight. Heavy sunglasses will tend to fly off the face with rapid changes in head position.
Have cosmetic acceptability.
Be impact resistant, consistent with the intended use.
HOW DO I KNOW WHAT TO BUY, PRESCRIBE, OR DISPENSE?
It could be disastrous to buy, prescribe, or dispense what you believed was protective eyewear and then have the eyewear fail. Compounding the problem is the fact that some manufacturers make “sports” eyewear that does not conform to safety standards (Fig. 9), and that most ophthalmologists and consumers do not know what protection standard should apply for a specific activity.
The safest way to choose an eye protector is to look for a certification seal (Fig. 8) to ensure that the protector has been tested by an accredited laboratory to a specific safety standard.
The spectacle prescription will be clear to the optician if the note “Polycarbonate or TriVex lenses are required for children, functionally one-eyed people, and active adults” is printed on the front of the prescription.
Although a fashion eyewear frame has little impact resistance, it is far better to have a lens that is shatter resistant in front of the eye than risk a lacerated globe from a shattered lens. It is almost certain that the eye care professional who dispenses or prescribes a spectacle lens that shatters easily will be sued if the shattered lens results in significant injury. Therefore it is prudent to prescribe, dispense, and wear eyewear with extremely shatter-resistant polycarbonate or TriVex lenses. To test the strength of these lenses, try to break them with a hammer.
Safety Recommendations on Rx Pad
Recommendations, printed on the reverse side of all spectacle prescriptions, should help the patient choose appropriate protective eyewear (Fig. 11).
 Figure 11. A summary of protective eyewear. ANSI Z80 Fashion eyewear. Use only with polycarbonate or TriVex lenses. OK for eye-safe sports and dress eyewear. ANSI Z87 Industrial eyewear and sports eyewear that passes the Z87 high velocity test must bear the Z87+ mark. Goggles are safer than spectacles when there is the potential for flying particles (grinding) or for use with chemicals. Z87+. Spectacles or goggles are always worn under a face shield, when a face shield is required for safety. These protectors are satisfactory for sports with no ASTM standards, such as Frisbee or cycling, and are a good choice for daily-wear sunglasses, never for paintball. Military eyewear and industrial or sports eyewear that passes the military fragment high velocity test. Military eyewear is not available to the general public, but other eyewear that passes military tests is good for shooting and hunting. Eyewear certified to ASTM F803 or F2713. Must be certified by an A2LA accredited laboratory for the specific sport. Necessary for sports covered by ASTM F803 (racket sports, women’s lacrosse, basketball, baseball) or ASTM F2713 (field hockey). ASTM F803 protectors are adequate for soccer. Available for prescription eyewear (upper left) for use over Z80 eyewear (upper right), as a polycarbonate eye shield (top center) or wire (bottom center), and as a plano spectacle with interchangeable lenses (clear, yellow, and gray) for sunglass use. |
Contact Lenses
Because contact lenses offer no protection from impact, it must be stressed to patients that protective devices, where indicated, should be worn in addition to the contact lenses. Patients who request contact lenses for sports use deserve a few minutes of discussion of injury prevention.188
Despite the fact that contrast sensitivity may be decreased with daily wear soft lenses,189 contact lenses, especially for people with large prescriptions, do offer advantages for many sports—better visual field, no fogging, and staying in place with rapid motion. Lens technologies that combine the excellent visual acuity of rigid gas-permeable contact lenses with the comfort and retention characteristics of soft lenses are preferred by many athletes, especially those with astigmatism.190 Large-diameter (15.5 mm) and scleral (18–24 mm) soft lenses are available for athletes who cannot wear standard soft or rigid gas-permeable lenses because of decentration with sports activity.191,192,193
Many sports are played in environments that make contact lens wear more difficult because of increased exposure to water, wind, sun, dust, and dirt. The use of wraparound polycarbonate sunglasses over the contact lenses frequently allows the mountain bicycle racer to have the benefits of contact lens vision in the face of wind and debris. For sports, such as ice hockey, in which low humidity may be encountered, low-water, low-soiling, low-dehydrating, larger-diameter, thin, soft contact lenses seem to give satisfactory results.194 Wind, dry air, UV light, and decreased oxygen at high altitude often cause punctate keratitis in skiers and mountaineers.195,196,197 Skiers who wear contact lenses should be encouraged to wear goggles that absorb UV light and break the wind. If contact lens wear becomes impossible, spectacles could save an otherwise ruined vacation.
RISK OF EYE INJURY AND EFFECTIVENESS OF PROTECTIVE DEVICES FOR SPECIFIC SPORTS
In this section, sports are arranged roughly according to the size of the potential impacting object. Data estimating the participant demographics in selected sports activities have been gathered by the Sporting Goods Manufacturers Association (SGMA)34 (Table 10).
Table 10. Comparison of Injuries from BB Gun by Type of Gun and Muzzle Velocity | ||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||
Small, Penetrating Projectiles
Penetrating projectiles, mostly shrapnel, shotgun pellets, BBs and air rifle pellets, fishhooks, and shattered eyewear lenses, have the highest ratio of eyes lost to injured eyes, yet these injuries are relatively easy to prevent. Streetwear spectacles with polycarbonate or TriVex lenses would stop most fishhooks. Plano industrial ANSI Z87+ eyewear gives adequate protection from BB and air gun pellets. Military eye armor will stop most small land-mine and small artillery fragments. Industrial eyewear that passes military standard specifications will stop most shotgun pellets.
BBs and Air Rifles
Considering that competitive air gun shooting is a safe sporting activity, with no reported injuries to any competitor, it is reasonable to conclude that injuries related to BB guns and air guns are secondary to inappropriate and unsafe use of the equipment. If BB guns and air guns are viewed in their proper role as sports equipment, and used safely with appropriate supervision, the injury problem can virtually be eliminated.
There are no reliable participation data for non–target-shooting air rifle and BB guns, but there are many air guns in circulation. In the Chicago area, 6% of families that included at least one 3-year-old child and 11% of families with a boy between the ages of 10 and 14 years owned an air gun.198
Yet, eye injuries related to the shooting of BB guns and air guns have been a source of concern and frustration for ophthalmologists. Despite the recommendations of Canadian ophthalmologists, nonpowdered firearms were excluded from the Canadian Firearms Act of 1995—and still had not been included in 2003.199,200 BB or pellet guns are responsible for 5.13% of all injuries in the USEIR database.201 There is no information as to the injury incidence. What is known is the following: Approximately 3 million air guns were sold in the United States in 1980; there are about 31,500 BB/pellet-gun-related injuries every year, of which about 2,000 require hospitalization; and 80% of the injuries occur in the 5- to 14-year age group.202 Unsupervised access to air guns and unstructured gun use are the principal risk factors for ocular injury. The victims were most likely to have been shot unintentionally by a male friend at the friend’s home, using the gun for a purpose other than target practice, using it without adult supervision.203,204
Gas-propelled guns have three primary methods of propelling the projectile: (i) A spring-piston air gun, when cocked, draws air into a cylinder and tensions a spring, When the trigger is pulled, the spring pushes the piston forward, compressing the air that fires the projectile at muzzle velocities up to 600 ft/s. (ii) Pneumatic air guns compress air that is released when a valve is opened on trigger depression. The multiple pump compression system, introduced in 1972, achieves the highest velocities—more than 900 ft/s. (iii) Compressed-CO2 guns have typical muzzle velocities in the 400 to 500 ft/s range.202,205,206 The velocity loss of a BB over a typical 20-foot firing distance is negligible. A BB starting at 260 ft/s loses only about 1 ft/s velocity per foot of distance traveled.207 The original, inefficient toy BB guns with smooth barrels that were larger than the missile have been replaced with air guns with rifled barrels, tight-fitting missiles, and pneumatic chambers that can be pumped to dangerously high levels. Technology has converted a toy into a potential weapon with the ability to kill.205,208
Despite advances in surgical technique,209 most eyes perforated with pellets or BBs suffer permanent visual loss, with many resulting in enucleation.204,210,211,212,213 Most (77%) of the patients are in the 7- to 14-year age group, and almost all the others in the slightly older 15- to 24-year age range. Forty percent of injured eyes become legally blind, and 12.5% to 18% are enucleated as a result of the injury, which most commonly occurs at Christmastime to unsupervised children, often from ricochets from improper (hard) target backstops. Complete blindness may occur from sympathetic ophthalmia affecting the uninjured eye.214,215,216
Injuries secondary to BB guns and air guns were the principal diagnosis in 16.6% (4,982 cases) of eye injuries resulting in hospitalization in the United States between 1984 and 1987.217 BBs caused 8 of 48 perforating (through and through) injuries to the globe. The fact that BB perforating injuries have a poor prognosis is due to the tremendous force transmitted to the globe as it creates two blunt openings approximately 5 mm in diameter (Fig. 12).218 BBs were responsible for 16 of 222 ocular injury cases in patients admitted to a children’s hospital. Six of the 16 resulted in blindness in the injured eye.219 Twenty-three of 278 childhood traumatic eye injuries admitted to Wills Eye Hospital were the result of BBs.21
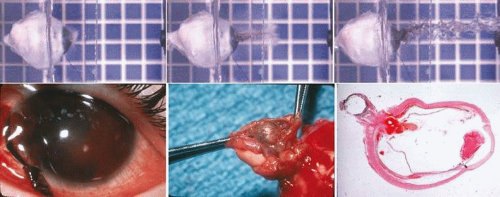 Figure 12. BB perforation of human eyes. Top. BB perforation of human cadaver eye. Continuation of Figure 1A–C. BB moving right to left at 92.0 m/s (301.8 ft/s; 0.58 J). Note continued extrusion of intraocular contents after BB has passed through posterior sclera. (Courtesy of Stefan Duma and Joel Stitzel. Virginia Tech Impact Biomechanics Laboratory [duma@vt.edu].) Bottom. BB perforation of a child’s eye through lamina cribrosa into optic nerve sheath. (Courtesy Ann Bajart.) |
BB guns and air guns are not given the respect they deserve as potential weapons with blinding and killing power.211,220,221 In 2001, NEISS estimated that 29,617 injuries from gas, air, and spring-operated guns were seen in U.S. emergency departments, of which 2,994 involved the eye. Of the total injuries, about two thirds were to children aged 14 years or younger, and about one third of the eye injuries required hospitalization.31 Patients who require hospitalization and surgical intervention from BB eye injuries have a high risk of enucleation.213 Of 32 patients treated with surgical intervention at the Wilmer Eye Institute between 1970 and 1981, 22 had penetrating injuries from the pellets, 19 had their penetrated eyes enucleated, and the remaining three had vision worse than 5/200.222 Of the 80 eyes removed due to sports-related injuries at the Massachusetts Eye and Ear Infirmary between 1960 and 1980, 36 were due to injuries from BB guns.223
A standard BB (0.345 g) will penetrate the globe at speeds greater than 236 ft/s (72,0 m/s) and result in injury at the vitreous base at an average speed of 205 ft/s (62.3 m/s).47 Round, smooth, relatively lightweight BBs are prone to embolize if they enter the vascular system, with potentially severe visual and systemic results.202,206,224 Higher-powered general-purpose air rifles, advertised in children’s magazines, may have muzzle velocities as high as 620 ft/s (189 m/s), which is well above the 408 ft/s (124 m/s) velocity required “for penetration of skin, bone, and moderate tissue, or if no bone is encountered, of skin and deep tissue.”
Since BB guns cannot be made safe and still have any utility, the only means of controlling injuries is to keep them out of the hands of unsupervised children and subject them to the same safety precautions and laws as apply to weapons using gunpowder (firearms).201 Air and BB gun sales are closely controlled in New York City206 but are mentioned in the laws of only 28 states. Some of that legislation explicitly excludes them from consideration as dangerous weapons or firearms.205 National legislation that specifically equates all guns with lethal potential as firearms is an essential first step in the educational process.
In future attempts to control BB and air gun injuries, several points must be considered:
With supervision, BB and air-powered weapons can be safe training devices for children who will later move up to the responsible use of gunpowder-propelled firearms. BB injuries, deaths, and blindness will continue as long as children have the feeling they are playing with toys and the true danger of these weapons is not stressed or their use supervised. Because it has been shown that parents who allow their children to have BB or pellet guns appear to misperceive their potential for injury and allow their children to use the guns in an unsafe manner,225 specific educational material should be available to the parent before purchase, and both parent and child should jointly take a gun-use training program before using the gun.226 When parents purchase such a gun, they must recognize it is a firearm,227 dangerous both to the child using it and to innocent bystanders. The child must never be allowed to use the gun except under direct, personal supervision of the adult.228
The immediate answer does not lie in the development of better surgical techniques. Our record for salvaging these eyes has been, and remains, quite poor.204,210,214,222,229,230,231,232 As is the case of most eye injuries, the best way to prevent loss of vision from air guns is to prevent the injury from occurring.203
The BB gun or air gun cannot be made safe. For a BB projectile to be beneath the kinetic energy of 0.03 J that will result in contusion eye injury, the muzzle velocity would have to be reduced to 43 ft/s (13 m/s). When fired in the horizontal direction from a height of 5 ft, the BB would travel a mere 24 feet,46 thus would appeal only to the most placid child. The child and the parent realize that an air rifle pellet contains more energy than an individual duck/pheasant shotgun hunting shot (Table 11).
A major legislative battle to ban BB guns and air guns would probably be ineffective even if won. There would be years of appeal on Constitutional grounds, and the extensive reservoir of several million BB guns and air guns would still be available to youngsters.
Eye protectors are available that will give essentially total protection, but how do we get persons to wear them? The use of protective goggles, which several manufacturers package with the firearm, would prevent most ricochet injuries (26% of BB eye injuries)204 to the user233 but would not help the person usually injured—the one accidentally or intentionally shot by the person with the gun.
Table 11. Target and Hunting Gun Muzzle Velocity and Energy | ||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Thus, it seems we are presented with the hard truth. BB guns and air guns are widely distributed throughout the United States; they are dangerous; they cannot be recalled. In one study, more than 40% of BB and pellet eye injuries occurred when someone actually pointed the air gun at a person and pulled the trigger, showing a lack of respect for the dangers of air guns.203 Therefore, our best means of decreasing eye injuries is by a massive educational campaign aimed at teaching the user to have the same respect for a BB gun or air gun as they do for a firearm. (Children are rarely injured with firearms—everyone knows you can get killed with a shotgun.) To emphasize that BB guns and air guns should be treated as firearms, legislation classifying BB guns and air guns as firearms is recommended.
The National Rifle Association (NRA) has committed its vast educational resources, including its 25,000 NRA-certified instructors, to a stronger initiative in the area of air gun safety, particularly as it pertains to eye injury. This includes special air gun safety training programs for use by schools and other community agencies and organizations. The NRA has also revised its training material—used by millions of persons annually—to place a special emphasis on air gun safety, including coordination of safety programs with groups such as the Boy Scouts, the 4-H, and the American Legion.234 There needs to be a more concentrated effort to make available community recreational facilities for persons who wish to shoot air guns in a supervised and safe environment, as well as an emphasis on parental responsibility and supervision of youngsters using air guns.235 The Non-Powdered Gun Products Association (NPGPA), which has published targeting safety rules, should establish a certification council to ensure that BB guns and air guns meet the safety standards specified in the Standard Consumer Specifications for Non-Powder Guns (ASTM standards F589 and F590). Prospective studies are needed to evaluate the effectiveness of educational programs on the incidence of eye injuries.
It is time for a coordinated approach by the public, police, sporting associations, manufacturers and retailers, and politicians.236 The impetus to start an effective process should come from the medical community since this is where both the greatest exposure to the problem and the greatest expertise in solving it are to be found.
Shooting
The shooting sports include hunting for game and birds with rifles and shotguns, shooting at stationary or moving targets with pistols or rifles (air or gunpowder), and downing clay discs (pigeons) with shotguns. The main participants in the shooting sports are males in their thirties with a concentration of veterans and relatively few beginners. About 19.1 million people hunted with a firearm in 2007. Only about 8% of the hunters were new to the sport in 2001, and nearly 60% have been involved 10 years or more. There is a relatively heavy cross-participation among gun users—64% of trap/skeet/clay shooters, 46% of rifle target shooters, and 37% of pistol target shooters are also hunters.
It is so rare for elite shooters to be cross-dominant that a right-handed shooter with a dominant left eye should be coached from the start of his or her career to shoot left-handed (or vice versa), since the dominant eye is more important than the dominant hand for shooting accuracy.237,238,239 However, when one shoots right-handed for a lifetime, switching hands may prove inconsistent with good performance—even if the dominant sighting eye is lost in an accident. In these cases, a parallel sighting rib will allow trapshooters to use the nondominant eye while maintaining the preferred shooting shoulder. It is usually stated that pistol shooters need 20/20 near visual acuity, for proper sight alignment, whereas elite rifle shooters usually need 20/20 distance acuity.240,241 However, I have found that most presbyopic shooters prefer to have the target blurred by no more than an add of +0.50 to +0.75 D, which makes the combined blur of sight and target approximately the best combination for both pistol and rifle. Shooting glasses frequently are tinted or polarized. Choice of tint varies among shooters, with waterfowl and snowfield hunters often having a preference for glare-reducing polarizing lenses and skeet and trapshooters tending toward brown, bronze, yellow, or light gold tints.242
Although most firearms injuries are the result of intentional assault,81,243 and are thus largely unpreventable, there is also a potential for blinding ocular injury from target shooting and hunting accidents. Of the 590 gunshot eye injuries in the USEIR database, 541 (92%) were secondary to violence. The 39 injuries from sport shooting and hunting were serious (72% open globe, 21% enucleation or no light perception) and occurred mostly in males (97%) between the ages of 20 and 50 (79%). None of the injured shooters was wearing protective eyewear. Two of the seven injured target shooters were struck by fragments of the target (aluminum can) or casing from a misfired bullet, three were accidentally shot by another shooter on the range, and two were injured by the swinging arms of the clay/skeet throwing apparatus. Twenty hunters were accidentally shot, usually with a shotgun, by another hunter in their party. Two hunters were shot by the landowner for hunting while trespassing. Two elderly men (76 and 85) were injured by the gun on recoil, with one suffering dehiscence of a long-incision cataract wound by the telescopic sight that rebounded through his streetwear eyeglasses. Eight of the 32 injured hunters were not injured with a firearm: 3 cut their eye while cleaning a shot deer, 3 were hit by tree branches, and 2 were hit with wire used for towing or fences.
The primary way to avoid shooting eye injuries is by proper gun handling and shooting technique. In 1994, 32% of American households owned a shotgun or rifle, 25% owned a pistol, and 59% owned no guns.244 Only 56% of gun owners have received formal training, and 21% of gun owners keep a firearm both loaded and unlocked in the home. Appropriate gun storage (keep a gun locked, unloaded; store ammunition locked and in a separate location) and training would help to reduce firearm injuries.245,246 New York State requires that all first-time hunting license holders complete a hunter-education course. Of 125 incidents in which the injured hunter is mistaken for game (the primary contributing factor for gunshot injuries to hunters), 117 hunters (94%) were not wearing hunter orange.247,248 The time to start training for safe gun handling is in youth. Several training programs, such as the Home Firearms Responsibility courses given by the NRA, and safety pamphlets are available, but the best education is a good example set by responsible adults.
There is no currently available protective eyewear that can withstand the impact of a high-powered rifle bullet from long distances or shotgun pellets from within 15 yards. Yet, serious,249,250,251 sometimes bilateral,252,253 eye injuries frequently occur with shots from longer distances, gunpowder blasts,254 blank cartridges,255 ricochets, and impacts with other objects (tree limbs, knives, wire)201 that can be prevented with appropriate eyewear. Eyewear with polycarbonate lenses, integral side shields, and a retention strap is extremely effective in protecting the eyes from shotgun pellets in the very hazardous 15- to 40-yard range.256,257 Eyewear that passes both ANSI Z87+ and the much more stringent military ballistic test for eye armor258 is readily available and inexpensive.
Archery
Archers with uncrossed eye dominance are more accurate when the bow is used without sights, but the use of sights seems to eliminate this effect.259 Archery target shooting (longbow, recurve, compound bows or crossbows, with or without sighting aids) has a minimal eye injury risk.
About one in four archers was involved 10 years or more, and 29% of the archers were first-time participants. Twenty-nine percent of archers also hunted with a bow. The USEIR database includes three archery-related eye injuries. A six-year-old girl had an open-globe injury when shot with an arrow. Two male archers had contusion injuries (retinal detachment, retinal hemorrhage): One, wearing streetwear glasses, was struck with the bow while shooting an arrow, and the other was struck in the eye with the sighting tube that dislodged while shooting. Playing with bow and arrow is a significant cause of eye injuries in India28,260,261 and Norway.262 Adult263 and toy264 bows and arrows have sufficient energy to penetrate through the orbit into the brain.
Suggested protection is eyewear with shatter-resistant lenses for those archers who wear Rx eyewear. The functionally one-eyed archer should wear eyewear that passes ANSI Z87+ or ASTM F803. There are ASTM standards to ensure that bows (F1832, F1880, F1544 F1363), scopes (F1753), cords (F1752, F1648, F1436), and arrows (F1889, F1435, F1352, F2031) are properly constructed. Bows and arrows should not be given to children for use as toys.
War
Although military injuries are not truly sports-related injuries, the same principles of prevention apply. Witnessing the results of monocular or bilateral blindness suffered by young men during the Vietnam War and realizing that a substantial percentage of war-related blindness is preventable provided my personal impetus for involvement in the prevention of traumatic eye injuries. The incidence of eye injuries increased with the development of war munitions—land mines, artillery shells, and bombs—that accurately disperse high-velocity shrapnel fragments among the targeted personnel. Between 6% and 9% of all Vietnam War injuries involved the eye, resulting in permanent visual impairment and blindness in thousands of American soldiers.265,266 Of all hospitalized casualties of the Yom Kippur War of 1973, 6.7% sustained ocular injuries, of which 24.4% were bilateral.267 Ophthalmic injuries, usually caused by munitions blast fragments,268 accounted for 13% (19/149) of all ground war casualties from October 17, 1990, to April 13, 1991 in Operations Desert Shield and Desert Storm. Although most troops were issued protective goggles, only 3 of the 92 U.S. soldiers with eye injuries were wearing them at the time of their injury.269 None of the military who suffered eye injuries (6.8% of all casualties) in the Lebanon war were wearing eye protection.270 Devastating eye injuries continued to be a major problem in Operation Iraqi Freedom where in a 33-month period (March 2003 through December 2005), of the 797 severe eye injuries treated, there were 438 open-globe injuries (49 bilateral) and 116 eyes were removed (6 bilateral). These injuries were most commonly caused by explosions.271 Iraqi chemical warfare with mustard gas resulted in keratitis, chronic blepharitis, and decreased tear secretion in 48 victims.272
Between 1980 and 1993 there were more than 27,000 deaths among the U.S. military personnel who served 28 million person hours on active duty, averaging approximately five deaths per day. Hostile action or war accounted for only 2% of the total whereas 60% died from largely preventable unintentional injuries that occurred during their day-to-day activities and off duty.273 Most military eye injuries also were not combat related, but occurred from motor vehicle accidents, fighting, and occupational or sports activities. One in 58 eye injuries required treatment in a hospital.274
Laser weapons, small enough to be attached to an M-16 assault rifle, yet effective at a distance of more than 1 km, can produce blindness with a microsecond pulse of light from retinal burns and subretinal hemorrhage.275 Laser eye protection can impact performance and color identification in protected military personnel.276 Since huge numbers of civilians and military personnel will not have appropriate laser protection and may be exposed to blinding lasers mounted on rotary turrets attached to tanks or other military vehicles, there has been a plea from concerned physicians to ban the antipersonnel laser.277,278
The need for a comprehensive eye protection program in the military cannot be overemphasized.279 If eye armor had been worn by troops in the Vietnam War, it is estimated that 39% of the eye injuries collected by the Wound Data and Munitions Effectiveness Team would have been prevented.280 In Iraq, many (but not all) of the devastating ocular and ocular adnexal injuries (most commonly caused by IEDs) would have been prevented by polycarbonate ballistic eyewear.281,282
The military has a combat eye armor program underway that is well accepted and has prevented eye injuries.283,284 Since soldiers have occupational exposure to eye hazards that are comparable to those in civilian industry,285 the military should enforce interventions to prevent work-related eye injuries that have been effective in preventing civilian occupational eye injuries.286,287,288 Those who have had refractive surgery require the same eye armor that should be issued to all military personnel.289 Protective sports eyewear should be issued to military personnel at risk for sports eye injuries.
Fencing
Although fencing is a relatively safe sport, two fatal injuries (penetration of a face mask by a broken foil with intracranial entry through the orbit and penetration of the neck over protective bib) and a serious hand laceration with the side of the blade have prompted the formation of an ASTM committee on fencing safety, which wrote performance standards for fencing surfaces (F1543) and the impact attenuation properties of body padding and protective wear (F1631). Since the mask that permitted fatal penetration tested as “good,” there is at least one known death that might have been prevented by stricter mask penetration requirements (Fig. 13). There is a significant discrepancy between the “punch test,” mandated by the International Federation for Fencing (FIE), which requires that a mask resist perforation by a conical punch (69 N) and the force of a broken épée blade for an extension lunge from a stationary position on a hard stationary object (4,000 N).
 Figure 13. Fencing face mask. |
The breakage characteristics of foils are an important consideration. Better foils break with a relatively square end, although they almost always have one or two sharp, short protrusions and a small cross-sectional area at the break point (2.5 × 4 mm for foil, 1.5 × 5 mm for sabre, and 4 × 4 × 5 mm [triangular] for épée).290 The rate of breakage is high. (A competitive fencer usually breaks six or seven blades a season and takes four to five weapons to a match.) Some experts believe that metal blades will someday be replaced with fiberglass or carbon-fiber blades, which would be lighter, have fewer breaks, and have less lethal-shaped break surfaces; others believe that metal blades can be improved with newer metallurgical techniques.
Darts
A lawn dart is about 12 inches long with a heavy metal or weighted plastic tip on one end and three plastic fins on a rod at the other end. Although the tip may not be sharp enough to be obviously dangerous, these darts, even when thrown underhand, can penetrate the skull and the eye. Lawn dart injuries have a 4% fatality rate and account for an estimated 675 emergency department visits per year; head injuries account for 54%, eye injuries 17%, and face injuries 11%. Hospitalization (54%) is often required for eye and brain injuries. The 10 to 15 million sets of lawn darts remaining in the homes of Americans after their sale was banned by the CPSC on December 19, 1988, should be discarded.291
Indoor darts, with an eight-inch maximum length and 18 g maximum weight, rarely result in eye injuries when National Dart Association rules of play are followed. However, children rarely follow the rules and their thrown darts may cause penetrating or perforating eye injuries with poor visual outcomes, from the initial injury, or later irreversible amblyopia or endophthalmitis.292,293,294 Games involving darts are not appropriate for children unless there is strict adult supervision and the rules of play are followed.
Fishing
Fishing (62 million participants) is one of the most popular of all sport activities. Fishing attracts all age groups (32% younger than age 12 years and 12% older than age 55 years), and about 20% of those who fish call it their favorite activity.
Fishing was responsible for 143 (19.5%) of the 732 total sports eye injuries in the USEIR database.295 The fact that 44.1% of fishing eye injuries were open-globe injuries is due to several factors: Fishhooks are sharp; sinkers have a concentrated mass that fits within the orbit; the fishing line can act as an elastic cord when the hook suddenly releases from an underwater obstruction—propelling the hook and sinker toward the sighting eye; and pole tips are whipped around in close proximity to other fishermen on shore or a boat. Fishing injuries from hooks,296,297,298,299 sinkers,300,301,302,303,304 pole tips,201 fishing spears or harpoons,305,306 or the fish itself307 are usually serious. Available data do not always separate fishhooks from sinkers or other causes of fishing eye injuries, so it is not yet possible to determine how many fishing injuries, from sinkers or pole tips, really belong in the “somewhat larger” category to follow. Spectacles with polycarbonate or TriVex lenses, whether in the form of sunglasses (preferably polarized) or corrective lenses, offer protection and should be worn at all times by those fishing.308
Shattered Eyewear
As discussed previously, lacerating eye injuries from shattered eyewear are almost totally preventable.
SMALL, SOMEWHAT LARGER HIGH-VELOCITY PROJECTILES
Airsoft
Paintball
Paintball (often called war games, survival games, Pursuit, or Gotcha) started in New Hampshire in 1981 when 12 friends used air guns that fired capsules—filled with paint and designed by foresters to mark trees for harvest—in a “survival game” where the participants were able to eliminate opponents from the game by shooting them with paint pellets. Paintball is now played in over 40 countries, with 5.5 million participants in the United States in 2007. The average player is a man (82%) 25.7 years old, who plays 15 days a year for 3 years.
Paintball violates the basic teachings of traditional firearms safety courses, which emphasize two absolute rules: always positively identify the target and never point a firearm (including an air gun) in the direction of any person, animal, or object other than the intended target.235 The intentional firing of a missile at another individual in peacetime, as a game, has been criticized by the Boy Scouts, The NRA, and the Shooting, Hunting, Outdoor Trade (SHOT) industry, who strongly emphasize the safe use of firearms and strict adherence to firearm safety rules. Yet, the appeal of war games has lured players, and what started as a cottage industry of air gun and paint capsule manufacturers and field operators is now a big business. Early on, the rapidly growing sport had no controls—as exemplified by the lack of age restrictions on the sale of paintball guns.
It soon became apparent that the paint capsules were responsible for severe (7.8% open-globe) eye injuries. Players and field operators then began to use or distribute industrial safety, motorcycle, or ski goggles, despite the fact that these goggles were never tested for paintball and that industrial goggles have the warning that they are not designed for sports use.312 This eyewear often failed, resulting in severe injury to players who had assumed they were protected (Table 12).
Table 12. Paintball Eye Injuries Related to Protective Eyewear | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


