The Evaluation and Management of Eyelid and Periorbital Soft-Tissue Trauma
James W. Karesh
Marc Hirschbein
Alex On
Daniel C. Garibaldi
Injuries involving the eyelids, lacrimal drainage apparatus, and periorbital areas are common after either blunt or penetrating trauma. A detailed anatomic and functional knowledge of the ocular and periocular structures is needed for the ophthalmologist to manage such injuries. In this chapter, the evaluation and management of lacerations and other injuries involving the eyelids, lacrimal drainage system, and periocular areas is discussed. The intent is to provide a firm basis for successful treatment of such injuries both for the beginning resident and the general ophthalmologist. No attempt is made to exhaustively cover this broad subject. Rather the reader is referred to the various references at the end of the chapter for more detailed discussions of specific treatment options.
An understanding of eyelid, lacrimal, and periorbital anatomy is essential for managing injuries to these structures (Fig. 1). The following description details those anatomic features important for managing eyelid trauma. More extensive discussions of anatomy are contained in the references at the end of this chapter.5,6,7,8
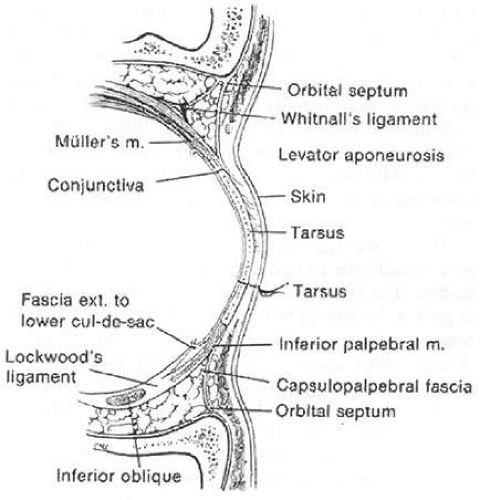 Figure 1. Eyelid anatomy. |
Skin
The upper eyelid skin is the thinnest in the body with the lower eyelid skin being only slightly thicker. There is very minimal dermal tissue associated with eyelid skin, whereas the periorbital, forehead, and cheek skin is considerably thicker with a much more substantial dermal layer. Therefore, less significant scarring occurs in the eyelids when compared with the periorbital tissues. The upper eyelid skin merges into the thicker forehead and glabellar skin at the superior orbital rim and eyebrow.
The major anatomic features of the upper eyelids include the eyelid crease and fold and the eyelashes. The normal crease is approximately 10 mm superior to the upper eyelid margin.9,10,11,12 There is some variation to this, with the eyelid crease in Asians often being considerably lower.8 The upper eyelid crease represents the point at which slips of the levator muscle interdigitate with the orbicularis muscle to insert into the undersurface of the skin. Recession of the eyelid crease associated with traumatic ptosis suggests an underlying dehiscence of the levator aponeurosis. A change in the eyelid crease can also occur after eyelid surgery or laceration repair where the aponeurotic interdigitations are disrupted.
The eyelid fold represents the point at which the looser preseptal skin overhangs the more firmly attached pretarsal skin when the eyelid is open. The eyelid fold in many Asians is lower due to both the lower attachments of the levator muscle and the lower attachment of the septum onto the levator. This allows the anterior and inferior extent of the orbital fat to be at a lower level on the tarsus.8 The full appearance of the preseptal area of the eyelid is due to the underlying fat. Loss of upper eyelid fullness can be associated with orbital fractures, where there is a relative increase in the orbital volume without an associated increase in the volume of the orbital. contents or in post-traumatic or inflammatory fat necrosis where there is a relative decrease in the volume of the orbital contents without an equal decrease in the orbit’s overall volume.13,14
The features of the lower eyelid are less distinct than the upper. Although there is a lower eyelid crease in most individuals, it is usually not as distinct as that in the upper eyelid. However, the pretarsal skin is more firmly attached than the preseptal skin, and, on careful examination, a crease may be seen 2 to 4 mm below the eyelid margin, especially in downgaze. Other creases occur in the lower eyelid and in the lateral temporal periorbital skin as aging occurs. As in the upper eyelid, the preseptal fullness of the lower eyelid is due to the presence of orbital fat. An asymmetric reduction in this fullness can be associated with orbital fractures and trauma as well as in association with fat necrosis and following lower lid blepharoplasty with over-aggressive fat removal. The lower eyelid skin merges into the thick skin of the cheek at the inferior orbital rim. A malar fat pad can be found beneath the thick skin and muscle over the zygomatic bone as it forms the lateral aspect of the inferior orbital rim.
The next layer below the eyelid skin and dermis is the orbicularis muscle. This muscle is shaped like a sphincter with attachments medially, forming the medial canthal tendon, and laterally, forming the lateral canthal raphe. The muscle extends to the eyelid margin where it forms the muscle of Riolan, which is seen as the gray line just anterior to the openings of the meibomian glands.17 Superiorly, the muscle extends under the eyebrow. The facial nerve provides the innervation to the orbicularis and can be damaged with large lacerations involving the lateral face.
Laterally, the fibers of the orbicularis muscle from the upper and lower eyelids interdigitate and become a raphe. A small tendon extends from this raphe and inserts onto the lateral orbital tubercle, which is located 3 to 4 mm inside the orbital rim. A small fat pad can be found in some individuals beneath this tendon.7 It is important to refixate the eyelids and lateral canthal tendon to the inner surface of the orbital rim when repairing lateral canthal lacerations to prevent gaping between the eyelids and the globe.
The medial canthal ligament has two heads, or tendons, a superficial head that inserts onto the anterior lacrimal crest and a deep head that inserts onto the posterior lacrimal crest.18 These two heads surround the lacrimal sac, which sits in the lacrimal fossa. The deep or posterior limb of the tendon is formed by the deep heads of the pretarsal and preseptal portions of the orbicularis muscle. The anterior limb of the tendon is formed by the superficial heads of the preseptal and pretarsal orbicularis muscle. There is also a superior supporting branch of the anterior limb that inserts onto the frontal bone.18 The integrity of this structure and of the deep head of the tendon is important for preventing post-traumatic medial canthal dystopia. The upper and lower canaliculi and common canaliculus are directly below the superficial limb of the medial canthal tendon. These structures should be considered involved in all medial canthal injuries until probing and irrigation of the lacrimal system has been performed and should be protected during surgeries in the region of the medial canthus
Orbital Septum and Fat
The orbital septum is an extension of the periosteum of the orbital rim. Superiorly this structure inserts onto the levator aponeurosis several millimeters above the level of the superior tarsal border. As already noted, this can vary from individual to individual with a much lower attachment being present in most Asians. In the lower eyelid, the orbital septum attaches to the lower eyelid retractors approximately at the level of the inferior tarsal border. Behind the septum in the upper eyelid are a medial and a central fat pad, located just anterior to the levator muscle and aponeurosis. Laterally, the orbital portion of the lacrimal gland is present behind the septum. In the lower eyelid there are three fat pads: medial, central, and lateral that are located just anterior to the capsulopalpebral fascia, which is the analogue of the levator in the upper eyelid.
Eyelid Retractors
In the upper eyelid, the eyelid retractors are Müller’s (or the superior tarsal) muscle and the levator muscle and aponeurosis. In the lower eyelid they are the capsulopalpebral fascia and Müller’s (or the inferior tarsal) muscle. The levator muscle originates just above the superior rectus muscle in the posterior orbit, travels anteriorly before changing direction at Whitnall’s ligament, and becomes an aponeurosis that ultimately inserts onto the anterior surface of the tarsus. As with the superior rectus muscle, the levator muscle is innervated by the superior division of the oculomotor nerve. At Whitnall’s ligament the aponeurosis fans out to form the so-called horns. The lateral horn separates the lacrimal gland into palpebral and orbital portions. Whitnall’s ligament and the lateral horn of the aponeurosis attach onto the lateral orbital tubercle and contribute to the lateral canthal tendon. Medially, Whitnall’s ligament fuses with connective tissue surrounding the trochlea. The aponeurosis lies posterior to the orbital septum and fat. It is only loosely connected to the orbicularis muscle anteriorly except for the slips of tissue that form the eyelid crease. This potential space between the aponeurosis and the orbicularis muscle is utilized in the anterior surgical approach to the eyelid as a way of avoiding damage to the aponeurosis. Identification of the orbital septum and fat is an important landmark during aponeurosis surgery or laceration repair.
In the upper eyelid, Müller’s muscle is a sympathetically innervated muscle 10 to 12 mm in height located immediately posterior to the levator aponeurosis. It is only loosely attached to the aponeurosis and the two can be easily separated during surgical dissection. Posteriorly, conjunctiva is only minimally adherent to it. Superiorly it originates from the posterior aspect of the levator muscle and inserts onto the superior tarsal border. The peripheral palpebral arterial arcade travels on the anterior surface of Müller’s muscle just superior to its insertion into the tarsus and is an important landmark for identifying the muscle.
In the lower eyelid, the capsulopalpebral fascia inserts into the anterior inferior surface of the tarsus. Müller’s in the lower eyelid inserts into the inferior tarsal border, but is usually quite difficult to differentiate from the capsulopalpebral fascia as the fibers of the two structures merge. The orbital septum lies anterior to the capsulopalpebral fascia with orbital fat separating the two until they fuse just prior to inserting onto the anterior face of the tarsus. There is a potential space between the orbicularis muscle and the eyelid retractors that can be utilized during lower eyelid surgery as an avascular plane for dissection. The conjunctiva can be dissected relatively easily from the capsulopalpebral fascia. Dehiscence of the lower eyelid retractors from the tarsus is thought, in some cases, to be associated with involutional entropion. Scarring between the septum, the tarsus, and the retractors can occur after orbital fracture repair and blepharoplasty, resulting in lower eyelid retraction. This is most often seen with a skin-muscle approach to repairing the orbit but can also be observed following an extensive transconjunctival approach to the orbit.
Tarsus
The tarsus is a dense connective tissue structure that forms the basic support for the eyelids. There are about 25 meibomian glands contained in the upper eyelid tarsus and 20 in the lower. The tarsus is 1 mm thick and 26 to 28 mm long. The height of the upper eyelid tarsus is about 10 mm and that of the lower eyelid is 3.5 to 5 mm.19 Müller’s muscle is attached to the superior tarsal border of the upper eyelid and the inferior tarsal border of the lower eyelid. The tarsus ends at the eyelid margin. The levator aponeurosis attaches to the inferior two thirds of the anterior surface of the tarsus. There is a potential space between the superior one third of the tarsus and the aponeurosis. The capsulopalpebral fascia inserts onto the anterior surface of the lower eyelid tarsus while Müller’s muscle inserts onto the inferior border of this structure. In both the upper and lower eyelids, the marginal artery travels between the orbicularis muscle and the tarsus 3 to 4 mm from the eyelid margin.
Conjunctiva
The palpebral conjunctiva lines the posterior surface of the eyelids reflecting upon itself at the superior and inferior fornices to become the bulbar conjunctiva covering the globe. The palpebral conjunctiva is firmly attached at the eyelid margin and to the tarsus. It is less firmly attached to Müller’s muscle and can be fairly easily dissected from this structure or ballooned away from it with saline. There is some redundancy to the conjunctiva, and a portion of it can be excised or lost without compromising either eyelid or globe function or reducing the goblet cell contribution to the tear film. In the lateral aspect of the upper eyelid and superior fornix is the palpebral lobe of the lacrimal gland and the lacrimal ductules. Deep lacerations of the eyelid can damage these structures, reducing the aqueous portion of the tear film.
Eyelid Margin
The eyelid margin represents a sandwich of tissues. Its most posterior layer is the nonkeratinized epithelium of the conjunctiva. This becomes keratinized at the mucocutaneous junction at the posterior border of the tarsus. The tarsus is the next most anterior layer and contains the orifices of the meibomian glands. The gray line or muscle of Riolan, which represents the edge of the orbicularis muscle is just anterior to the tarsus.17 The eyelid skin and eyelashes comprise the most anterior layer. Eyelashes are more numerous in the upper eyelid, which may contain two to four irregular rows of cilia. The lower eyelid contains one or two rows of eyelashes. The most medial aspect of the upper and lower eyelid margin contains a lacrimal punctum. Each is approximately 5 mm from the medial canthal angle. The puncta are nipple-like openings surrounded by a muscular sphincter. They are usually slightly inturned toward the tear lake. The tarsus ends at the punctal opening. Although not part of the eyelid margin, the caruncle, a nodular continuation of the conjunctiva containing both glandular tissue and cilia, lies just posterior to the medial termination of the eyelids at the medial canthal angle.
The puncta and vertical portions of the canaliculi are 1 to 2 mm long, becoming horizontal at a dilatation called the ampulla. The horizontal portions of the canaliculi are each about 8 mm long, where they join to become a common canaliculus which is 1 to 3 mm in length.20 The puncta are 0.3 mm in diameter while the canaliculi are 1 to 2 mm in diameter.20 Although initially traveling in the superficial and posterior aspect of the medial eyelid, the canaliculi dive deep into the eyelid and medial canthal tissue until they are below the superficial limb of the medial canthal tendon. The common canaliculus enters the lacrimal sac at the junction of its superior one third and inferior two thirds. The lacrimal sac is 15 mm in height, with 3 to 5 mm of it above the medial canthal tendon and the rest below the tendon.20 The lacrimal sac becomes the nasolacrimal duct in the bony nasolacrimal canal at the inferior orbital rim as it merges with the anterior lacrimal crest. The nasolacrimal duct enters the nose in the inferior meatus approximately 4 cm posterior to the opening of the nares. The canaliculi are lined with nonkeratinized stratified squamous epithelium. When cut, they have a grayish appearance. The lacrimal sac and duct are lined with modified, nonciliated respiratory epithelium.
Eyebrows
The upper eyelid skin merges into the thicker skin of the eyebrow and forehead at the superior orbital rim. The inferior aspect of the male eyebrow begins at the superior orbital rim, whereas the female eyebrow is usually at a slightly higher level. The eyebrow is widest medially where it overlies the frontal sinus and is narrowest laterally. It forms a mild arch as it extends over the superior orbital rim. The eyebrows are separated by the skin of the glabellar area just above the nasal root. There is a thick layer of muscle beneath the eyebrows lying anterior to the eyebrow fat pad and the deep insertion of the galea aponeurotica.
Normal Measurements
The normal palpebral fissure is 26 to 30 mm in horizontal dimension and 8 to 10 mm in height (Fig. 2).9,10,21 The normal distance from the pupillary light reflex to the upper eyelid (MRD-l) is between 2.5 and 5.0 mm and the normal distance from pupillary light reflex to the lower eyelid (MRD-2) is between 4.5 and 5.5 mm.9,10 Normally the upper eyelid rests 1 to 2 mm below the 12 o’clock border of the limbus, while the lower eyelid rests just at the 6 o’clock border of the limbus, although it may also be slightly above or below this level.22,23 The distance between the two medial canthi is normally 30 to 34 mm.21 The puncta are approximately 6 to 7 mm from the medial canthal angle. The medial canthal angle is 0 to 2 mm below the level of the lateral canthal angle in most individuals.21 The tarsus is approximately 1 mm in thickness and 24 to 28 mm in length.8 The height of the upper eyelid tarsus is usually 10 mm, and the average height of the lower eyelid tarsus is 3.7 mm.8,19
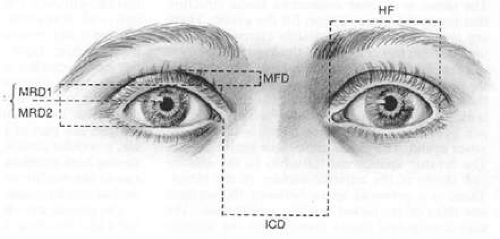 Figure 2. Eyelid measurements: margin fold distance (MFD); margin reflex distance—one (MRD-1); margin reflex distance—two (MRD-2); palpebral fissure (PF [MRD-1 + MRD-2]); horizontal fissure distance (HF); intercanthal distance (ICD). |
History
Obtaining a detailed history concerning the nature of a patient’s injury forms the basis for determining various management options. The time, cause, circumstances, and mechanism of the injury must be determined. Since many periorbital and eyelid injuries can also involve the globe, a history of any change in visual acuity or severe ocular pain after the injury should be obtained. For children, consideration must be given to the possibility of child abuse as the cause of ocular and periocular injury. In criminal cases, bullets and other projectiles must be retained and marked by the physician so that there is no break in the chain of evidence.
Treatment provided at the time of injury or in the emergency department must be determined, especially regarding wound debridement, irrigation, manipulation of tissues, the removal of foreign bodies, and the administration of antibiotics and tetanus toxoid. If an animal or human bite is suspected, all information regarding the place of injury, the ownership of the animal, and abnormal animal behavior must be obtained and the local animal control department or state health department contacted. For human bites the possibility of human immunodeficiency virus infection or hepatitis must be considered.
A history of anticoagulant use, including aspirin and the use of any other medicines, and allergies is important. An immunization history, history of sickle cell disease or other serious illness, history of drug or alcohol use, and the name of the patient’s family physician or internist should be obtained. Use of epinephrine is contraindicated in sickle cell disease. If surgical intervention is to be considered, the patient must be questioned regarding the time of last fluid or solid food ingestion.
The goal of the examination of the patient with periorbital and eyelid injuries is to determine the exact extent of these injuries. Injury to the globe and intraocular contents as well as to other facial and intracranial structures can accompany seemingly trivial as well as obviously severe periorbital and eyelid injury.28,29 It is important to carefully document all injuries and if possible to photograph them. When the patient is severely injured, unstable, or unconscious, only a partial examination may be possible and a more thorough examination performed at a later time. Saline moistened dressings or petrolatum impregnated gauze should be placed over facial and eyelid lacerations if there will be a delay between evaluation and surgical intervention. This prevents drying of the wound edges and desiccation of avulsed tissues. In addition, a protective shield should be placed over the injured tissue to prevent further injury before surgical intervention.
All patients with periocular or eyelid lacerations must have a complete ocular examination with particular attention paid to best corrected visual acuity, pupillary function and the presence of an afferent pupillary defect, intraocular pressure, ocular motility abnormalities, and globe integrity. In the obtunded patient, the reaction of the pupil to light may be the only method for assessing the presence of optic nerve injury.
All periorbital and orbital injuries must be carefully examined for depth, extent, underlying bony fractures, and the presence of foreign bodies.30,31,32,33,34 Examination gloves should be worn during the evaluation of lacerations and fractures as part of universal precautions. Although some foreign bodies can be removed without anesthesia at the time of initial evaluation and wound irrigation, many foreign bodies will need to be removed intraoperatively at the time of injury repair. Suspicion of an intraocular or orbital foreign body should preclude removal of apparently superficial foreign bodies until appropriate examinations and neuroimaging can be performed. The eyelids should be everted to determine if foreign bodies are embedded into the palpebral conjunctiva or are present in the conjunctival cul-de-sacs. Wound depth can be estimated by gently separating the wound edges with a cotton-tipped applicator. The facial bones should be palpated to determine the presence of crepitus or orbital rim fractures.29,35,36,37
The eyelids must be carefully examined to determine the integrity of the margin, skin, and tarsus. Lacerations of the medial eyelid may also involve the lacrimal system. It is important to probe and irrigate the lacrimal drainage system to determine if it is injured.38,39,40 In children, a complete evaluation of the lacrimal system may require examination under anesthesia. Evaluation of levator function can be performed by measuring the excursion of the upper eyelid from far downgaze to far upgaze and comparing this with the uninjured side. Normally, the amount of excursion is 14 to 18 mm.10 The presence of swelling or impaired motility will interfere with determining if levator function is normal. The presence of orbital fat protruding from a laceration indicates extension of a wound into the orbit. In such cases consideration must be given to occult injury to the globe, extraocular muscle, and optic nerve as well as the possibility of retained orbital foreign bodies.41,42,43 Abnormalities of orbicularis function or the presence of lagophthalmos must also be assessed as these may indicate an injury to the facial nerve and can be associated with corneal exposure. In these cases it is important to keep the cornea lubricated with artificial tear ointment at least until definitive repair of all lacerations can be performed or until it can be determined that corneal exposure and drying is no longer a problem. If a penetrating corneal or globe injury is present, a protective shield or other rigid protective covering (such as a cut down paper or Styrofoam cup) should be taped in place over the injured eye until surgical repair can be accomplished.
It is important to monitor a patient’s vision before and after surgery. Persistent post-traumatic orbital hemorrhage can result in damage to the optic nerve. Increasing levels of severe pain, proptosis, resistance to retropulsion, increased intraocular pressure, decreasing visual acuity, and worsening periorbital edema and ecchymosis in the immediate postoperative period are signs indicating orbital hemorrhage. This may require an urgent lateral canthotomy and cantholysis of both the upper and lower limbs of the lateral canthal tending with evacuation of the hemorrhage and placement of a drain to hand suction if visual acuity is to be preserved. While the local application of various coagulation enhancing materials and chemicals may be helpful, it is usually difficult to pinpoint and exact source for such postoperative bleeding. If the patient has a normal coagulation status, postoperative hemorrhage will usually stop due to clot formation and vasospasm. However, it is important to monitor the patient’s vision and intraocular pressure as well as the amount of drainage from the surgical site for at least 24 hours postoperatively following such a bleeding episode.
Laboratory and Radiologic Evaluation
Only a few laboratory tests are needed to complete the evaluation of the patient with ocular injury. A complete blood cell count and serum chemistries are often required for anesthesia purposes. A sickle cell screen should be obtained in those patients at risk for this disease, especially in the setting of hyphema or microhyphema. A coagulation profile may be of utility for those patients on anticoagulants. In certain cases, it may be necessary to obtain blood alcohol levels or a serum toxicology screen to determine the presence of various chemical substances.
Ultrasonographic examination of the globe, extraocular muscles, orbit, and optic nerve is often helpful, especially in the obtunded patient and may be used to detect foreign bodies. Computed tomography with 1 or 2mm slices and direct axial imaging with high quality coronal reconstructions is more helpful than plain radiologic films of the orbits and sinuses to determine the presence and extent of orbital fractures, foreign bodies, and extraocular injury to intracranial, nasal, intraoral, and sinus structures.35,42,44,45 If high quality coronal reconstructions cannot be obtained, direct thin-cut coronal images are necessary to best assess the integrity of the orbital structures. It can also be helpful in cases of extensive bony injuries to obtain 3D reconstructions of the orbit and skull to more accurately determine the extent of any bony injuries. Orbital MRI is generally not a helpful first line imaging study unless intracranial injury is suspected as this modality does not image bony structures as well as computed tomography.
Documentation of Injuries
All injuries must be carefully documented in the patient’s chart. This should include drawings and measurements of all lacerations, abrasions and contusions. Photodocumentation is an essential aspect of any trauma assessment and Polaroid, 35-mm, or digital photographs should be obtained at the time of initial evaluation. These records may prove vital in the resolution of any legal issues that stem from the initial trauma.
Timing of Repair56
Although it is optimal to repair eyelid injuries within 24 hours after their occurrence, these injuries can easily be repaired up to several days later. It is occasionally possible, although difficult, to primarily repair eyelid and canalicular injuries as long as 2 or more weeks after injury by carefully separating the edges of the wound, excising granulation tissue, and anatomically repositioning the tissues in their normal position. It is essential that the patient and globe be in a stable condition before acutely repairing nonlife-threatening or nonvision-threatening injuries. This is particularly true for those cases in which globe integrity has been compromised and manipulation of the periorbital soft tissues or the bony orbit may cause increased pressure on the globe, resulting in the loss of the intraocular contents or elevated intraocular pressure. Postoperative soft tissue swelling can also cause significant pressure increases within the globe owing to decreased venous outflow. In the multiply injured patient, particularly when there are severe intracranial, cardiac, and pulmonary injuries as well as ocular and facial injuries, it is important to consult with the other physicians managing the patient to determine the optimum timing for repair of each of these injuries. Communication between the various treatment teams may allow for simultaneous operative repair of a patient’s injuries involving multiple structures and prevent unnecessary additional anesthesia risk. The treatment of intraocular and optic nerve injuries often takes precedence over other injuries. In such instances, it is important to protect other injured sites from further trauma until these injuries are appropriately managed.
In general, it is important to expertly repair all lacerations of the eyelids and periorbital areas acutely. However, if it appears that definitive repair is extremely difficult at the time of initial surgical management, as in the case of significant tissue loss or severely macerated tissue, no attempt should be made to provide definitive repair at the time of initial surgical intervention. In these cases, skin grafts and complicated tissue flaps and tissue transfer techniques should be reserved for later use. A delay of 3 to 9 months, allowing for edema to resolve and scars to mature, may facilitate the determination of the exact approach best suited for the specific reconstructive challenge and may provide for better ultimate operative outcome.48,57,58 With resolution of edema and hematoma and with scar maturation there may also be a considerable improvement in eyelid position as is often the case with post-traumatic ptosis, postsurgical ectropion and eyelid retraction.
In those instances when it is essential to provide an immediate covering for the globe, as in cases of severe burns or partial avulsions of the eyelids, a temporary suture tarsorrhaphy and aggressive ocular lubrication can be utilized.56 When there is extensive or total loss of the eyelid structures with seemingly no effective method for protecting the cornea and globe from further injury or to provide adequate lubrication for these structures, it is usually possible to mobilize the remaining intact conjunctiva by extensive undermining sutured and suture this tissue to itself to cover the cornea. A full-thickness skin graft from an area that would not ordinarily be used for eyelid reconstruction (e.g., the inner thigh or the inside of the arm), banked donor skin, or even acellular dermis can then be applied over this marsupialized conjunctiva.56,59,60 Suture tarsorrhaphies should be used in those cases when the patient is obtunded, when there is facial nerve injury, or when severe lagophthalmos is present. The use of a releasable suture will facilitate observation of the globe and application of drops or ointment in those cases with co-morbid ocular trauma. Finally, although it is not common to permit the healing of eyelid lacerations by secondary intention, it is well known that after excision of medial canthal tumors and in instances of eyelid margin dehiscence, wound healing by granulation and scar formation can yield excellent results.61
Patient Preparation and The Informed Consent62
In addition to careful and thorough preoperative evaluation and surgical planning, patient preparation and meticulous surgical technique are essential for successfully managing eyelid trauma. The patient needs to be informed about the likely postoperative results of surgery and possible complications, including the chance that additional surgical intervention may be necessary for correcting postoperative problems or intraoperative conditions that could not be adequately addressed. This is vital in cases of pediatric trauma, where evaluation under anesthesia may be required to determine the full extent of ocular and periocular injury.63,64,65,66 A seemingly successful result can be completely undermined if a patient does not understand the purpose of the surgery and the results that can be expected, the extent of postoperative swelling and ecchymosis, the possible need for additional scar management or eyelid surgery, the length of time it may take for incisions to heal, and the possibility of postoperative ocular irritation. Also, patients need to be informed that certain pre-existing conditions such as hyperthyroidism, congestive heart failure, diabetes, hypertension, renal failure, liver disease, and immune deficiency states can interfere with wound healing, resulting in a less than optimal outcome.58,67,68 In addition, a variety of other problems can interfere with surgical results. These include: nutritional abnormalities, irradiated and inflamed tissues, vascular compromise as is seen in cigarette smokers and those with chronic lung disease, and patients taking corticosteroids, anticoagulants, and chemotherapeutic agents.58,69 In the young child, the occurrence of amblyopia is often unavoidable after repair of severe facial injuries. It is important to inform the child’s parents of this possibility and to recruit the assistance of a pediatric ophthalmologist to manage amblyopia as soon as the patient’s condition allows.
After any injury it is important to determine every patient’s tetanus immunization history.71,72 All patients who have not received tetanus prophylaxis for 10 years or more need to be re-immunized. For clean, nonpuncture wounds, tetanus toxoid should be administered to all patients except those who have received a full course of three boosters within the previous 10 years. For unclean wounds or puncture wounds all patients should receive tetanus toxoid except those patients with an up-to-date immunization history within the past 5 years and in addition, they should receive tetanus immune globulin. The usual dose of tetanus toxoid is 0.5 mL intramuscularly or subcutaneously, and the dose of tetanus immune globulin is 250 IU intramuscularly.
The other important prophylaxis is for rabies.73 Although cases of rabies infection in humans has become increasingly rare, it remains prevalent in feral animals in many parts of the United States.75 If the animal involved in the injury is a pet, it should be observed, under the care of a veterinarian for 10 days for signs of illness. If captured, feral animals should be euthanized and their brains tested for the presence of the rabies virus. If the animal tests positive for rabies, if the animal cannot be found but is suspected to be rabid, or if a pet develops signs of rabies, both human rabies immune globulin (20 to 40 IU/kg) and human diploid cell rabies vaccine must be administered. One milliliter of vaccine is given initially and again at day 3, 7, 14, and 28. Immune globulin is divided in two parts, one of which is infiltrated, if possible, into the wound and the other given intramuscularly.
Antibiotic prophylaxis is probably not necessary for most injuries of the eyelids and periorbital tissues owing to the extensive vascularity of these tissues..74 Antibiotic prophylaxis for bite injuries is described later. Vigorous irrigation and wound debridement and removal of all foreign material are usually sufficient to prevent wound infection without the use of antibiotics.76,77,78,79,80 However, as the consequences of infection can be catastrophic, antibiotic prophylaxis is usually provided unless injuries are very superficial or are known not to be contaminated.
In “clean, contaminated” surgery of the head and neck, including those operations involving the sinuses, oral cavity, pharynx, or nasal passages, pre- or intraoperative antibiotic prophylaxis can be provided by a single dose of clindamycin (600 to 900 mg IV), cefazolin (1 to 2 g IV), or vancomycin (1 g IV) without the need for additional postoperative antibiotic coverage.74,76,81,82 However, in contaminated or traumatic injuries, antibiotic coverage should be continued for 5 to 10 days after surgery. It is best not to use third-generation cephalosporins for prophylaxis, because they are expensive and may not be as effective against staphylococci as cefazolin, and their use as prophylaxis promotes the emergence of resistant organisms. New erythromycin-related antibiotics, while convenient for oral administration, probably do not have an adequate spectrum for anaerobic organisms or methicillin-resistant staphylococcus species. Occasionally, tetracycline-related antibiotics will provide adequate treatment for methicillin-resistant staphylococcus. However, this drug should not be used unless until cultures and sensitivities are available. Amoxicillin plus clavulanic acid, 250 to 500 mg three times daily, or clindamycin, 300 mg every 6 hours given orally, can be used postoperatively instead of intravenous antibiotics since these will provide adequate prophylaxis for most infections. It must be remembered that clindamycin is associated with pseudomembranous colitis secondary to Clostridium difficile.74 The treatment for C. difficile associated colitis is oral vancomycin, 500 mg to 2 g daily in three or four divided doses over 7 to 10 days.
Coagulation Status
The soft tissues of the face, mucosal lining of the nasal passages and sinuses, and the eyelids and orbit are quite vascular. Persistent bleeding often occurs after injury as well as during surgery. Delaying repair of lacerations for several hours will allow normal coagulation to take place and make the initial intraoperative wound evaluation easier. Patients on chronic aspirin therapy or anticoagulants may have extensive bleeding associated with their injuries and the subsequent surgical repair. Preoperatively, intramuscular or subcutaneous injections of vitamin K (10 to 25 mg every 4 hours) in patients taking anticoagulants can reduce a prolonged prothrombin time within 6 to 8 hours.53 It is important to consider the systemic indication for anticoagulation and to consult with the patient’s general practitioner if possible prior to the reversal of anticoagulant therapy. The intraoperative use of lidocaine with 1:100,000 epinephrine and the intranasal or intrasinus use of 1% epinephrine or 4% to 10% cocaine-soaked pledgets are also helpful to control persistent bleeding. Reducing the systolic pressure to 100 mm Hg or less intraoperatively maybe helpful in selected situations. Intraoperative use of monopolar or bipolar cautery is essential for hemostasis, but one must remember that monopolar cautery is contraindicated in patients with pacemakers.
Wound Hygiene
As part of the evaluation and repair of injuries to the eyelids and periorbital tissues, it is important to thoroughly cleanse all such wounds. Care must be taken to ensure globe integrity before either irrigating or investigating the extent of any soft tissue injury. Both superficial and deep wounds should be forcefully irrigated with sterile saline or sterile water to remove dirt and other materials that are clinging to the injured tissues.76,77,78,79,80,83 A large syringe with an attached 16- or 18-gauge catheter is often helpful for this purpose. Firmly embedded foreign bodies may be removed with scraping or with forceps and scissors. It may be necessary to scrub wounds with a stiff sterile scrub brush and mild soap. Chlorhexidine gluconate should not be used around the eyes, ears, or mouth because it is known to cause severe ocular injury and damage to mucous membranes. The depths of each individual laceration should be examined for debris and large foreign material. Oil, tar, superglue, or grease around or in wounds may need to be removed with solvents, such as acetone, xylol, or ether.48,84 Although these chemicals can cause significant irritative conjunctivitis, the eyes should be protected during their application. Failure to remove oil, tar, or grease as well as superficially embedded particles of dirt or gunpowder may result in permanent tattooing of the skin.48,84,85
Foreign Bodies
The management of superficially embedded foreign bodies has been discussed earlier.48,84,85 Deeply embedded material can be more problematic to manage. All organic material, such as wood, plant debris, hair, or fecal material, must be removed as retention of such material is associated with both acute infection and chronic inflammation and suppuration.48 Glass foreign bodies are simple to remove, but may be difficult to locate. Although they do not cause a significant inflammatory reaction, they may be found to protrude from the skin after wound healing has occurred. Metallic foreign bodies, such as bullet fragments, are usually sterile and can often be removed. However, deeply embedded glass, plastic, or metal can be difficult to find. Whenever there is a possibility of ocular penetration or damage to orbital structures, foreign bodies should be left undisturbed pending appropriate imaging studies. Plain radiographic films of the orbit and face will demonstrate metal- or lead-containing glass. However, as most glass does not contain lead, it may be quite difficult to find and remove all glass fragments. Computed tomography, orbital echography, or magnetic resonance imaging may be more helpful for locating deeply embedded foreign objects and wood or other organic material.34,44 Nonreactive metallic and inorganic foreign bodies, such as BB pellets, bullet fragments, and glass, when deeply embedded in the orbit do not need to be removed unless they are associated with some functional ocular deficit such as ptosis, ocular motility disturbance, or optic nerve injury. Most of these will become encapsulated by scar tissue and usually do not migrate or extrude. Nonetheless, the patient should be advised that late migration and extrusion of retained foreign bodies may occur.
Lacerations and tissue avulsions due to animal or human bites are frequently associated with infection from oral flora. Abscess formation involving both local and distant sites, such as the brain and orbit, have been associated with such injuries.95 Aggressive wound debridement and irrigation will help to reduce the number of organisms remaining in the wound site.81,93 Studies have demonstrated that forceful irrigation with normal saline alone will decrease the infection rate by 90 percent. Puncture wounds should be allowed to granulate. Other wounds should be closed in layers to eliminate dead space where fluid can accumulate and become a nidus for infection. Whenever possible, drains should be placed in such wounds to prevent the accumulation of blood and other fluids which can be a nidus for infection. Bite wounds over 24 hours old should be left unsutured and allowed to granulate, making sure that there is adequate corneal protection.
Although controversial, especially in minor injuries, given the prevalence of infection with multiple organisms following bite injuries, empiric use of antibiotics should be considered for deep and extensive bite injuries, in particular those caused by humans.76,78,81 Generally, prophylaxis in these cases is with a combination of a ß-lactam antibiotic and a ß-lactamase inhibitor, a second-generation cephalosporin with activity against anaerobes, or combination therapy with clindamycin and a fluoroquinolone.
The most common flora in animal bite wounds are Streptococcus species, Pasteurella species, anaerobic bacteria including Bacteroides species, Eikenella corrodens, and Capnocytophaga canimorsus (previously known as dysgonic fermenter type 2). A recent analysis of infected dog and cat bite wounds disclosed that Pasteurella species is the most common pathogenic organism in infected wounds, present in 50% of dog bites and 75% of cat bites.81,97 Intravenous penicillin G (2 to 4 million units every 4 hours in adults and 75,000 U/kg/day divided into doses given every 4 to 6 hours in children) should be given for dog bites where DF2 infection is possible. This is a life-threatening fulminant infection from oral flora commonly found in dogs. Penicillin G is also effective against anaerobes found in human oral flora and can be combined with intravenous nafcillin (500 mg to 1 g IV every 4 hours) for improved Staphylococcus coverage.
Continued use of a particular antibiotic or combination of antibiotics will depend upon wound culture results. Amoxicillin with clavulanic acid, 40 mg/kg/day given orally in three divided doses (maximum dosage 500 mg three times daily or 875 mg twice daily for 10 days), will provide excellent coverage against most pathogenic organisms, including anaerobes and penicillinase-producing staphylococci associated with both human and animal bites and is probably the antibiotic of choice for these injuries.74 Clindamycin (600 to 900 mg IV every 6 hours) also provides excellent coverage against both staphylococci and anaerobes.74 Other antibiotic choices include: oral cefuroxime (20 mg/kg/day in two divided doses not to exceed 500 mg/dose), intravenous cefuroxime (75 mg/kg/day in three divided doses up to 1.5 g every 6 hours in adults with life-threatening infections), or ceftriaxone (50 mg/kg/day as a single IM dose or IV in two divided doses not to exceed 2 g daily in children and 4 g daily in adults).74
In addition to the high rate of infection when untreated, bite injuries are associated with certain other specific problems. In particular, dog bites usually involve the medial canthal structures and frequently result in damage to the lacrimal drainage system.98,99,100 Additionally, while uncommon, dog bite injuries may be associated with facial fractures, especially when the wound involves the “target zone” of the orbital, nasal and maxillary region of the face.101 For this reason, it is often useful to obtain imaging studies of the orbit, nose, and sinus structures, if there is any reason to suspect the presence of bony injuries.
General anesthesia must be used in most children, in some adults, and in cases of complicated wounds or injuries involving multiple bony and soft tissues structure of the face. One of the difficulties with local infiltrative anesthesia is tissue distortion and localized hemorrhage, which can make soft tissue repair somewhat more challenging. However, infiltrative anesthesia is commonly used when repairing facial lacerations. Usually, 1% or 2% lidocaine with 1:100,000 epinephrine is utilized for such injections, although longer-acting anesthetics such as 4% bupivicaine with or without epinephrine can be substituted or added to the lidocaine. The epinephrine in the lidocaine or bupivicaine is essential for hemostasis and is the reason infiltrative anesthesia is often utilized in conjunction with general anesthesia. Topical application of various forms of lidocaine gel or solution has also been shown to be effective in those instances where injuries are relatively limited.65,103,105,106,107
Regional anesthesia, when properly utilized, can also be an effective approach for repairing many lacerations. Nerve blocks of the various branches of the trigeminal nerve can be successfully utilized in many less extensive soft tissue injuries. Adjunctive sedation is commonly used with these blocks as well as with local infiltrative anesthesia. Regional anesthesia results in less tissue distortion and recurrent hemorrhage than infiltrative anesthesia especially when it is necessary to anesthetize large areas.102 Injection of the infraorbital, supraorbital, infratrochlear, and supratrochlear nerves is adequate for the repair of most lacerations involving the eyelids, lacrimal drainage system, and periorbital soft tissue. Another useful regional block involves the pterygopalatine canal just medial to the second molar to anesthetize the greater palatine nerve, a branch of the maxillary nerve. This will successfully anesthetize the lower eyelid, zygomatic area, and lateral aspect of the nose. Similar regional anesthesia can be achieved with a maxillary nerve block using a 3-inch long 22-gauge needle inserted externally just anterior to the coronoid process, inferior to the zygomatic arch, and through the pterygopalatine gap into the pterygopalatine fossa.
When intubation of one or both canaliculi is required for successful repair of injury to the lacrimal system, the intranasal use of 4% or 10% cocaine or 4% topical lidocaine may assist in providing hemostasis. Cottonoids soaked with one of these solutions should be placed in the inferior meatus and around the inferior turbinate, remembering that the opening of the nasolacrimal duct into the nose is about 4 cm posterior to the nares just underneath the inferior turbinate. Another approach is to use oxymetazolone or neosynephrine nasal spray for hemostasis and mucosal shrinkage along with 2% viscous lidocaine gel or 4% topical lidocaine solution. As needed, the surrounding nasal mucosal structures can be locally injected with 1% or 2% lidocaine with 1:100,000 epinephrine.
Management of Specific Injuries
Basic good surgical technique is essential to achieve a successful outcome in the repair of soft tissue injuries. Rough handling of tissues can lead to crushed skin edges and necrosis, with subsequent inflammation and scarring.84,109 Extensive desiccation and crusting of the wound may require rehydration with moist dressings before the initiation of surgical repair. Reactive suture materials used for cutaneous repair should be removed 7 to 10 days following surgery to prevent significant scarring and may be replaced with adhesive paper strips such as the Steri-Strip or Micropore tape (3M Co. Medical Products Division, St. Paul, MN). Tightly tied sutures will result in cross-hatching of the wound, leaving an unsightly scar and a less than acceptable outcome. This can be a particular problem with nylon and polypropylene since these materials stretch to some extent. Meticulous hemostasis during wound repair is important since hematoma formation can cause wound edges to separate and may prove to be the nidus of a postoperative infection. Removal of any retained reactive foreign bodies, careful wound debridement, excision of areas of tissue necrosis, and control of infectious processes are also necessary to prevent excessive postoperative inflammation and scarring.
The repair of complicated lacerations requires some artistic vision and experience. Running sutures with or without a separate closure of the deeper tissues can be utilized for repairing relatively uncomplicated lacedrations.111,112 Surgical staples are quite effective for repairing scalp lacerations.113 However, interrupted sutures are almost always necessary for reapproximating wound edges in the correct anatomic position and with appropriate tension when injuries are complex and particularly when the eyebrows, eyelids, lips, nose, and ears are involved. Interrupted sutures can be removed one at a time to evacuate accumulated fluid or for drainage of purulent discharge or hematoma. It is important to reapproximate lacerated muscle during repair to eradicate dead space and to prevent pockets of blood and serum from collecting and ultimately becoming thickened scar tissue. It may be helpful to use a gravity or low suction drain in these cases to reduce the incidence of fluid accumulation.
Conservation of Tissues46
Despite the initial appearance of severe eyelid and periocular injuries associated with sharp instruments and motor vehicle collisions, actual significant loss of soft tissue is often not present. The elasticity of avulsed tissue as well as dehydration frequently results in an apparent soft tissue deficiency. Extensive surgical experience repairing severe facial and eyelid injuries is often needed to understand actual nature and extent of any soft tissue loss and the most successful path to a successful repair strategy. When there is gross tissue loss, such as when a portion of a nose or ear is missing, it is vital that all attempts be exhausted to retrieve the missing tissue, as it may be successfully re-implanted as an autograft. As it is common for apparently necrotic eyelid tissue or thin pedicles of tissue to survive owing to the extensive blood supply to the eyelids and face, it is important to conserve all injured tissues. In addition, there is often retraction of eyelid tissue when it is lacerated and this is further enhanced by tissue shrinkage due to deficient vascularity and dessication. Intraoperatively as blood flow returns and as tissue turgor improves, areas that appeared to be missing tissue or that were difficult to reapproximate will be able to be repaired.
Careful reapproximation of all injured tissues is another essential aspect of laceration repair. In some cases of severe eyelid and periorbital injury it can be difficult to orient the tissues and to determine precisely which tissues should be reapproximated. The eyebrow, eyelashes, and eyelid margin provide keys to correctly aligning and repairing these injuries. The eyebrow tissues should be approached first. Carefully suturing the upper and lower edges of this structure will help to orient the direction of surrounding periorbital lacerations.3,116,117 After reapproximation of the eyebrows, the eyelash line and eyelid margin should be sutured.118 It is helpful to remember that there are generally two or three rows of eyelashes in the upper eyelid and one or two in the lower, with the eyelashes ending just lateral to the punctum. Repair of the eyelid margin can be performed in conjunction with reapproximation of the eyelashes. In the case of a full thickness eyelid laceration, it may be helpful to first reapproximate the tarsus using interrupted 5-0 or 6-0 polyglactin sutures prior to repairing the eyelid margin. This will help to relieve wound tension and allow for optimal lash line realignment. Finally, resuturing the medial and lateral canthal angles will help to realign the eyelids into their normal position. The remaining lacerated tissues can then be repaired with the eyelid on some stretch. This will help to further define the tissue edges needing reapproximation.
In general, interrupted absorbable 5-0 or 6-0 polyglactin 910 sutures are used to repair the tarsus and the orbicularis muscle while nonabsorbable sutures of 6-0 or 7-0 nylon, silk, or polypropylene are used for the skin. The eyelid margin and lash line may be optimally aligned in some cases using 8-0 silk interrupted sutures, In children or other individuals for whom suture removal may be difficult, 6-0 fast-absorbing gut or mild chromic sutures can be used for lacerations involving the skin. Dehiscence of the levator aponeurosis can be repaired with either absorbable or nonabsorbable 5-0 or 6-0 sutures material. Generally, skin sutures are removed 5 or 6 days after repair, whereas margin sutures are removed 10 to 14 days after repair as thee is a tendency for repaired margin lacerations to pull apart when sutures are removed prior to this time. If the wound is on tension, skin sutures should be left in place longer than 5 to 6 days to reduce the incidence of wound separation after suture removal. However, leaving sutures in place for long periods of time can increase wound inflammation and scarring as well as suture abscess formation. Although polyglactin 910 sutures can be utilized for lateral canthal tendon repair, nonabsorbable 5-0 nylon or polypropylene sutures can provide a more permanent reattachment to the lateral orbital tubercle and periosteum. This same suture material should be used for reattachment of the medial canthal tendon as well, although in cases of traumatic telecanthus the suture may be attached to a wire or a small bone screw.120,121,122 In these cases, a 4-0 or, in rare instances, a 3-0 nonabsorbable suture is used to attach the tendon to the wire since the reattached tendon is on considerable tension. Lacerations involving the canaliculi are most easily repaired using 6-0 or 7-0 absorbable chromic or polyglactin 910 sutures.39,40,123,124 Lacrimal sac lacerations are usually repaired with 4-0 or 5-0 absorbable sutures of the same material. Mattress sutures of 4-0 silk placed across repaired medial eyelid avulsion flaps and tied over bolsters will reduce tension across these wounds and possible postoperative wound separation. This suture is particularly helpful after repair of significant canalicular lacerations. Steri-Strips can be effectively used to support wounds involving the cheek, forehead, and lateral canthus and can also be used after suture removal to prevent wound separation. Tincture of benzoin or gum mastic can be used in conjunction with Steri-Strips to provide increased skin adherence.
Draping and Patient Preparation
Prior to laceration repair, the patient’s entire face and hair should be thoroughly scrubbed with mild soap, diluted hexachlorophene solution, or povidone-iodine scrub solution. It is important to remove all make-up and debris. While the eyebrows should never be shaved or cut, a man’s face may be shaved if necessary. This should be followed by either the use of povidone-iodine or hexachlorophene solution. The nasal cannula used in local anesthesia with sedation can be scrubbed along with the face as shaving causes spreading of skin flora. If the patient is undergoing surgery with local anesthesia, topical anesthetic drops should be instilled in the conjunctival cul-de-sacs to reduce ocular irritation before cleaning the face. After the surgical preparation of the face, the cul-de-sacs should be irrigated with saline to remove any remaining cleansing solution.
To successfully repair extensive lacerations it is important to have the entire face in view to better visualize the interconnection between the various soft tissue structures of the face and to provide a normal comparison for damaged eyelids and periocular structures. A turban using two towels and a folded half sheet should be placed around the head. Towels can then be placed over the lower face, leaving the nose and, if necessary, the mouth exposed. The endotracheal airway used in general anesthesia can be draped off with towels. Should nasal cannula oxygen be administered and cautery utilized for hemostasis, care should be taken to avoid creating a reservoir of flammable oxygen during draping. Head drapes should be positioned snugly so that they do not become loosened during surgery. A split sheet can be used to complete facial draping. Surgical staples are often helpful for reducing movement of the draping material or in draping out large areas of the head and neck. Plastic adhesive polyethylene film may also be useful for covering difficult-to-drape areas.
Skin
In general the skin is sutured with interrupted or running nonabsorbable sutures such as 6-0 or 7-0 silk, nylon, or polypropylene. Eyelid skin may be reapproximated with 8-0 sutures for optimal result. Running sutures can be used in long linear lacerations. However, interrupted sutures are better able to reapproximate ragged edges and irregular lacerations. It is important to suture significant underlying orbicularis muscle lacerations to prevent the appearance of depressed areas of skin due to lack of tissue bulk.
Tarsus
The tarsus is a dense connective tissue structure that provides the eyelid with stability. For this reason it is important that this structure be carefully sutured as a separate layer when it is lacerated. Generally, 5-0 or 6-0 polyglactin 910 interrupted sutures are most effective for this, although any absorbable suture can be used. It is important to make sure the suture knot faces anteriorly so it does not abrade the cornea. In those instances where the tarsus is fractured in small pieces or is partially missing, this structure can be minimally trimmed to allow its reapproximation. Generally, the lacerated tarsal edges should be relatively parallel to each other for effective closure. The palpebral conjunctiva does not need to be sutured if the tarsus and orbicularis muscle are successfully reapproximated. Since at least a 3 mm wide band of tarsus is required to achieve a stable eyelid position, it may be necessary to develop a sliding tarsal flap to bridge an area of eyelid missing tarsal tissue. This can then be covered with a sliding skin–muscle flap.
Deep lacerations and puncture wounds of the eyelid can involve the levator muscle or its aponeurosis. In complicated injuries it can be difficult to visualize this structure. Knowledge of eyelid anatomy is essential for successfully repairing levator injuries. In linear vertical lacerations involving the tarsus reapproximating the tarsal edges may be sufficient for realigning the edges of the aponeurosis so that they can be sutured. Absorbable sutures are sufficient for this purpose. Horizontal or irregular lacerations are more problematic. In cases of simple horizontal lacerations, it may be possible to separate the edges of the wound, visualize the aponeurosis, and suture it to its normal position with a long-lasting absorbable or nonabsorbable 5-0 or 6-0 suture. However, in complicated or ragged lacerations, this can be a difficult task owing to the marked disruption of the normal eyelid anatomy. If the orbital fat and septum can be identified, the aponeurosis and muscle will be found immediately posterior or beneath them. If the surgical repair is being performed with the patient under local anesthesia with minimal sedation, asking the patient to look up and down will cause the aponeurosis to move, thereby facilitating its identification. Under general anesthesia this is not possible and only anatomic landmarks can be used. It may be possible to identify the levator muscle by mobilizing the superior rectus muscle and examining its dorsal surface posterior to the level of Whitnall’s ligament. If the eyelid is extensively mangled, it may be impossible to accurately identify either the aponeurosis or the levator muscle. In such cases, it is important not to widely dissect and explore looking for the edges of these structures as this can often cause more damage to already injured tissues. In such cases, delayed repair of these structures several months after initial wound repair and healing has occurred will allow a successful correction of the eyelid position to be performed.
Orbicularis Muscle
To take tension off of the eyelid closure and to cover septal lacerations, it is helpful to suture the orbicularis muscle with interrupted buried 5-0 or 6-0 absorbable sutures. When the orbicularis layer is adequately sutured it is not necessary to suture the septum. In fact, suturing this latter structure may result in lagophthalmos since it is very inelastic.
Orbital Septum
When the septum is lacerated, orbital fat will prolapse into the wound. These deep injuries are associated with occult globe perforation, optic nerve injury, orbital hemorrhage, and orbital infection. Generally the septum does not need to be repaired, but the orbital fat should be repositioned, if possible, and the orbicularis muscle closed over it to retain it in its normal position. If the fat has been exposed for 24 hours or appears necrotic or hemorrhagic, it should be excised to prevent it from becoming a nidus for infection. Orbital fat is not well vascularized and frequently undergoes necrosis after injury.
Conjunctiva
Isolated lacerations involving the conjunctiva rarely require repair. However, they frequently accompany eyelid margin lacerations and avulsions. When the fornices are involved, repair of the conjunctiva will help with recreating the normal relationship between the globe and the eyelid. It will also help to reduce scarring and contracture of the posterior lamella of the eyelid which is associated with cicatricial lid retraction and entropion. Usually it will also be necessary to repair any laceration of the bulbar conjunctiva associated with disruption of the fornix. This will also prevent adhesions of the globe to the eyelid. Conjunctival lacerations are usually repaired with 7-0 or 8-0 gut or polyglactin 910 sutures. It is important to bury the knots of these sutures to prevent them from abrading the cornea or causing ocular irritation.
In general, strict conservation of injured tissues should be maintained when addressing these types of injuries. However, prior to closure of eyelid margin and tarsal lacerations, the wound edges can be trimmed minimally to allow better approximation of the repaired tissues. Initially a 5-0 or 6-0 interrupted absorbable suture, preferable polyglactin 910, should be placed in the tarsus 1 to 2 mm from the eyelid margin (Fig. 3). In the upper eyelid, this should be a partial-thickness bite, whereas in the lower eyelid, this may be a full-thickness bite, because corneal abrasions are less likely from lower eyelid sutures. All tarsal sutures must be placed so that when tied the knots face toward the skin surface and not toward the cornea. This initial suture is crossed to pull the edges of the wound together to determine proper suture placement and misalignment of the margin. After placement of this suture, interrupted 6-0, 7-0, or 8-0 silk sutures are placed in the eyelid margin. One suture is placed in the mucocutaneous margin, one in the gray line, and one in the posterior eyelash line. The suture bites should be approximately 2 mm from the edge of either side of the laceration and 2-mm deep.
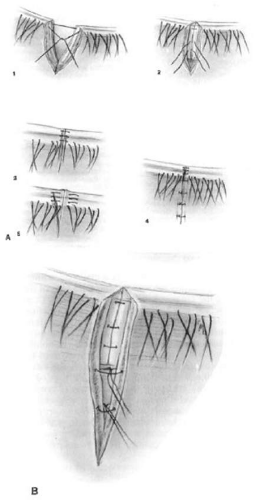 Figure 3. A. Eyelid margin repair. Method demonstrated shows placement of tarsal sutures (1 and 2) followed by placement of interrupted sutures in eyelid margin (3) and routine closure of skin (4). Instead of interrupted sutures, the margin can be closed with vertical mattress sutures (5). B. Eyelid margin repair demonstrating closure of the tarsus and orbicularis muscle. |
To prevent postoperative notching of the margin, it is important to cause eversion of the wound edges after the silk margin sutures are tied. This will prevent notching or recurrence of notching after wound healing has occurred. It may be helpful to employ mattress sutures placed in the eyelid margin in a near-near-far-far configuration to achieve the best approximation margin lacerations as well as eversion of the wound edges. Before the margin sutures are tied, additional absorbable sutures of polyglactin 910 can be placed intratarsally. Two to three such sutures are usually sufficient in the upper eyelid tarsus, and one to two are placed in the lower eyelid tarsus. The silk sutures in the margin are usually tied before the intratarsal sutures, but this may vary from surgeon to surgeon. When the margin sutures are tied, the two posterior margin sutures are tied through the anterior margin suture to prevent the suture ends from abrading the cornea. Traction on the margin sutures is helpful for reapproximating the other eyelid tissues. The intratarsal suture closest to the margin is tied next. In some cases, it may be helpful to tie this suture before the silk sutures in the margin are tied to properly reapproximate the edges of the wound. The other tarsal sutures are tied after the margin is correctly aligned. Absorbable sutures should be used to reapproximate the orbicularis muscle after the tarsal sutures are tied. The skin is closed with 6-0, 7-0, or 8-0 silk, nylon, or polypropylene sutures. In children, 6-0 mild chromic or fast-absorbing gut sutures can be used for skin closure.
When margin lacerations involve the canaliculus, intubation of this structure with silicone tubing is required for its re-anastomosis.40,130,131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149 Although monocanalicular stents can be utilized, bicanalicular intubation will be more helpful for both aligning the canaliculus as well as the eyelid margin. Traction on the silicone stent when tying the 7-0 sutures used to align the canaliculus will reduce the tension needed to tie these sutures and the incidence of suture breakage. A 4-0 silk mattress suture placed across the wound on the skin surface and tied over bolsters is also helpful for the postoperative stabilization of these wound repairs. In some instances, a suture tarsorrhaphy may be required to ensure the proper wound healing and alignment, particularly in those instances of very complicated wound repairs.150
Management of Specific Eyelid and Periorbital Injuries
Contusions are bruising injuries frequently associated with blunt trauma. The injured tissue becomes edematous, and there may be an underlying hematoma. There may also be associated subconjunctival or orbital hemorrhage. Usually such injuries will resolve without sequelae and without the need for therapy beyond the use of cold compresses for 24 to 48 hours followed by warm compresses. A short course of low-dose oral steroids may help to accelerate the reduction of wound associated edema. However, these should be used with caution as they can be associated with significant sequelae including an exacerbation of diabetes and certain infectious processes. While entirely without scientific substantiation, a homeopathic herbal preparation, Arnica montana, which is available in many naturopathic pharmacies and health food stores, can be utilized either topically or in sublingually to reduce postoperative bruising. Many patients and physicians anecdotally report significant improvements using this preparation in a dose of 3 to 5 pills sublingually three times daily for the first postoperative week. However, to date there have been no peer-reviewed articles that have supported this finding. Dark glasses and cosmetic cover-up may help to further mask the presence of periorbital ecchymoses. Occasionally, the swelling may be severe and cause a dehiscence of the levator aponeurosis. However, this often cannot be determined until there has been resolution of the acute injury.
Eyelid contusions may be markers for more severe eyelid, anterior segment and posterior segment injury.28 For example, a large review of bungee cord injuries disclosed that 60% of patients had eyelid ecchymosis and edema. This mechanism of injury was associated with eyelid lacerations in 24%, hyphema in 63%, retinal tear or detachment in 4 patients and an open globe injury in 7 patients.151 Similarly, eyelid trauma is the most common ocular sequelae of airbag injury and is frequently associated with anterior and posterior segment trauma.152 Given that eyelid contusion is a readily apparent injury to the casual observer, it may be used as a marker of severe ocular trauma and should prompt referral for detailed ophthalmic evaluation.
Blepharohematoma may also serve as a marker for more severe intracranial injury such as skull base fracture or intracranial hemorrhage.153 Significant hematomas of the eyelid and periorbital structures may not spontaneously resorb. If left untreated, this can provide a nidus for infection and result in significant scarring. While still in the “currant jelly” stage, a persistent hematoma can be easily evacuated with a simple skin incision. This incision should be placed within the eyelid crease, a skin fold, or a relaxed skin tension line to reduce the chance of postoperative scarring. When liquefied, the hematoma can be aspirated using a large-bore (16- or 18-gauge) needle. Loculated hematomas may require the aspiration needle to be inserted several times in different places. Patients should be warned that while initially unilateral, swelling and ecchymoses may spread to the uninjured side or to other portions of the face. Edema and hematoma will persist longer on the side on which the patient sleeps. Blunt trauma to the eyelids is often associated with orbital or periorbital fractures, rupture of the globe, or intraocular injury. For this reason, a complete ocular examination is essential after such injuries. In addition, the presence of proptosis may indicate an associated orbital hemorrhage. Evaluation of the patient’s vision, pupillary function, and intraocular pressure for the first 24 hours after injury is important for identifying the presence or occurrence of compressive optic neuropathy associated with orbital hemorrhage.
Eyelid Abrasion.48
This type of injury involves the epidermis and superficial dermis. Deeper injuries involving full-thickness dermis are considered lacerations. After cleansing with mild soap or antiseptic preparations, such as diluted povidone-iodine or hexachlorophene, and removal of superficial foreign bodies, these wounds are usually left uncovered except for antibiotic ointment. Large abrasions or those that may become exposed to dirt or debris and are therefore at a risk for secondary infection may also be covered with a nonadherent dressing. Unless abrasions are quite deep, they usually heal without significant scar formation. In cases of large abrasions, patients should be advised to avoid excessive sun exposure to minimize skin hyperpigmentation.
Recent work has disclosed that the single best predictor of the need for surgical intervention in cases of thermal injury to the eyelids is the severity of the initial burn itself with 100% of severe burns and 50% of moderate burns requiring surgery.161 This study also revealed that prophylactic use of ocular lubricants was associated with a decrease in requirement for surgery from 30% to 18.4%.
In general, unless the depth of a chemical or thermal burn extends through the full thickness of the dermis, the cutaneous aspect of such injuries can be managed as an abrasion. After copious irrigation and debridement, superficial cutaneous injuries through partial-thickness dermis are allowed to granulate during the healing process. Antibiotic ointments and nonadherent dressings are used for wound coverage and as a prophylaxis for infection. Artificial tear ointments may be needed to lubricate the cornea if lagophthalmos is present after early eyelid edema subsides or if chemosis and conjunctival prolapse occurs. When ectropion or severe eyelid retraction occurs due to postburn scarring, scar excision and skin grafting may be required after the acute phase of wound healing has passed. A suture tarsorrhaphy is a helpful aid for repositioning markedly prolapsed and edematous conjunctival tissue. It is also helpful for protecting the cornea when there is lagophthalmos and corneal exposure.
When deep dermal injuries occur in association with severe third-degree burns, the wound would be gently cleaned and carefully debrided. The early application of a meshed or split-thickness skin graft will reduce postburn scarring and ectropion.60,155,162,163,164,165 The use of banked or artificial skin substitutes may be considered.60 A suture tarsorrhaphy should be used to provide corneal protection and to keep the eyelids on stretch. The vigorous use of antibiotic ointments is essential in the early phase of wound healing to prevent infection. Definitive full-thickness skin grafting is usually performed after the acute phase of wound healing, usually at about 8 weeks after the initial burn. However, case reports in the literature serve as a reminder that there can be no hard and fast rules dictating the timing of repair in individual patients presenting unique reconstructive problems.164,166 If there is significant lagophthalmos or ectropion and the patient is unstable or not yet ready for skin grafting, it may be necessary to create intermarginal adhesions that can later be released. Significant long-term sequelae, such as lower lid retraction and ectropion, should be anticipated and may require multiple surgical procedures to achieve acceptable cosmetic and functional outcome. Allografts, such as temporalis fascia, may prove useful in reconstruction, and have been used successfully as lower eyelid suspension slings in the presence of highly contractile scar tissue.167,168 Acute changes in scar configuration should be evaluated, as basal cell carcinomas have been shown to arise within eyelid burn scars.169,170
Vigorous ocular lubrication must be continued until acceptable eyelid closure and corneal protection is achieved. In some cases, it may be possible to perform full-thickness skin grafting somewhat earlier than 8 weeks after injury. Severely burned patients are hospitalized and usually under the care of a burn team, which is responsible for their overall management. The ophthalmologist must act in concert with the team members and their overall management approach.
Accidental tattoos occur when small embedded foreign bodies, especially asphalt or tar, are not removed from abrasions or lacerations. When left in place they become fixed to the tissue within 12 to 24 hours after injury. Removal of these particles requires energetic scrubbing and debridement, occasionally necessitating general anesthesia. The use of solvents (e.g., acetone, xylol) may also be helpful in removing oil-based debris. If tattooing occurs, dermabrasion or surgical excision is required for removal of the pigmented areas after wound healing has taken place.
Eyelid gangrene and necrotizing fasciitis are unusual occurrences after trauma, but may be observed in diabetics and alcoholics following minor trauma180 and may be associated with immunosuppression.179,180 The mortality rate in this condition has been reported to be as high as up to 12.5% due to periorbital spread of the infectious process as well as production of various toxic products by the organisms involved in this process.178 The blood supply to the eyelid is quite rich, and even thin flaps of eyelid tissue will usually survive intact when sutured into place. However, skin infections associated with Proteus, Pseudomonas, Staphylococcus, and Streptococcus species have all caused gangrenous and necrotizing skin reactions. Treatment options in such cases are based upon controlling the infectious process with appropriate intravenous and topical antibiotics combined with debridement of necrotic tissues and maintenance of corneal protection. Hyperbaric oxygen, tetracycline, vitamin C, heparin, steroids, and other traditional and nontraditional interventions have been utilized as adjunctive treatments in this condition. Some advocate a conservative approach to the management of eyelid necrotizing fasciitis rather than aggressive debriding.181 Regardless of debridement technique, it is vital to obtain wound cultures to determine proper antibiotic coverage and to begin empiric broad spectrum coverage while awaiting culture results. Definitive repair of the eyelid tissues should be deferred until the infectious process and all associated inflammation has resolved. Considerable scarring can be expected after severe eyelid infections, and skin grafts or flaps as well as other more complicated procedures are usually needed to surgically correct the resulting eyelid abnormalities.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


