The Dizzy Patient: Disturbances of the Vestibular System
Ronald J. Tusa
VESTIBULAR SYSTEM: AN OVERVIEW
The vestibular system serves to stabilize eye position and movements during changes in head rotation and is an essential mechanism for clear vision. In fact, patients with bilateral vestibular defects must interrupt walking in order to see, and while reading a book they must even brace the head against the wall to prevent the smallest head movements transmitted from each heart beat. A classic article written by a physician describes the problems he experienced from ototoxicity.1 This chapter describes the pathophysiology of vestibular function, elaborates the clinically relevant symptoms, and reviews treatment and management options.
Normal Function: The Vestibular Reflexes
Vestibular reflexes are triggered by head movements. Imagine a bird-watcher standing in a rocking boat traveling downstream (Fig. 18-1A). To identify a bird roosting on a tree, the image of the bird must be kept stable on the retina by three separate vestibular reflexes (Fig. 18-1B). As the boat pitches up and down the eyes must move in the opposite direction and synchronously with the angular motion of the head to keep the eyes stable in space. This is accomplished by the angular vestibulo-ocular reflex (VOR), which is sensed by the semicircular canals in the inner ear (Fig. 18-1B). As the boat moves down the river toward the bird, the eyes must move horizontally synchronously with the linear motion of the boat. This is accomplished by the linear VOR, which is sensed by the otoliths in the inner ear (Fig. 18-1C). Figure 18-1D shows the most complicated reflex as the boat tilts left and right. To keep the head and eyes level during tilt to the right, the right eye is elevated in the orbit and the left eye is depressed (skew deviation). Both eyes undergo torsion to the left within the orbit (counterroll deviation), and the head is tilted to the left on the body (head tilt). This is accomplished by the ocular tilt reflex, which is sensed by the otoliths. Without these vestibular reflexes, visual acuity would be degraded and diplopia would occur. Table 18-1 lists the three vestibular reflexes, the sensory organs involved, and the motor output for each reflex.
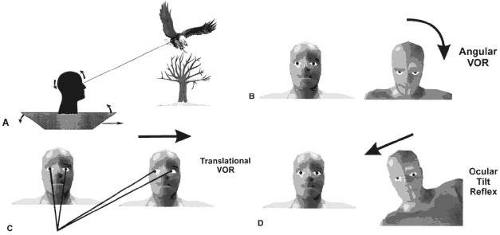 Fig. 18-1. Illustration of vestibulo-ocular reflex (VOR) and ocular tilt reflex (OTR). A: Bird-watcher standing in a rocking boat traveling downstream. B: As the boat pitches up and down, the angular VOR moves the eyes in the opposite direction, synchronous with the angular motion of the head. C: As the boat moves down the river toward the bird, the linear VOR moves the eyes horizontally in the opposite direction, synchronous with the linear motion of the boat. D: As the boat tilts to the left and right, the OTR tilts the eyes and head in the opposite direction to maintain an earth-horizontal plane. The figure shows what happens with tilt to the right. The right eye is elevated in the orbit and the left eye is depressed (skew deviation); both eyes undergo torsion to the left within the orbit (counterroll deviation), and the head is tilted to the left on the body. |
TABLE 18-1. Vestibular Reflexes | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||
PATHOPHYSIOLOGY
Peripheral Structures
The vestibular sensory organs lie within the membranous labyrinth of the inner ear, protected in the petrous portion of the temporal bone. The membranous labyrinth consists of three semicircular canals (SCCs)–the anterior, posterior, and horizontal–that lie 90 degrees (orthogonal) to each other, and two otoliths, the utricle (horizontally aligned) and the saccule (vertically aligned) (Fig. 18-2). The labyrinth is innervated by the vestibular nerve, which is part of the eighth nerve. The vestibular nerve contains two fascicles, the superior and inferior divisions. The cell bodies of each axon of the eighth nerve lie in the Scarpa ganglion, located in the internal auditory canal. The superior division innervates the utricle and the anterior and horizontal SCCs. The inferior division innervates the saccule and posterior SCCs. Within each semicircular canal is an area of hair cells that protrude their processes into a gelatinous matrix called the cupula. Angular head acceleration imposes inertial forces on the endolymph fluid within the canal, which causes relative fluid flow through the canal in the direction opposite to that of head acceleration. This flow deflects the cupula and bends the hair cells (Fig. 18-3). During head acceleration, these hair cells bend in proportion to head acceleration and change the neuronal firing rate in the eighth nerve. Because each Scarpa ganglion is spontaneously “firing” at 100 spike/sec, head motion (acceleration or deceleration) modulates this firing rate. The firing rate is increased for ipsilateral angular head movements and decreased for contralateral angular head movements. The otoliths also contain a local region of hair cells. The hair cells protrude their processes into a gelatinous matrix called the macula, which is covered by a surface of calcium carbonate crystals, the otoconia. The otolith organs respond to linear acceleration and sustained head tilt relative to gravity. Linear acceleration (including tilt of the head) causes these crystals to move, which bends the hair cells and modulates the firing rate in the eighth nerve. The firing rate is increased for ipsilateral linear head movement or tilt, and is decreased for contralateral linear head movement and tilt.
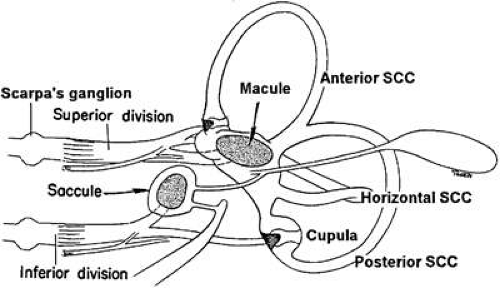 Fig. 18-2. Labyrinth. See text for details. |
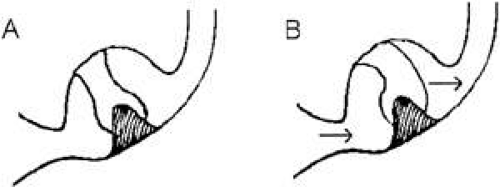 Fig. 18-3. A: Enlarged view of cupula of the horizontal semicircular canal when the head is still. B: The arrows indicate direction of endolymph flow during head rotation to the left. |
Semicircular Canals
Each SCC innervates two eye muscles by means of a three-neuron arc. The central connections of the horizontal and anterior SCCs on one side are shown in Figure 18-4. The projections of these two SCCs are shown together because usually they are both involved in vestibular neuritis,2 the most common cause of severe vertigo. The pathophysiology of vestibular neuritis is diagrammed in Figure 18-5. Because the Scarpa ganglion on each side normally is firing at 100 spikes/sec, any loss of activity on one side results in relative excessive excitation from the intact side. This large bias in neural activity causes nystagmus. The direction of nystagmus is labeled according to the direction of quick phase, but the vestibular deficit is actually driving the slow phase of the nystagmus. Vestibular neuritis results in a mixed horizontal and torsional nystagmus. This pattern of nystagmus is caused by the innervation pattern of the superior division of the eighth nerve on the intact side (recall that the superior division innervates the horizontal and anterior semicircular canals; Fig. 18-2). Relative excitation of the horizontal SCC causes horizontal nystagmus with the slow phase toward the side of the lesion. Figure 18-5 depicts a left-sided lesion, which would cause a right-beating nystagmus. Relative excitation of the anterior SCC causes torsional nystagmus (counterclockwise nystagmus for a left-sided lesion). Because of the confusion over whether to label torsional nystagmus from the perspective of the observer or the patient, the current trend is to label torsional nystagmus according to the direction of the quick phases with respect to the patient. Thus, a left-sided lesion results in right-beating and right-torsional nystagmus (Fig. 18-5B). There are two other key features of vestibular nystagmus. The intensity of nystagmus is increased when fixation is blocked (Fig. 18-5B depicts increased nystagmus when the subject looks through Frenzel or 20-diopter lenses), and the intensity of nystagmus also increases when the patient looks in the direction of the quick phases.
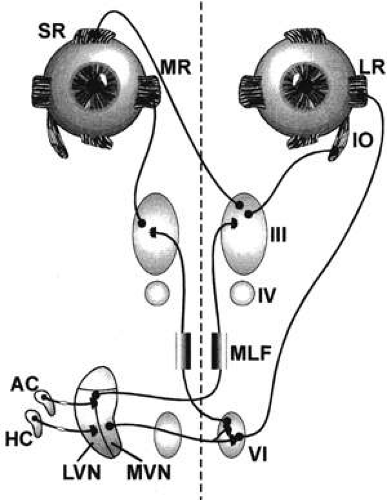 Fig. 18-4. Central connections of the horizontal and anterior semicircular canals mediating angular vestibulo-ocular reflex. Primary afferents of the horizontal semicircular canal (HC) project to the medial vestibular nucleus (MVN). Neurons in the medial vestibular nucleus project across the midline to terminate in the sixth nerve nucleus. Two types of neurons are in the sixth nerve nucleus, abducens neurons that project to the lateral rectus (LR) muscle, and interneurons that cross the midline and travel up the medial longitudinal fasciculus (MLF) to innervate the medial rectus subnuclei of the third nerve nucleus. Primary afferents of the anterior semicircular canal (AC) project to the lateral vestibular nucleus (LVN) and MVN, which in turn project across the midline and travel up the MLF to terminate in the superior rectus and inferior oblique subnuclei of the third nerve nucleus. |
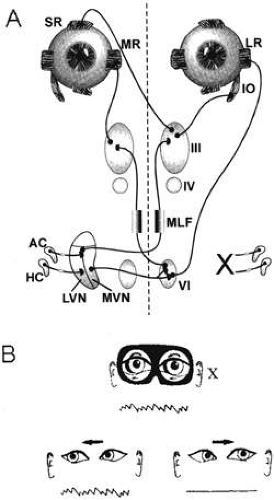 Fig. 18-5. Acute unilateral loss of semicircular canal function causing vestibular nystagmus. A: Disruption of the left superior division of the eighth nerve from vestibular neuritis. Loss of spontaneous neural activity from the left side causes slow phases to the left from relative excitation of the right horizontal semicircular canal (HC). B: Features of nystagmus. By convention, right eye position is up and left eye position is down. As the eyes move across the orbit, a quick phase resets the eyes back to the right. Quick phases are generated by burst cells, which are not part of the vestibular system. Nystagmus is labeled according to the direction of the quick phases. Consequently, this would be called a right-beating nystagmus. The lesion also disrupts spontaneous neural activity from the left anterior semicircular canal (AC), which results in right torsional nystagmus (the superior pole of each eye beats right). The intensity of nystagmus increases when the patient looks in the direction of the quick phases (B, bottom). If fixation is blocked by Frenzel glasses, nystagmus also increases and is seen clearly even in primary gaze (B, top). |
Otoliths
Each otolith innervates four eye muscles by means of a three-neuron arc. The central connections of the utricle on one side are shown in Figure 18-6.3 The projection to the vertical muscles causes vertical eye deviation and torsion during head tilt. The projections in the lateral and medial vestibulospinal tracts mediate the head tilt during the ocular tilt reflex. Acute loss of function of the utricle on one side from the eighth nerve section or vestibular neuritis causes a pathologic ocular tilt response because of the unopposed excitation of the intact utricle. Figure 18-7 depicts the results of a left-sided lesion.4 Excitation of the right superior rectus and oblique muscles causes elevation and intorsion of that eye. Excitation of the left inferior rectus and oblique muscles causes depression and extorsion of that eye. Excitation of the neck muscles innervated by the intact vestibulospinal tracts causes a left head tilt.
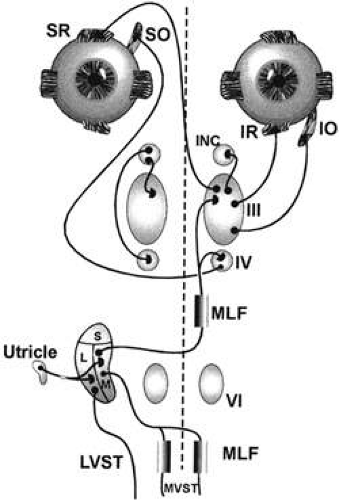 Fig. 18-6. Central connections of the utricle mediating the ocular tilt reflex. This figure illustrates the projections from the right utricle. Primary afferents of the utricle project to the lateral (L) and medial (M) vestibular nuclei. Neurons in the lateral vestibular nucleus cross the midline and travel up the medial longitudinal fasciculus (MLF) to project to the fourth nerve and third nerve nuclei, which innervate eye muscles involved with vertical and torsional eye movements. The third nerve nucleus also innervates the interstitial nucleus of Cajal (INC). The INC in turn projects back to the third nerve and fourth nerve nuclei. Neurons in the L and M vestibular nucleus also project to the spinal cord through the lateral and medial vestibular spinal tracts (LVST and MVST). |
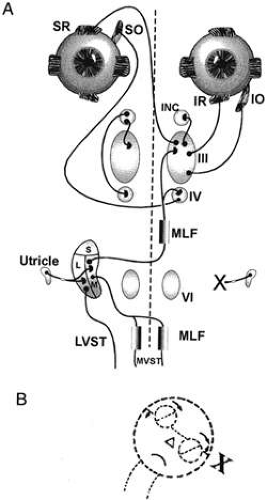 Fig. 18-7. Unilateral loss of the utricle, causing pathologic ocular tilt reflex. A: Disruption of the left utricular division of the eighth nerve from vestibular neuritis. B: The pathologic ocular tilt reflex from this lesion. Relative excitation of the right medial vestibular nucleus (M) causes elevation and intorsion of the right eye (mediated by the right superior rectus and right superior oblique muscles), and causes depression and extorsion of the left eye (mediated by the left inferior rectus and left inferior oblique muscles). Excitation of the neck muscles innervated by the intact vestibulospinal tract causes a left head tilt. |
CLINICAL ASSESSMENT
History
Determining a patient’s history is by far the most important part of a clinical evaluation. Unfortunately, taking a good history can be tedious because complaints by patients with dizziness are often vague and frequently confounded with anxiety-provoked symptoms. For these reasons a preliminary questionnaire is helpful. Three key items of the history are most helpful in determining the cause of dizziness.
Tempo.
It must be determined whether the patient is suffering from an acute attack of dizziness (3 days or less), chronic dizziness (more than 3 days), or episodes of dizziness. An acute attack frequently is caused by vestibular neuritis, labyrinthitis, Ménière disease, or brainstem infarct. Chronic dizziness often is caused by an uncompensated unilateral vestibular defect, bilateral vestibular hypofunction (ototoxicity, sequential vestibular neuritis), or disequilibrium from a variety of different causes, or psychological problems. If the patient suffers from episodic symptoms, the average duration of the spells should be determined. Spells that last for seconds are usually caused by benign paroxysmal positional vertigo (BPPV) or orthostatic hypotension; spells that last for minutes are usually caused by transient ischemic attacks (TIAs) or migraine; and spells that last for hours are usually from Ménière disease.
Symptoms.
What the patient means by “dizziness” should be expanded on. Dizziness is an imprecise term used to describe a variety of symptoms including vertigo, disequilibrium, light-headedness, floating, and rocking, each of which has a different pathophysiologic mechanism and significance (Table 18-2).
TABLE 18-2. Symptoms | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Vertigo.
Vertigo is the illusion of movement (rotation, linear movement, or tilt) and is caused by a sudden imbalance of tonic neural activity in the vestibular nucleus. It may be caused by either normal head movements or disease in the labyrinth, eighth nerve, vestibular nucleus, vestibular cerebellum (nodulus and flocculus), or central otolith pathways (from the medial longitudinal fasciculus to the interstitial nucleus of Cajal). The causes of vertigo may be divided into those lesions that cause a mechanical problem to the inner ear (e.g., BPPV), and those that cause loss of function (ablation) of the inner ear or central pathways (e.g., vestibular neuritis).
Disequilibrium.
This is an imbalance or unsteadiness while standing or walking. It is caused by a variety of factors including diminished or double vision, loss of vestibular function, defects in proprioception from peripheral neuropathy or spinal cord lesions, defects in motor function from central nervous or peripheral nervous system abnormalities, joint pain or instability from arthritis or weakness, and psychological factors.
Light-headedness.
Also called presyncope, light-headedness usually is related to a momentary decrease in blood flow to the brain.
Floating, Swimming, Rocking, and Spinning Inside of Head.
These frequently are symptoms of psychological disorders, which include anxiety (panic attacks, agoraphobia, obsessive-compulsive disorder), somatiform disorders (including conversion), and depression.
Oscillopsia.
This is the subjective illusion of visual motion. Patients with acquired nystagmus (e.g., acute vestibular neuritis) report apparent motion of the visual scene caused by movement of the retina (retinal slip). Patients occasionally interpret oscillopsia as dizziness, although it differs from true vertigo in that it only occurs with the eyes open. Patients with congenital nystagmus usually do not report. Another form of oscillopsia occurs in patients with severe, bilateral loss of the VOR, which is frequently caused by ototoxicity from aminoglycosides. This form of oscillopsia occurs only during head movements and is caused by the lack of stabilizing features of the VOR; it is sometimes referred to as head-induced oscillopsia to differentiate it from oscillopsia caused by spontaneous nystagmus.
Circumstance.
The circumstances under which dizziness occurs should be obtained. When vertigo occurs without provocation (spontaneously), it is usually due to an acute imbalance in vestibular tone. When dizziness is provoked only by certain movements, such as standing up after reclining for at least 10 minutes, it is due to orthostatic hypotension. If vertigo occurs when the head is moved into certain vertical head positions (lying down or sitting up), it is due to BPPV.
Medications.
Several medications may cause dizziness, especially in patients older than 65 years of age.5,6 Table 18-3 lists common medications and their primary effects. Certain drugs cause disequilibrium and light-headedness. Sensitization to meclizine and scopolamine may occur after a few days of continuous use, and withdrawal symptoms occur when the medication is discontinued; this may be misinterpreted as a recurrence of the disorder itself, so physicians should be cautious about restarting these medications. It is suggested that meclizine, scopolamine, and other vestibular suppressants be used for only a few days during acute vestibular hypofunction caused by vestibular neuritis or labyrinthitis. These drugs should then be discontinued because they interfere with central compensation within the denervated vestibular nucleus. Patients with brainstem medullary lesions may have nausea lasting for weeks and may require medication for a longer time. Certain drugs may cause vestibular ototoxicity and spare hearing, yet lead to disequilibrium. These include certain aminoglycosides (streptomycin, gentamicin, tobramycin) and cisplatin.
TABLE 18-3. Drug-Induced Dizziness | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Office Examination
Eye Movements.
Vestibulo-ocular Reflex.
There are three bedside tests of the VOR (Table 18-4). The vestibular dynamic visual acuity test compares static acuity with the head still to dynamic acuity with the head moving. First, distance visual acuity is measured using a visual acuity chart. The patient is then asked to read the smallest possible line on the chart while the examiner manually oscillates the patient’s head horizontally at 2 Hz, with the head moving 1 to 2 inches in each direction; this is greater than the frequency at which smooth eye movements pursuit can track a target. If the VOR is normal, the patient’s eyes move smoothly in the opposite direction of the head such that ocular fixation is always maintained. The patient should be able to read the same line that was readable when his head was still, or the adjacent line with larger letters. If the patient can read only letters three lines or more above his initial static visual acuity, and there is no other ocular motility defect (nystagmus, misalignment, internuclear ophthalmoparesis, ocular motor paresis), the patient most likely has a vestibular defect. Second, VOR is examined using head thrust. Have the patient fixate on a target and observe the eyes after passive horizontal head thrusts. After a head thrust, an observed refixation saccade indicates decreased VOR.7 Third, determine whether head-shaking nystagmus is present. Have the patient close his eyes, pitch the head down 30 degrees, and then oscillate the head 20 times horizontally. Elicitation of nystagmus after this procedure indicates a vestibular imbalance.8 Head-shake nystagmus is best elicited when fixation is blocked with Frenzel glasses (20- to 30-diopter lenses) or video infrared goggles. This sign may persist indefinitely after a peripheral or central unilateral vestibular lesion.
TABLE 18-4. Bedside Tests of the Vestibulo-Ocular Reflexes | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
In very young children and babies, VOR can be assessed by picking up the child and rotating her in outstretched arms while observing the eyes for nystagmus. During this test, visual fixation should be blocked by having the patient wear Frenzel glasses to prevent the optokinetic response.
Smooth Pursuit and Vestibulo-ocular Reflex Cancellation.
The patient is asked to track a slowly moving target, both horizontally and vertically, with the head still (smooth pursuit) and with the head moving synchronously with the target (VOR cancellation). Lesions in the parieto-occipital cortex, pons, and cerebellum cause deficits in smooth pursuit (catch-up saccades are observed) and VOR cancellation (inappropriate VOR) for targets moving toward the side of the lesion.
Nystagmus.
Selective lesions in the peripheral and central vestibular pathways result in spontaneous nystagmus because of the unopposed higher spontaneous neural activity in the intact vestibular pathways (Table 18-5). For example, vestibular neuritis on one side results in peripheral vestibular nystagmus because of the unopposed activity of the anterior and horizontal SCCs on the intact side. These two SCCs project to the medial vestibular nucleus. Dorsolateral medullary lesions (Wallenberg syndrome) result in torsional nystagmus caused by involvement of the anterior and posterior SCC pathways centrally on one side.9 The presence of spontaneous nystagmus should be assessed with and without fixation because peripheral causes of nystagmus usually can be suppressed with fixation, whereas central causes cannot be suppressed. An easy way to test this is during the ophthalmoscopic examination, with the other eye fixating on a target.16 During this procedure, the fixating eye can be covered with the hand.
TABLE 18-5. Spontaneous Vestibular Nystagmus Due to Peripheral and Central Lesions | |||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


