(1)
Department of Ophthalmology and Visual Sciences, University of Iowa Hospitals and Clinics, Iowa City, IA, USA
The central retinal artery (CRA) is the primary source of blood supply to the retina. A detailed discussion of it is essential for an understanding of the various aspects of CRA occlusion (CRAO). Though the CRA is of vital importance, its anatomy has been the subject of much controversy. A review of the literature reveals a striking lack of unanimity in the views of different workers [1–10]. Much of this confusion seems to be due to attempts to cover endless variations by rigid and dogmatic statements. Moreover, the number of specimens examined in each series has been rather small. It is also necessary to remember that the anatomical results from blood vessels depend upon the efficiency and completeness of the injection. I conducted a detailed, comprehensive anatomical study on various aspects of the CRA in 106 human specimens – in 100 specimens by injection with liquid neoprene latex and 6 by serial sectioning of the part of the optic nerve containing the CRA; this constituted the largest number of CRA specimens studied. The findings of that study are described in detail elsewhere [11–13]. This study showed that no two examples (even from the two eyes of the same person) wholly agreed in their pattern of origin, course, branches, distribution, and anastomoses; this means that any dogmatic ruling is likely to lead to error. The following discussion primarily represents a brief account of the findings of my study [11–13], with review of the relevant literature.
Origin
Source of Origin
All the authors who investigated the anatomical features of the CRA described the ophthalmic artery, a branch of the internal carotid artery, as the source of origin of the CRA. In my study [11, 12], the CRA was a branch of the ophthalmic artery, irrespective of whether the latter was a branch of the internal carotid artery (Figs. 2.1b–e, 2.2, 2.3, and 2.4) or, rarely, of the middle meningeal artery (Figs. 2.1f, g, 2.5, and 2.6). Of six specimens, where the main source of blood supply to the ophthalmic artery was the middle meningeal artery, in four there was also a small trunk connecting the internal carotid artery to the main ophthalmic artery (Figs. 2.1b–e, 2.5, and 2.6), and in the other two the connection between the initial part of the ophthalmic artery and the internal carotid artery was absent (Fig. 2.1f, g), so that the blood supply to the CRA was from the middle meningeal artery. Morandi et al. [14] described a case where the ophthalmic artery arose from the middle meningeal artery and was associated with CRAO, and they considered that such an unusual origin could be a factor for CRAO. My study did not bear out that speculation.
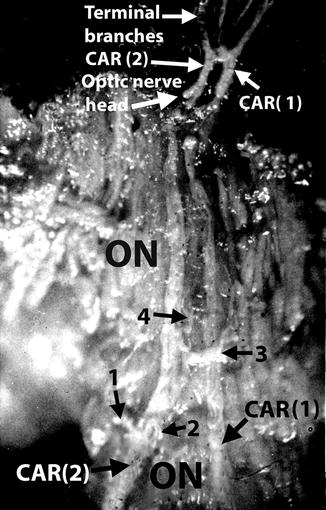
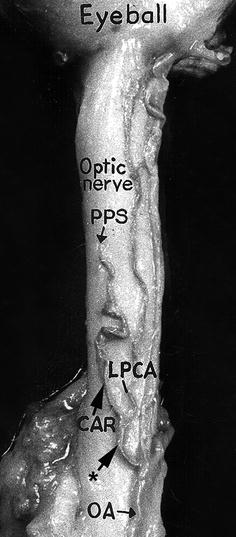
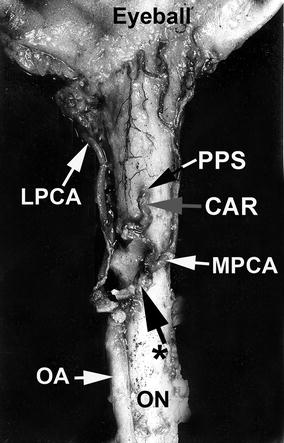
Fig. 2.1
Variations in origin and course of ophthalmic artery. (a) Normal pattern. (b–e) The ophthalmic artery arises from the internal carotid artery as usual, but the major contribution comes from middle meningeal artery. (f, g) The only source is the middle meningeal artery, as the connection with the internal carotid artery is either absent (f) or obliterated (g) (Reproduced from Singh (Hayreh) and Dass [12]). CAR central artery of the retina, ICA internal carotid artery, Lac. lacrimal artery, MMA middle meningeal artery, OA ophthalmic artery
Fig. 2.2
Two central arteries of the retina, CAR (1) and (2), of independent origin. The intraneural course and termination of the two arteries are shown, as seen on splitting open the optic nerve and eyeball. Branches (1, 2, 3, 4) from the intraneural course of CAR (2) are also seen (Reproduced from Hayreh [11]). CAR central artery of the retina, ON optic nerve
Fig. 2.3
The central artery of the retina arising by a common trunk with lateral posterior ciliary artery from the ophthalmic artery, as seen from inferior surface of the optic nerve (Reproduced from Hayreh [11]). CAR central retinal artery, LPCA lateral posterior ciliary artery, OA ophthalmic artery, PPS point of penetration into the sheath by CAR, * common trunk of origin of CAR and LPCA
Fig. 2.4
The central artery of the retina and medial posterior ciliary artery arising by a common trunk from the ophthalmic artery, as seen from below (Reproduced from “Hayreh [11]”). CAR central artery of the retina, LPCA lateral posterior ciliary artery, MPCA medical posterior ciliary artery, OA ophthalmic artery, ON optic nerve, PPS point of penetration into the sheath by CAR, * common trunk of origin of CAR and MPCA
Fig. 2.5
The central artery of the retina and medial posterior ciliary artery arising by a common trunk from the ophthalmic artery, as seen from below (Reproduced from Hayreh [11]). CAR central artery of the retina, Col. Br. collateral branch, LPCA lateral posterior ciliary artery, MPCA medical posterior ciliary artery, OA ophthalmic artery, ON optic nerve, PPS point of penetration into the sheath by CAR, * common trunk of origin of CAR and MPCA
Fig. 2.6
The origin and intraorbital course of the central artery of the retina, as seen from below. The ophthalmic artery arises from the internal carotid artery as usual, but the major contribution comes from middle meningeal artery (see Fig. 2.1d) (Reproduced from Hayreh [11]). CAR central artery of retina, ICA internal carotid artery, LPCA lateral posterior ciliary artery, MMA middle meningeal artery, OA ophthalmic artery, ON optic nerve, PPS point of piercing optic sheath
Number of CRAs
In my study [11, 12], two specimens had two CRAs, each arising independently from the ophthalmic artery (Fig. 2.2). That had not been previously reported. In one of these specimens, the two CRAs pierced the sheath of the optic nerve 12 mm and 5 mm behind the eyeball on its lower lateral aspect and ran independently up to the optic disc. At the optic disc the two joined to form a loop, from the summit of which arose terminal branches which followed the usual course (Fig. 2.2). In the other specimen, the two arteries united to form one trunk at the point of entry into the sheath of the optic nerve.
Site of Origin from the Ophthalmic Artery
According to Meyer [1] and Kershner [4], the CRA branches from the ophthalmic artery, while the latter is still within the sheath of the optic nerve at the apex of the orbit. Sudakevitch [5] reported that the artery may arise anywhere along the first part of the ophthalmic artery and very rarely distal to this point.
Order of Origin from the Ophthalmic Artery
The order and site of origin of CRA from the ophthalmic artery in my study [11, 12] is summarized in Table 2.1. The CRA was described by Tsutsumi and Rhoton [15] as the first branch of the ophthalmic artery in 67 % and the second branch in 28 % and by Kocabiyik et al. [16] the third branch in 5 % and the first branch in 93.3 %.
Table 2.1
Site, order, and mode of origin of CRA from the ophthalmic artery
Origin | Total incidence | Ophthalmic artery crosses | ||
|---|---|---|---|---|
Over optic nerve | Under optic nerve | |||
Site | From the first part of the ophthalmic artery | 22.12 | 20.20 | 1.92 |
From the angle of the ophthalmic artery | 57.69 | 51.92 | 5.77 | |
From the second part of the ophthalmic artery | 18.27 | 4.81 | 13.46 | |
From the third part of the ophthalmic artery | 1.92 | – | – | |
Order | As the first branch of the ophthalmic artery | 77.45 | 74.51 | 2.94 |
As the second branch of the ophthalmic artery | 18.63 | 2.94 | 15.69 | |
As the third branch of the ophthalmic artery | 3.92 | 0.98 | 2.94 | |
Mode | As the independent branch | 37.50 | 21.15 | 16.35 |
With the medial posterior ciliary artery | 37.50 | 33.65 | 3.85 | |
With the lateral posterior ciliary artery | 11.54 | 11.54 | Nil | |
With the MPCA, LPCA, and muscular artery | 1.92 | 1.92 | Nil | |
With the MPCA and LPCA | 4.81 | 4.81 | Nil | |
With the MPCA and muscular artery | 2.88 | 1.92 | 0.96 | |
With the muscular artery | 2.88 | 2.88 | Nil | |
With the lacrimal artery and LPCA | 0.96 | 0.96 | Nil | |
Total number of specimens examined | 102 | 78.43 % | 21.57 % | |
Mode of Origin from the Ophthalmic Artery
This was described differently by various authors. The CRA has been described as arising as an independent branch [4, 9, 15] and in common with the posterior ciliary artery [2, 4, 15], medial posterior ciliary artery [1, 2, 5, 9], and lateral posterior ciliary artery [9]. Modes of origin of CRA from the ophthalmic artery in my study [11, 12] are summarized in Table 2.1. In Fig. 2.3, the CRA arises from the ophthalmic artery in common with the lateral posterior ciliary artery and in Figs. 2.4 and 2.5 in common with the medial posterior ciliary artery.
Course
No detailed description is available in the literature about the course of the CRA. For descriptive purposes the whole course of the CRA may be divided into three distinct parts.
Intraorbital Part
This is from its origin from the ophthalmic artery till it pierces the optic nerve sheath. In my study [11, 12], in most specimens the CRA had a tortuous intraorbital course (Figs. 2.2, 2.3, 2.4, 2.5, 2.6, and 2.7). This tortuosity was particularly marked near the point of entry into the dural sheath, and in this locality the coils of the artery are usually fixed to each other by thin fibrous sheets. In 90 % of specimens this part lay free in fatty areolar tissue around the optic nerve, lightly adherent to the sheath of the nerve, and in 6 % embedded in the folds of the dura beneath the optic nerve. In 4 % it was adherent only near the site of entry into the sheath for a millimeter or so and was free more proximally. Sometimes the CRA is surrounded in its intraorbital course by a thick plexus of veins derived from the dural sheath and central retinal vein. Tsutsumi and Rhoton [15] stated that the diameter of the CRA at its origin from the ophthalmic artery averaged 0.4 mm (range, 0.3–0.6 mm). According to Kocabiyik et al. [16], the mean diameter of the CRA was 0.47 ± 0.05 mm on the right side and 0.46 ± 0.04 mm on the left side.
Fig. 2.7
The origin and intraorbital course of the central artery of the retina, as seen from below. The ophthalmic artery arises from the internal carotid artery as usual, but the major contribution comes from middle meningeal artery (see Fig. 2.1e) (Reproduced from Hayreh [11]). CAR central artery of retina, ICA internal carotid artery, LPCA lateral posterior ciliary artery, MPCA medial posterior ciliary artery, OA ophthalmic artery, ON optic nerve, PPS point of piercing optic sheath
Site of Penetration of the Dural Sheath by the CRA
There is a good deal of difference of opinion about this among various investigators. It has been stated that the CRA pierces the dural sheath at the inferior medial aspect of the optic nerve [4, 10, 16–18]. According to Deyl [17], during development, this is the site of the embryonic optic fissure where the mesenchyme invaginates the primary optic vesicle to form the vitreous, and it thus appears that the CRA maintains its primitive position. This site was observed in my study [11, 12] in 86 % (Figs. 2.3 and 2.6). Contrary to this view, Vossius [20] thought that the artery pierced the sheath on its lower lateral aspect, believing that during development the nerve and eyeball rotated through a 90° angle; this site was observed in 13 % of my series (Fig. 2.5) [11, 12]. Surprisingly, Beauvieux and Ristitch [3] found the site of penetration on the superior surface of the optic nerve in 20 % of their 20 specimens, but this site was never seen in my study [11, 12]. In 1 % of my study [11, 12], the site of penetration was observed on the lateral side of the optic nerve. According to Tsutsumi and Rhoton [15], the CRA penetrated the lower surface of the optic nerve sheath at or near the midline in 70.6 %, the inferolateral surface in 6.4 %, and the inferomedial part in 21.1 %.
The distance of penetration of the sheath behind the eyeball by different authors has also been described differently by different authors; for example, it was 5–15 mm by Whitnall [21], 10–15 mm by Wolff [22], 15 mm by Wybar [9], 7–17 mm by Steele and Blunt [10], 8–15 mm by Kang et al. [23], and 4–20 mm by Tsutsumi and Rhoton [15]. Kocabiyik et al. [16] described the distance as 10.90 ± 2.09 mm (range 7–14.7) on the right side and 10.35 ± 2.52 mm (range 6.4–15.2) on the left side. In my study [11, 12], it varied between 5 and 15.5 mm (median 10 mm, mean 9.8 ± 1.8 mm) behind the eyeball.
According to Beauvieux and Ristitch [3], the CRA pierces the sheath obliquely, running upward and forward within the sheath for about 1 mm before entering the intravaginal space. That was also the case in my study [11, 12], the CRA invariably traversing the sheath obliquely upward and forward, remaining within the substance of the sheath for 0.3–1.5 mm (Figs. 2.8 and 2.9a, b).
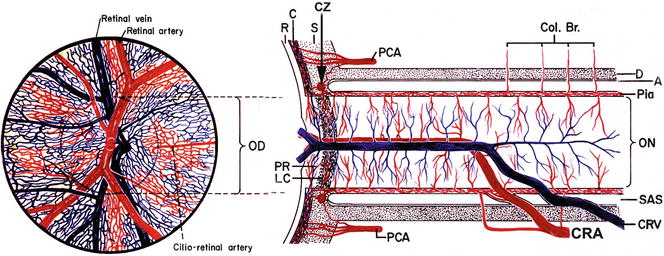
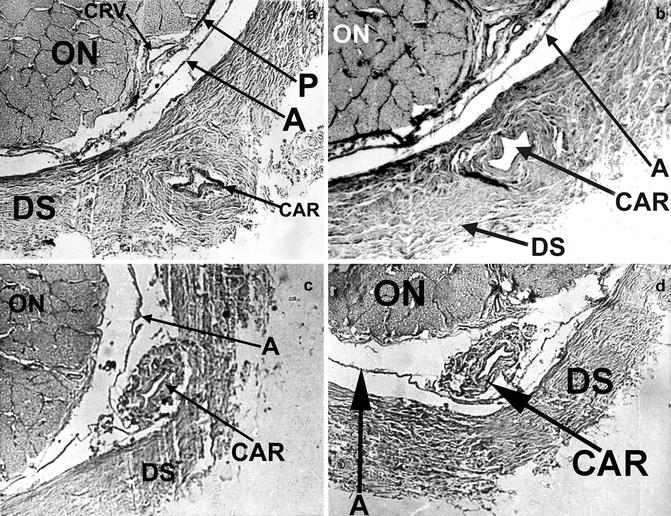
Fig. 2.8
Schematic representation of the course and branches of the central artery and vein of the retina (Modified from Hayreh [24]). A arachnoid, C choroid, CRA central retinal artery, Col. Br. collateral branches, CRV central retinal vein, CZ circle of Haller and Zinn, D dura, LC lamina cribrosa, OD optic disc, ON optic nerve, PCA posterior ciliary artery, PR prelaminar region, R retina, S sclera, SAS subarachnoid space
Fig. 2.9
Four transverse sections of the optic nerve showing the various stages in the penetration of the central artery of the retina from intraorbital part to intravaginal part. Central artery of the retina: (a) starting to pierce the dural sheath of the optic nerve, (b) lying within the substance of the dural sheath, (c) lying in subdural space, and (d) lying in subarachnoid space (Reproduced from Hayreh [11]). A arachnoid, CAR central artery of the retina, CRV central retinal vein, DS dural sheath of the optic nerve, ON optic nerve, P pia
Intravaginal Part
This part lies between the points where the CRA has pierced the dural sheath of the optic nerve and the nerve itself. In my series [11, 12], the existence of distinct subarachnoid and subdural spaces was clearly seen in the reconstructions of serial sections (Figs. 2.9c, d). In its intravaginal course, the artery usually runs forward for a short distance in the subdural space (Fig. 2.9c) and for a much greater distance in the subarachnoid space (Figs. 2.9d, 2.10, 2.11, and 2.12). The artery carries a prolongation from the dura, and it also carries from the arachnoid a tubelike prolongation, which surrounds it in the subarachnoid space. The intravaginal part of the artery is usually 0.9–2.5 mm long. The artery may be accompanied by the central retinal vein; although this was described as invariable by some [3, 4], it was found in only 8 out of the 14 of my specimens [11, 12] in which the vein could be studied. In 8 % of the specimens, the CRA formed a tortuous loop in its intravaginal course (Fig. 2.12), and in such cases the intravaginal part was much longer than usual. In 1 % the artery looped and ran backward.
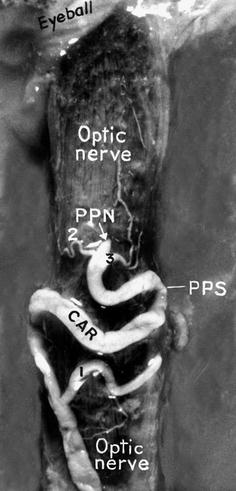
Fig. 2.10
Origin, intraorbital, and intravaginal course of the central artery of the retina and its pial branches, as seen from below. Its intraneural course is shown in Fig. 2.31 (Reproduced from Hayreh [11]). CAR central artery of retina, DS dural sheath of the optic nerve, IV part intravaginal part of the CAR, LPCA lateral posterior ciliary artery, ON optic nerve, PPN point of piercing the optic nerve, PPS point of piercing DS
Fig. 2.11
Origin, intraorbital, and intravaginal course of the central artery of the retina and its branches and circle of Haller and Zinn, as seen from below (Reproduced from Hayreh [11]). CAR central artery of retina, CZ circle of Haller and Zinn, DS dural sheath of the optic nerve, IO intraorbital part of the CAR, IV intravaginal part of the CAR, LPCA lateral posterior ciliary artery, OA ophthalmic artery, ON optic nerve, PPN point of piercing the optic nerve, PPS point of piercing optic sheath
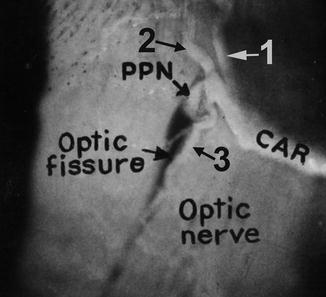
Fig. 2.12
Origin, intraorbital, and intravaginal course of the central artery of the optic nerve and its branches, as seen from below (Reproduced from Hayreh [11]). CAR central artery of the retina, PPN point of piercing the optic nerve, PPS point of piercing dural sheath
Intraneural Part
This lies in the optic nerve. In my study [11, 12], the artery entered the optic nerve in a well-defined fissure on the inferior surface of the optic nerve anterior to the site of penetration into the dural sheath (Figs. 2.13, 2.14, and 2.15) and carried a fold of pia with it (Fig. 2.16). The site of entry into the nerve was always 1.2–3.5 mm anterior to the site of penetration into the dural sheath (Figs. 2.8, 2.10, 2.11, and 2.12), except in one specimen in which it was situated 4 mm posteriorly. The intraneural part of the CRA has two distinct sections – vertical and horizontal (Figs. 2.8 and 2.17). In my study [11, 12], the initial vertical part reached the center of the nerve by running upward and slightly forward in 89 % (Figs. 2.8 and 2.17), vertically upward in 8 %, and upward and backward in 3 %. The transition from the vertical to the horizontal parts was gradual, no sharp angle being formed at this point. In the specimens with two trunks of the CRA, the vertical part was missing, and the two trunks ran straight to the optic disc from their point of penetration into the nerve (Fig. 2.2). The horizontal part runs forward horizontally in the center of the optic nerve and lamina cribrosa to reach the optic disc, where it divides into its terminal branches (Fig. 2.8). Magitot [2] and Beauvieux and Ristitch [3] reported that the artery was surrounded in this part by vascular fascia which gradually diminished and came to an end just at the point of entry of the artery into the eyeball. In my serial sectioning study [11, 12], the artery was enclosed in a fibrous tissue envelope, which in turn was continuous with the fibrous septa of the optic nerve (Fig 2.18). The artery was loose inside this envelope, the surrounding space being visible on dissection (Fig. 2.18). No such space was seen around the central retinal vein, which lay beside the artery on the lateral side and was also enclosed in a fibrous envelope. The two vessels may lie in close apposition (Figs. 2.18a, b), or they may be separated by fibrous tissue (Figs. 2.18c, d), and at places even nervous tissue may intervene. I found that it was not essential for the CRA to travel in the center of the optic nerve to reach the lamina cribrosa. In one specimen the vertical section was virtually absent, so that the artery ran straight to the center of the lamina cribrosa from its point of penetration into the nerve; the central retinal vein, however, occupied the usual position at the center.