FIGURE 41.1 The temporoparietal fascia is a superficial vascularized tissue flap that is located immediately deep to the subcutaneous tissue of the scalp. The temporalis muscle is found deep to the temporalis muscle fascia.
Like the TPFF, the TMF is a reliable, myofascial flap that was also described more than a century ago. The vascular supply is the deep temporal artery, which originates from the internal maxillary artery (Fig. 41.2). The temporalis muscle lies deep to the temporoparietal fascia. It is a broad, radiating muscle that arises from the temporal fossa and from the deep surface of the temporal fascia. Its fibers converge inferiorly to form the tendon, which passes deep to the zygomatic arch and inserts into the medial surface of the coronoid process. The flap can be raised up and pedicled only on the coronoid process. This improves the arc of rotation to reach the paramedian aspect of the skull base.
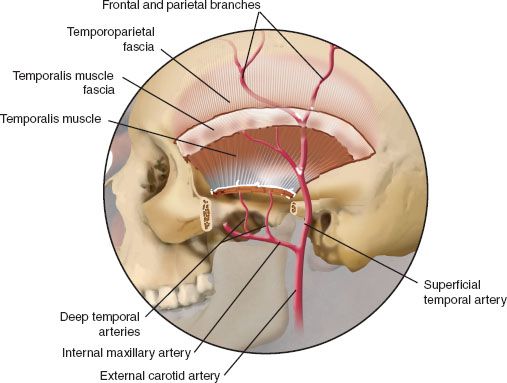
FIGURE 41.2 The vascular supply to the TPFF is the superficial temporal artery and vein; however, the vascular supply to the TMF is the deep temporal artery derived from the internal maxillary system.
I find that these flaps provide an excellent source of well-vascularized tissue that can be used for skull base reconstruction. They are reliable, and the donor site is well tolerated.
HISTORY
There are several important issues that must be considered when taking a history. The first relates to prior surgery. The advantage of the TPFF and the TMF is that they are often preserved in spite of prior surgery. As part of the history, it is important to determine if the patient has had prior cranial base surgery that may have compromised the pericranial flap. In such a case, the TPFF or TMF may be used for reconstruction of the lateral skull base. A careful history will often determine if the pericranial flap has been previously used for reconstruction. A second aspect of the history relates to the blood supply of these two flaps. The TPFF receives its blood supply from the superficial temporal artery and vein. In contrast, the TMF receives its blood supply from the deep temporal artery and vein. In the former case, if the external carotid artery has previously been ligated, the TPFF will not be viable. In the latter case, if the internal maxillary artery has been previously sacrificed, then the blood supply to the TMF will be compromised. A history of previous trauma to the donor site should be sought.
PHYSICAL EXAMINATION
The physical examination should be directed toward an evaluation of the external carotid artery and the lateral skull base region. Evidence of scarring or prior surgery should be carefully noted to determine if there has been a compromise in the blood supply to the temporalis muscle or temporal parietal fascia. Physical examination should also include a careful evaluation of the defect. While both the temporal parietal and the temporalis flaps are well vascularized, the arc of rotation and reach to the midline is limited. Both flaps are ideal for lateral temporal bone and lateral cranial base defects; however, they are not well suited for medial defects of the cranial base.
INDICATIONS
The indications for the TPFF and TMF are for defects of the lateral skull base. The TPFF is a well-vascularized flap that is ideal for reconstitution of defects of the dura. In contrast, the TMF is bulky but well vascularized. I tend to use the TPFF in cases where dural reconstruction is required. I reserve the TMF for defects that require restoration of bulk.
CONTRAINDICATIONS
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


