Purpose
To describe 3 patients with chronic mucopurulent conjunctivitis found to have an unrecognized sequestration of bacteria within tarsoconjunctival crypts of the upper eyelid.
Design
Review of 3 noncomparative cases.
Methods
settings: Institutional. study population: Three consecutive patients with tarsoconjunctival crypts. intervention procedure: Marsupialization of the individual crypts. main outcome measures: Resolution of chronic discharge and resolution of signs and symptoms.
Results
One patient with Stevens-Johnson syndrome and 2 patients with floppy eyelids had chronic mucopurulent conjunctivitis that was refractory to multiple medical and surgical interventions. Retention of a yellowish coagulum within the fistulous tracts of the tarsal conjunctiva was the site of pathologic features in all patients. The diagnosis was confirmed by squeezing out of the coagulum from the fistulous tracts by pinching the eyelid horizontally. Pseudomonas aeruginosa was isolated in 1 patient and Staphylococcus aureus was isolated in the other 2 patients. A Bowman probe could be passed through the fistulous opening to unveil the full extent of the conjunctival tunnels on the epitarsal surface. Each tract was marsupialized, and no relapse was found during a follow-up period of 12 to 96 months.
Conclusions
Patients with chronic, relapsing, purulent conjunctivitis should have their upper eyelid everted to search for tarsoconjunctival crypts as the source of bacteria-laden coagulum. The formation of the crypts is likely the result of tarsal conjunctiva trauma with lamellar de-epithelialization, followed by re-epithelialization to form an epithelialized tunnel as a potential space for harboring bacteria. Marsupialization of the crypts obliterates the potential space and is curative.
Chronic, unilateral conjunctivitis may be caused by nasolacrimal duct obstruction, chronic canaliculitis, conjunctival intraepithelial neoplasia, sebaceous cell carcinoma, floppy eyelid syndrome, and giant fornix syndrome. Rose described the giant fornix syndrome as a chronic, relapsing, purulent conjunctivitis that often was unilateral and lasted between 8 and 48 months. He postulated that the gradual deepening of the superior fornix was the result of age-related levator aponeurosis disinsertion, which permitted the accumulation of a bacteria-laden protein coagulum within a capacious superior fornix. The retained purulent material leads to persistent reinoculations of the tear lake by low-grade bacteria, despite repeated courses of topical antibiotics.
We describe 3 patients with signs that were similar to the giant fornix syndrome. They also had chronic mucopurulent conjunctival discharge that was refractory to multiple courses of antibiotic therapy. Although the superior forniceal space is the site of involvement in patients with giant fornix syndrome, the anatomic sources of the persistent purulent discharge in our patients were the fistulous tracts within the upper eyelid tarsal conjunctiva. We have termed this condition tarsoconjunctival crypts . The clinical features of this previously unrecognized condition, proposed mechanism of pathogenesis, and a surgical technique for the resolution of the condition are presented.
Methods
Case 1
A 52-year-old woman had contact lens intolerance, foreign body sensation, erythema, and mucoid discharge from both eyes that began 10 months after Stevens-Johnson syndrome had developed. Over the next 4 years, she was seen by several ophthalmologists, all of whom attributed her symptoms to keratoconjunctivitis sicca. Punctual cautery to both lower lid puncta was performed without significant benefit. Multiple topical therapies were attempted, but failed to resolve her symptoms. Medications included methylprednisolone 1%, loteprednol etabonate, fluorometholone acetate, solcoseryl, saline, artificial tears, autologous serum tears, vitamin A, and acetylcysteine 5% and 10%. Culture of the discharge revealed Pseudomonas aeruginosa . Topical antibiotic therapies prescribed included ocufloxacin, tobramycin, gentamicin, polymyxin B, fusidic acid, and combined hydrocortisone, neomycin, and polymyxin. Additionally, the patient received oral tetracycline, doxycycline, levofloxacin, and ciprofloxacin, as well as a 14-day course of intravenous ticarcillin disodium and clavulanate potassium; however, she continued to have persistent mucoid discharge.
The patient was referred to the Oculoplastic Service for evaluation of the lacrimal drainage system as a potential occult source of the persistent discharge. The lacrimal system was noted to be patent; however, eversion of the right upper eyelid revealed scarring with papillary changes of the tarsal conjunctiva. At the initial examination, there was no hint of a sequestered coagulum under the scarred conjunctiva or obvious fistulous openings ( Figure 1 , Top left). However on squeezing the tarsal plate horizontally, mucoid material exuded from the tunnels, revealing several pinpoint fistulous openings on the tarsal conjunctiva. A Bowman probe was passed through the fistulous opening to unveil the full extent of the conjunctival tunnels on the epitarsal surface ( Figure 1 , Top right).
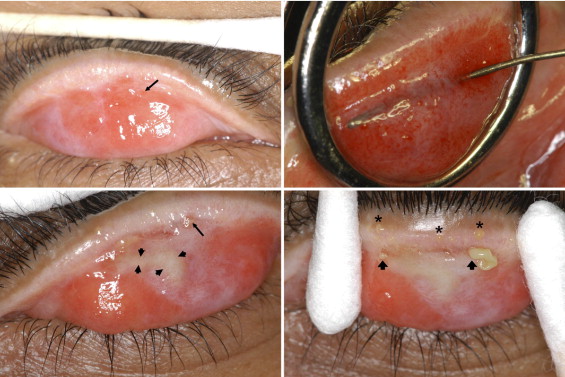
The anatomic findings were similar in the left upper eyelid ( Figure 1 , Bottom left). Discovery of the fistulous openings of these tracts was possible only by the fortuitous buckling of the tarsal plate to extrude the sequestrum. The color and texture of the oil droplets exuded from the meibomian gland openings was quite different from the thicker exudate expressed from the crypts ( Figure 1 , Bottom right). Similar tarsoconjunctival tracts with retained yellowish exudates were noted on the epitarsal surface of both lower eyelids, but these were much less severe.
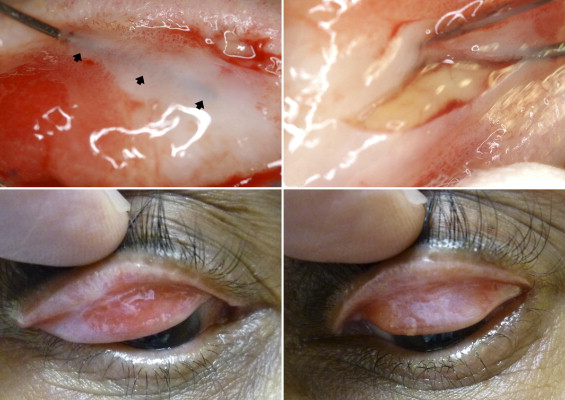
The patient underwent marsupialization of the left upper and lower eyelid tarsoconjunctival crypts. A Bowman probe was passed into each tract and a no. 11 Bard-Parker blade was used to incise the tissue over the metal probe ( Figure 2 , Top left). The coagulum within the tract was evacuated using a fine chalazion curette ( Figure 2 , Top right). After surgery, the patient was placed on a course of topical ciprofloxacin, and her symptoms of chronic mucous discharge resolved completely within 1 month. She subsequently underwent an identical procedure on the right upper and lower eyelids. Eight years after the marsupialization of the tarsoconjunctival crypts, the patient has remained free of mucous discharge ( Figure 2 , Bottom left and right).
Case 2
An 83-year-old man with a history of peripheral ulcerative keratitis in his right eye was treated at another eye clinic for several years for ipsilateral recurrent, purulent discharge. Cultures obtained from the discharge revealed methicillin-sensitive Staphylococcus aureus . The patient was treated with oral doxycycline and topical gatifloxacin and prednisolone acetate eye drops. After failing to respond to this treatment regimen, a diagnosis of giant fornix syndrome was made. The patient was switched to a new treatment regimen consisting of oral ciprofloxacin, combined polymyxin B and trimethoprim, prednisolone acetate eye drops, and lavage of the superior fornix with povidone–iodine every other day. After 4 months of treatment, the patient’s discharge and tearing had improved, and culture results were negative. All antibiotics were discontinued, but within 1 week, copious conjunctival discharge returned. Oral ciprofloxacin was resumed and topical tobramycin was initiated.
The patient was seen by another physician who noted bilateral lagophthalmos, lower lid laxity, and floppy eyelids. Discharge was present in the right upper and lower punctum, and mucous was expressed from the right superior canaliculus. The nasolacrimal drainage system irrigated freely through the inferior punctum. Reculture of the discharge again revealed methicillin-sensitive S. aureus . Tobramycin and ciprofloxacin were replaced with topical combined bacitracin and polymyxin B and combined oral trimethoprim and sulfamethoxazole without clinical improvement. A right inferior canaliculotomy was performed based on the pouty appearance of the punctum; no concretions or foreign bodies were found. After surgery, the patient continued combined oral trimethoprim and sulfamethoxazole and was switched to topical combined neomycin, polymyxin B, and dexamethasone ointment. After a 2-week quiescent period, the purulent discharge and epiphora returned.
The patient was referred to us for another opinion. In addition to the previously noted clinical findings of copious discharge, bilateral lower eyelid laxity, floppy right upper and lower eyelids, and a patent nasolacrimal system were found. The consultant also detected mild protective ptosis and lateral canthal tendon disinsertion. Eversion of the right upper lid showed intense papillary conjunctivitis and multiple tarsoconjunctival crypts in linear and spherical configurations with trapped mucopurulent material ( Figure 3 , Top). A cotton-tipped applicator could not wipe the mucoid material off the tarsal plate, indicating its subconjunctival location. Gentle pressure on the surface expressed the exudate from the epitarsal recesses through the punctate conjunctival openings. The left eye was unaffected ( Figure 3 , Bottom left).




