T
tabes dorsalis A degenerative disease of the posterior columns of the spinal cord, the posterior spinal roots and the peripheral nerves accompanied by a number of ocular signs and symptoms such as atrophy of the optic nerve, visual field defects, ptosis, Argyll Robertson pupil and paralysis of one or more of the extraocular muscles. The disease is a result of neurosyphilis.
TABO notation See axis notation, standard.
tachistoscope An instrument that presents visual stimuli for a brief and variable period of time (usually less than 0.1 s).
tacrolimus See immunosuppressants.
Talbot-Plateau law See law, Talbot-Plateau.
tamponade agent A gas, pad or silicone oil used to plug a cavity, stop a haemorrhage or compress a part. In the eye it may be employed in vitreous surgery to fill the vitreous space with either gas or silicone, and in retinal detachment therapy.
tangent scale See Maddox cross.
tangent screen See screen, tangent.
tangential focus See astigmatism, oblique.
tapetoretinal degeneration See degeneration, tapetoretinal.
tapetum lucidum A reflecting pigment layer lying behind the visual receptors of the retina of certain mammals (e.g. cats, dogs), birds and fish, which gives a shining appearance to the eyes when illuminated in the dark. The tapetum is located either in the pigment epithelium or in the choroid and covers either the whole fundus or more often only the upper and back portion. The role of the tapetum lucidum is to increase the probability of visual stimulation of the photoreceptors by reflecting light back after having already traversed them once, thus aiding vision in dim illumination. In some species the tapetum consists of guanine crystals.
target A pattern or an object of fixation such as a red dot or an optotype.
See optotype.
tarsal Pertaining to the tarsus.
tarsal gland See glands, meibomian.
tarsal muscles See muscles, Müller’s palpebral.
tarsal plate See tarsus.
tarsorrhaphy A surgical procedure consisting of suturing the upper and lower eyelids together either partially or completely. It provides a temporary protection to the eye or forms part of the treatment of dry eyes.
See alacrima; keratoconjunctivitis sicca.
tarsus Thin flat plate of dense connective tissue, situated one in each eyelid, which gives it shape and firmness. Each tarsus extends from the orbital septum to the eyelid margin. The upper tarsal plate, shaped like the letter D placed on its side, is much larger than the lower. Its width is 11 mm in the centre whereas the corresponding measurement in the lower tarsus, which is somewhat oblong in form, is 5 mm. Each tarsus is about 29 mm long and 1 mm thick. Within each tarsus are the meibomian glands, approximately 25 in the upper and 20 in the lower. Syn. tarsal plate.
See ligament, palpebral; orbital septum.
Tay’s choroiditis See drusen, familial dominant.
Tay–Sachs disease See disease, Tay–Sachs.
tear duct One of about a dozen ducts of the lacrimal gland. It originates in the orbital part of the gland, traverses the palpebral part of the gland and opens into the lateral superior fornix of the conjunctival sac. Syn. lacrimal duct.
See lacrimal apparatus.
tear exchange See lens, fenestrated.
tear film See film, precorneal.
tear film break-up test See test, break-up time.
tear film, prelens Tear film found on the front surface of a contact lens on the eye. The oily layer of the film is slightly thinner with soft lenses than in the precorneal film and almost absent with rigid lenses. The aqueous layer is thinner with rigid lenses than in the precorneal film. The exact composition of the prelens tear film varies with the characteristics of the contact lens on the eye.
See film, precorneal.
tear layer See film, precorneal.
tear meniscus A thin strip of tear fluid with concave outer surfaces at the upper and lower lid margins. It contains most of the exposed tear volume. The absence of a tear meniscus is an indication of a dry eye. Syn. marginal tear strip; lacrimal prism; tear prism.
See film, precorneal; lacrimal lake.
tear prism See tear meniscus.
tear pumping The mechanism involving blinking, which acts to bring fresh tears with oxygen and nutrients to the cornea behind a contact lens, and pumping stale tears containing carbon dioxide, lactic acid and other waste products from beneath the lens. It occurs most readily with hard contact lenses (between 14% and 20% of the tear volume is exchanged with each blink) and to a much smaller extent with soft lenses (between 1% and 5% of the tear volume is exchanged with each blink).
See hypoxia; oxygen transmissibility.
tear, retinal See retinal break.
tear secretion There are two types of tear secretion: (1) Basal (basic) tear secretion, which occurs normally without any stimulation. It maintains the cornea and conjunctiva continuously moist, but is reduced in dry eyes (e.g. keratoconjunctivitis sicca) and in elderly individuals. (2) Reflex tear secretion, which is produced in response to a corneal or conjunctival irritant and also depends on psychological factors. Basal secretion and reflex secretion are produced by the lacrimal gland and the accessory glands of Krause and Wolfring. The amount of tears secreted amounts to 14–33 g per 24 hours or 0.5–2.2 μl/minute, being about 2 μl/minute at 15 years of age and less than 1 μl/minute at 65 years of age. Note: it was formally thought that basal secretion was produced solely by the accessory glands and reflex secretion by the lacrimal gland but it is now thought that they all contribute to both forms of tear secretion.
See reflex, lacrimal; test, basic secretion; test, Schirmer’s.
tear stasis The slowing down or stoppage of tear flow behind a contact lens. It can lead to lens adherence (lens binding) to the cornea with the possible consequences of acute red eye, arcuate corneal staining, and, if severe, corneal ulceration. Fitting or refitting in such a way that some lens movement is maintained usually prevents this condition.
See lens adherence; staining, fluorescein.
tear strip, marginal See tear meniscus.
tearing reflex See reflex, lacrimal.
tears The clear watery fluid secreted by the lacrimal gland which, together with the secretions from the meibomian glands, the goblet cells, the gland of Zeis, as well as the accessory lacrimal glands of Krause and Wolfring, helps to maintain the conjunctiva and cornea moist and healthy. Periodic involuntary blinking spreads the tears over the cornea and conjunctiva and causes a pumping action of the lacrimal drainage system, through the lacrimal puncta into the nasolacrimal duct. Approximately 25% of the tears is lost by evaporation, the remaining 75% is pumped into the nasal cavity and over 60% of the tear volume is drained through the lower canaliculus. Tears contain water (98.2%), salts, lipids (e.g. wax esters, sterol esters, hydrocarbons, polar lipids, triglycerides and free fatty acids), proteins (e.g. lysozyme, lactoferrin, albumin, IgA, IgE, IgG, complement proteins C3, C4, C5 and C9, and beta-lysin), magnesium, potassium, sodium, calcium, chloride, bicarbonate, urea, ammonia, nitrogen, citric acid, ascorbic acid, and mucin. Tears have a pH varying between 7.3 and 7.7 (shifting to a slightly less alkaline value when the eye is closed) and the quantity secreted per hour is between 30 and 120 ml. Syn. lacrimal fluid.
See alacrima; blink; epiphora; film, precorneal; hyperlacrimation; keratoconjunctivitis sicca; lacrimal apparatus; lacrimal lake; lysozyme; mucin; staining, fluorescein; test, break-up time; test, non-invasive break-up time; test, phenol red cotton thread; test, Schirmer’s.
artificial t. Any eye drop solution that can replace tears by approximating its consistency in terms of viscosity and tonicity and may contain many of the substances found in tears. The most common agents found in artificial tears are cellulose derivatives, such as methylcellulose, hydroxymethylcel-lulose, hydroxypropylcellulose, hypromellose (hydroxypropylmethylcellulose), hydroxyethylcellulose, and polyvinyl alcohol, povidone (polyvinyl pyrrolidine), sodium hyaluronate and sodium chloride, which have low viscosity. Carbomer (polyacrylic acid), carmellose (carbomethylcellulose), liquid paraffin and yellow soft paraffin have medium to high viscosity. Acetylcysteine, a mucolytic agent prepared with hypromellose is used when the tear deficiency is associated with threads and filaments of mucus to soften and make the mucus more fluid, as well as shrinking the mucous membranes (astringent). Syn. ocular lubricant.
See alacrima; corneal erosion, recurrent; ectropion; eye, dry; hypromellose; keratoconjunctivitis sicca; methylcellulose; palsy, Bell’s; wetting solution; xerophthalmia.
crocodile t. Copious secretion of tears occurring during eating in cases of abnormal regeneration of the seventh cranial nerve after recovery from Bell’s palsy. Syn. paradoxic lacrimation.
Tearscope plus Trade name of a handheld instrument designed to view the tear film non-invasively. It uses a cold light source to minimize any drying of the tear film during the examination. It can be used directly in front of the eye or in conjunction with a slit-lamp biomicroscope to gain more magnification. Evaluation of the interference patterns of the anterior surface of the tear film lipid layer facilitates the diagnosis of the cause of dry eye symptoms, as well as screening patients for contact lens wear. The instrument also allows the measurement of the non-invasive break-up time.
See film, precorneal; test, non-invasive break-up time.
technique See method or test.
tectal midbrain syndrome See syndrome, Parinaud’s.
tectum of the mesencephalon Structure comprising the plate of grey and white matter (called the tectal lamina) that forms the roof of the midbrain and from which project the inferior and superior colliculi. The area anterior to it is called the pretectal region. Syn. tectum of the midbrain; optic tectum. Note: The word tectum comes from the Latin and means roof. The word mesencephalon is made up of two parts that come from the Greek and means middle brain.
See colliculi, inferior; colliculi, superior; fibres, pupillary; nystagmus, convergence-retraction; pathway, retinotectal; pretectum.
tectum of the midbrain See tectum of the mesencephalon.
teichopsia A transient, shimmering visual sensation. Example: the fortification spectrum of a scintillating scotoma.
telangiectasia A dilatation of small blood vessels (arterioles, capillaries, venules), often multiple in character. Telangiectasias create small red lesions, sometimes spidery in appearance, usually in the skin or mucous membranes, which blanch on pressure. They can develop into naevus flammeus (‘port-wine stain’), a birthmark found usually on the head or neck.
See syndrome, Sturge–Weber.
retinal t. See disease, Coat’s.
Telebinocular A trade name for a stereoscope based on that of Brewster–Holmes and used to investigate distance and near visual functions such as acuity, stereopsis, etc.
See stereoscope, Brewster’s.
telecanthus Excessive separation between the medial canthi of the eyelids. It may occur in isolation or form part of the blepharophimosis syndrome. Treatment consists in shortening and re-fixating the medial canthal tendons to the lacrimal crest.
See syndrome, blepharophimosis.
telecentric Pertains to an optical system in which its aperture stop is positioned so that the entrance pupil falls in the first focal plane, the exit pupil is at infinity, and the rays through the centre of the entrance pupil from all points on the object are parallel to the axis in the image space. Similarly, if the exit pupil lies in the second focal plane the entrance pupil will be at infinity, and the rays through the centre of the exit pupil will be parallel to the axis in the object space.
teleopsia Anomaly of visual perception in which objects appear to be much further away than they actually are. It may be due to vision in a hazy atmosphere, intoxication, neurosis, etc.
See metamorphopsia.
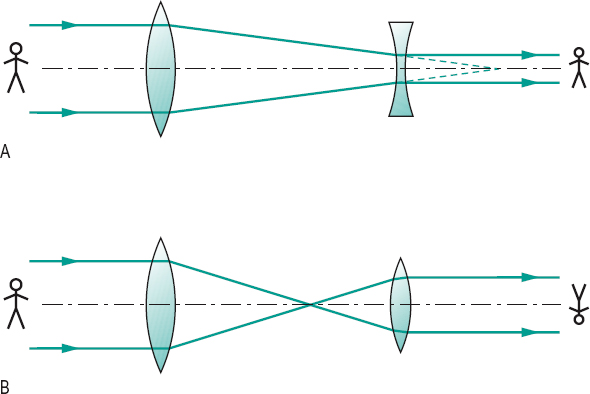
telescope An optical instrument for magnifying the apparent size of distant objects. It consists, in principle, of two lenses: (1) the objective, being a positive lens which forms a real inverted image of the distant object; (2) the eyepiece through which the observer views a magnified image of that formed by the objective. The eyepiece may be either positive (astronomical or Kepler telescope) or negative (galilean telescope). The magnification M of a telescope is given by the following formula

where f’o is the second focal length of the objective, fe the first focal length of the eyepiece, and Do and De are the diameters of the entrance and exit pupils of the telescope (approximately equal to the diameters of the objective lens and the eyepiece).
There are also some telescopes that do not use a lens (or lens system) as objective, as these are difficult to produce if large apertures and minimum aberrations are required. These telescopes use a concave mirror (usually parabolic) as the objective. They are called reflecting telescopes. Light from a distant object is collected by the large concave mirror and reflected onto a small mirror (positive in the Cassegrain telescope and negative in the gregorian telescope). This mirror is located on the optical axis and light is then transmitted through a central hole in the concave mirror onto the eyepiece. In the newtonian telescope the light collected by the large concave mirror is reflected onto a small plane mirror at a 45° angle to the optical axis, and transmitted to the eyepiece, which is at right angles to the optical axis (Fig. T1).
See binoculars; eyepiece; magnification, telescopic; objective.
astronomical t. See telescope.
bioptic t . A system of lenses forming a galilean or Kepler telescope which is mounted high on a plastic spectacle or carrier lens with the distance correction, so as to allow the patient to look through either the telescope, or below, by moving his or her head. It is used to magnify distant objects for patients with low vision. Syn. bioptic position telescope.
Cassegrain t . See telescope.
Dutch t. See telescope, galilean.
galilean t. A simple optical system that allows observation of far objects with a low magnification and without image inversion. It consists of a convex lens, which acts as the objective, and a concave lens as the eyepiece. Magnification of such a telescope rarely exceeds x 5. This optical system is used in opera glasses and as a low vision aid (Fig. T1). Syn. Dutch telescope.
See binoculars; minification.
gregorian t.; Kepler t.; newtonian t.
See telescope.
reflecting t. A telescope that uses a concave mirror as the objective.
refracting t . A telescope that uses a positive lens system as the objective.
reverse t . See field, visual expander.
terrestrial t. A telescope that provides an erect image of a distant object. The image is usually erected by means of a lens system placed between the objective and the eyepiece. It does, however, make the terrestrial telescope relatively longer than an astronomical telescope.
See binoculars; erector.
telescopic spectacles See lens, telescopic.
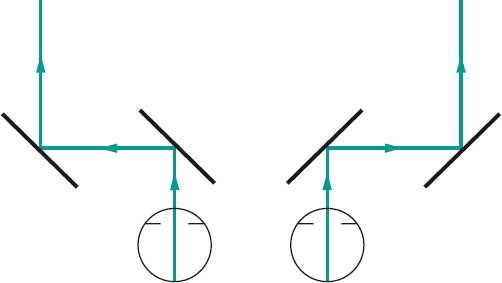
telestereoscope, Helmholtz Instrument designed to produce an exaggerated perception of depth by optically increasing the length of the base line of the viewer, using a system of mirrors or prisms (Fig. T2).
Teller acuity cards See acuity cards, Teller.
temple 1 . See side of a spectacle frame. 2. The lateral area of the human head between the outer canthi and the ears and above the zygomatic arch.
temple, library A straight side of a spectacle frame.
See spectacles, library.
temporal arteritis; induction; summation
See under the nouns.
tendon See muscles, extraocular.
tendon of Zinn See annulus of Zinn.
Tenon’s capsule The fibrous membrane that envelops the globe from the margin of the cornea to the optic nerve. Its inner surface is in close contact with the episclera to which it is connected by fine trabeculae. These trabeculae also attach it to the extraocular muscles. The posterior surface of the capsule is in contact with the orbital fat. Anteriorly, it becomes thinner and merges gradually into the subconjunctival connective tissue. Syn. Bonnet’s capsule; capsule of the eyeball; fascia bulbi.
See injection, sub-Tenon’s; ligament of Lockwood.
tension, ocular See pressure, intraocular.
Terrien’s disease See ectasia, corneal.
Terson’s syndrome See syndrome, Terson’s.
tertiary action; position See under the nouns.
test 1 . A method of examination to determine a disease or a performance. 2. To try; to prove. 3. The equipment used to carry out the test.
after-image t . A subjective test used to determine the presence or absence of abnormal retinal correspondence (ARC). The subject is instructed to fixate the centre of a vertical light filament for some 15 s with one eye and then the centre of a horizontal light filament for some 15 s with the other eye. Looking at the after-images of the two filaments on a uniform surface (e.g. a wall) the subject sees either a cross, which indicates normal retinal correspondence or two separated filaments, indicating ARC. Syn. Hering’s after-image test.
See after-image; retinal correspondence, abnormal.
after-image transfer t. Test aimed at detecting and measuring the angle of eccentric fixation in an amblyopic eye in a patient with normal retinal correspondence. The normal eye fixates an illuminated vertical line and is then occluded, while the amblyopic eye fixates a dot. If the after-image and the fixation point coincide the amblyopic eye has no eccentric fixation, otherwise the relative position of one to the other indicates the angle of eccentric fixation. Syn. Brock’s after-image test.
See fixation, eccentric; retinal corresponding points.
alternate cover t. See test, cover.
Ammann’s t. See test, neutral density filter.
Arden grating t. A clinical test for contrast sensitivity. It consists of photographic plates, each with a sinusoidal grating of constant spatial frequency but of increasing contrast from top to bottom. There are seven plates, one being for demonstration. The other six, each with a different spatial frequency, are used for testing. The spatial frequencies are: 0.2, 0.4, 0.8, 1.6, 3.2 and 6.4 cycles per degree when viewed at a distance of 50 cm. Contrast levels are numbered from 1 to 20 on a vertical scale on the side of the plate. The testing procedure consists of slowly removing each plate from its folder until the grating becomes visible to the patient, at which point the contrast level is noted. The testing is carried out monocularly with optical correction, if any. The procedure is repeated for each plate and all the contrast levels are added to arrive at a score, which is compared with normal values provided in the instructions. Syn. Arden gratings; Arden plates.
See chart, contrast sensitivity; function, contrast sensitivity; Vistech.
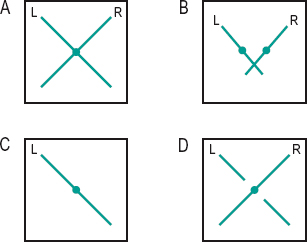
Bagolini’s lens t. A test to detect binocular sensory and motor anomalies such as abnormal retinal correspondence and suppression. Two Bagolini lenses, one in front of each eye with their striations oriented 90° apart (typically 135° for one eye, 45° for the other) are used. The patient fixates a punctate light source at distance and near. Each eye sees a diagonal line perpendicular to that seen by the fellow eye. For example, if one line, or part of one line, is missing there is suppression. If the two diagonal lines cross at the source the patient is orthophoric or if strabismic, as indicated by the cover test, the patient has harmonious abnormal retinal correspondence (Fig. T3). Syn. Bagolini’s striated lens test.
See glass, Bagolini’s.
balancing t. A test designed to obtain equal focusing or equal accommodative states in the two eyes. This is accomplished either objectively (by retinoscopy) or, more commonly, subjectively using either the duochrome test, or comparing the visual acuity in the two eyes simultaneously or successively, or using prisms to present two images of a chart and ask the patient to compare these images, or using a binocular refraction technique (e.g. Turville infinity balance test). Syn. equalization test.
See balance, binocular; method, Humphriss; vectogram.
bar reading t. A test for determining the presence of binocular vision and also used in the management of amblyopia in which a narrow bar (or a pencil) is held vertically between the reader’s eyes and a page of print. The bar occludes a vertical strip of print but the strip is different for the two eyes and if binocular vision is present the subject will experience no difficulty reading the text. Syn. Welland’s test.
basic secretion t. Measurement of the basal tear secretion independently of reflex tear secretion. A filter paper strip (e.g. Whatman No. 41) is placed in the anaesthetized lower fornix, and after five minutes the strip is removed and the amount of wetting measured from the folded end.
See tear secretion; test, Schirmer’s.
Bielschowsky’s head tilt t . A test to determine which of the inferior or superior extraocular muscles and of which eye is paretic. The test is based on the following fact: if the head is tilted to the right, the right intorters of the right eye (superior oblique and superior rectus muscles) contract as well as the extorters of the left eye (inferior oblique and inferior rectus muscles). If the head is tilted to the left, the inferior oblique and inferior rectus muscles of the right eye contract to cause extorsion while the superior oblique and superior rectus of the eye contract to cause intorsion. Thus, tilting the head towards one side will indicate the palsied muscle. For example, in the right superior rectus muscle palsy, when the head is tilted to the left there will be no change in the vertical deviation, since contraction of the right superior rectus muscle is not involved. However, when the head is tilted to the right there will be an increase in downward movement. This test is not reliable in an adult with congenital ocular palsy.
See test, forced duction; test, three-step.
Bielchowsky’s phenomenon t. A test used to differentiate between dissociated vertical deviation (DVD) and alternating hypertropia. After the occlusion of one eye (which elevates behind the cover) a wedge of increasing density is placed in front of the fixating eye; if the patient has DVD the eye behind the cover will perform a gradual downward movement with increasing filter density and a gradual upward movement if the wedge is moved in the opposite direction. Syn dark wedge test.
See deviation, dissociated vertical; phenomenon, Bielchowsky’s.
blind t. See study, single-blind; study, double-blind.
blue field entoptoscope t. See entoptoscope, blue field.
blur back t. See test, plus 1.00 D blur.
break-up time t. (BUT) A test for assessing the precorneal tear film. Fluorescein is applied to the bulbar conjunctiva and the patient is asked to blink once or twice and then to refrain from blinking. The tear film is scanned through the slit-lamp using a cobalt blue filter with a wide beam, while the examiner counts or records the time between the last blink and the appearance of the first dry black spot which indicates that the tear film is breaking up. In normal subjects, break-up times vary between 15 and 35 s (in Caucasians). A BUT of 10 s or less is abnormal and may be due to mucin deficiency, and is often considered to be a negative factor for success in contact lens wear, especially soft lenses. However, this test has been shown to be flawed, because fluorescein can disrupt the tear film.
See film, precorneal; lens, cobalt; mucin; test, non-invasive break-up time.
broad H t. A test to evaluate the integrity of the extraocular muscles and their innervation. The patient is asked to fixate a penlight while keeping the head still. The penlight is moved slowly horizontally to one side of the straight ahead position, then moved vertically, back down to the horizontal line, then below it and back up again to the horizontal line. The penlight is now moved along the horizontal line to the other side of the straight-ahead position and the same procedure is repeated thus completing the shape of the letter with a wide horizontal dimension. Overaction or underaction of one eye and the patient’s report of diplopia in any position of gaze are recorded to identify the paretic muscle/s.
Brock’s after-image t. See test, after-image transfer.
Brock’s string t. See Brock’s string.
Bruckner’s t. See method, Bruckner’s.
Cardiff acuity t. A test for measuring the visual acuity of young children. It is composed of a series of cards, each with a different picture (either a car, a dog, a duck, a fish, a house or a train) drawn with a white band, which is surrounded by a black line half the width of the white, on a neutral grey background. Thus the average luminance of the target is equal to that of the grey background. The picture is situated either in the top or bottom half of the card. The pictures remain of the same overall size on each card; only the width of the black and white bands decreases in size. There are 11 acuity levels ranging from 6/60 (20/200) to 6/6 (20/20) at a viewing distance of 1 metre, in 0.1 log steps. The acuity is given by the narrowest white band for which the picture is still recognizable, but the child’s eye movements are also noted to confirm or establish recognition. This test is best used with toddlers and children with intellectual impairment (Fig. T4).

See method, preferential looking.
City University colour vision t. A set of 10 pseudoisochromatic plates, each consisting of a central coloured spot surrounded by four differently coloured spots. The subject is asked to choose the spot that most closely matches the colour of the central spot in each plate viewed at a normal reading distance. For each plate there is a normal response and a response corresponding to each of the colour defects, deutan, protan and tritan.
See test, Farnsworth.
colour vision t . See Edridge–Green lantern; plates, pseudoisochromatic; test, City University colour vision; test, Farnsworth; test, lantern; test, wool.
confrontation t. A rough method of determining the approximate extent of the visual field. The patient, with one eye occluded, faces the examiner at a distance of about 60 cm and fixates the opposite eye of the examiner. The test object is moved in a plane midway between the examiner and the patient, starting far in the periphery and moving it towards the patient and in various meridians until it is seen.
contrast sensitivity t. See chart, contrast sensitivity; function, contrast sensitivity; sensitivity, contrast; test, Arden grating; Vistech.
corneal reflex t. See method, Hirschberg’s; method, Javal’s; method, Krimsky’s.
cortical vision screening t. (CORVIST) A test designed to detect visuoperceptual impairments caused by a cerebral disease (e.g. Alzheimer, stroke) or injury, in individuals who have normal or near-normal vision (with or without correction). It consists of an A4-size bound book containing a sequence of ten cards, each one assessing a different aspect of visual processing by cortical centres, and prefaced by a description of its aim, instructions and significance. The test includes symbol acuity, shape discrimination, size discrimination, shape detection, hue discrimination, scattered dot counting, fragmented numbers, word reading, crowding and face perception.
cotton thread t . See test, phenol red cotton thread.
cover t . (CT) A test for determining the presence and the type of heterophoria or strabismus. The subject fixates a small letter or any fine detail at a given distance. Strabismus is usually tested first. The opaque cover or occluder is placed over one eye and then removed, while the examiner observes the other eye and then the same operation is repeated on the other eye (this is called the unilateral cover test). If neither uncovered eye moves, the subject does not have strabismus. If the unoccluded eye moves when a cover is placed in front of the other, strabismus is present. In esotropia the unoccluded eye will move temporally to take up fixation, while in exotropia the unoccluded eye will move nasally, and an upward or downward movement indicates hypotropia or hypertropia, respectively. In alternating squint, in which either eye can take up fixation, the eye behind the cover will appear deviated when uncovered and will move as the cover is shifted to the other eye.
The type of heterophoria can be detected by observing the eye behind the cover. If there is no movement of the eye behind the cover, the subject is orthophoric. If the eye behind the cover moves inward, and outward when the cover is removed, the subject has esophoria. If the eye behind the cover moves outward, and inward when the cover is removed, the subject has exophoria. A similar procedure is used for hyperphoria and hypophoria. As it is difficult to view the eye behind the cover without allowing sufficient peripheral fusion to stop the eyes going to the phoria position, the observer usually watches for the recovery movement as the occluder is removed. By placing prisms of increasing power in front of one of the eyes until no movement is evoked, one can evaluate the approximate amount of the phoria. The cover test is the only objective method of measuring heterophoria. The determination of the magnitude of the deviation of the strabismus or heterophoria can also be done with the alternate (alternating) cover test (ACT). The subject fixates a target and the cover is successively placed in front of one eye and then the other while watching the eye that has just been uncovered to see the direction of the deviation. The amount of deviation can be estimated by using prisms of appropriate strength and base direction until the movement of the eye is neutralized when the cover is alternated from one eye to the other (prism cover test).
Although these tests are objective, they are sometimes used subjectively, i.e. the patient indicates the apparent movement of the fixation object. The alternate cover test is the most appropriate test for subjective testing. An apparent movement of the fixation object in the same direction as the cover indicates exophoria, while an apparent movement of the fixation object in the opposite direction to the cover indicates esophoria. An apparent downward movement of the fixation indicates hyperphoria of the eye from which the occluder is moved. Again prisms can be placed in front of the eyes until the apparent movement disappears, thus giving a measure of the heterophoria. This subjective perception of a movement of a stationary fixation object in people with heterophoria or strabismus is a particular example of the phi phenomenon. Syn. occlusion test; screen test.
cross-cylinder t. for astigmatism A subjective test for measuring the axis and the amount of astigmatism using a cross-cylinder lens. Having obtained the best visual acuity with a spherical lens, the cross-cylinder lens is placed before the eye being tested with its axes at 45° to the cylinder axis determined by retinoscopy. The patient looks at a single circular target, often a letter (O or C or Verhoeff’s circles), the cross-cylinder lens is then flipped and if one position provides a clearer image of the target, the axis of the correcting (minus) cylinder should be turned towards the minus axis of the cross-cylinder lens until vision is equally blurred in both positions of the cross-cylinder lens. That point indicates the correct axis of the correcting cylinder. The determination of the power of the correcting cylinder is carried out by placing the cross-cylinder lens with one of its axes parallel to the axis of the correcting cylinder. The cross-cylinder lens is flipped and the position that provides the clearer vision indicates whether to increase the cylinder power (when the minus axis of the cross-cylinder is parallel) or decrease cylinder power (when the plus axis is parallel). The proper amount of cylinder correction is obtained when the vision is equally blurred in both positions of the cross-cylinder lens. Syn. cross-cylinder method; cross-cylinder test; Jackson crossed cylinder test.
cross-cylinder t. at near A subjective test to determine the addition for near vision. It is performed (monocularly or binocularly) at a distance of usually 40 cm with the patient wearing his or her subjectively determined lenses and cross-cylinder lenses with axes horizontal and vertical and viewing a test chart composed of parallel, horizontal and vertical black lines. Beginning with sufficient fogging lens power, the plus lens power is reduced until the patient reports that the vertical and horizontal lines are equally distinct.
See addition; method, fogging.
dark filter t. See test, neutral density filter.
dark room t. See test, provocative.
dark wedge t. See test, Bielchowsky’s phenomenon.
Denver Developmental Screening t. See test, developmental and perceptual screening.
development and perceptual screening t. A test used to assess children’s perceptual and processing skills, such as gross motor coordination, directionality, laterality, visual form perception, visual memory and visualization, visual-motor integration and auditory and language development. There are many such tests, each evaluating one or several of the above skills. The most common ones are: (1) The Denver Developmental Screening Test (DDST), which is used for children up to about six years of age. It is easy to administer and covers a wide range of skills, which fall into four sectors: personal-social, fine motor-adaptive, language and gross motor. Treatment and/or referral will depend on the type of skills found to be abnormal. (2) The Test of Visual Analysis Skills (TVAS) assesses the child’s visual perceptual skills. It consists of 18 squares containing dots and lines, each forming a different pattern. The child is given a pencil and a special test form on which to reproduce the visual stimuli. The test comes with an expected score for each grade up to grade 3 and failure to reach that score may indicate that the child has a perceptual skills disorder. (3) The Gardner Reversal-Frequency Test in which the child is asked to mark those letters and numbers which are printed backward. This test assesses the directionality skill.
developmental eye movement t. (DEM) An indirect test for saccadic eye movements in which the subject reads numbers placed in four vertical columns (total of 80 numbers) and 16 horizontal rows (total of 80 numbers). The lengths of time taken to perform the horizontal and the vertical subtests are measured independently and assessed as a ratio, as well as the number of errors (omissions, additions, transpositions, or substitutions). All results are compared to test norms for the age of the subject. The vertical array mainly gives an indication of visual-verbal number skills (automaticity), whereas the horizontal array provides additional information on oculomotor function.
differential intraocular pressure t. A test for differentiating between a muscle paresis and a mechanical restriction of the eye. The intraocular pressure is measured in the primary position and then again with the patient turning his or her eyes in the direction of action of the suspected paretic muscle. An increase in intraocular pressure of 6 mmHg or more indicates a mechanical restriction (e.g. a fracture of the orbital floor), whereas no change in pressure suggests a muscle paresis. This test produces less discomfort to the patient than the forced duction test.
See test, forced duction.
diplopia t. 1. A test for measuring heterophoria in which the fusion reflex is prevented by displacing the retinal image of one eye with a prism as in the von Graefe’s test in which the magnitude of the phoria is estimated by the amount of prism necessary to align the two images. To measure lateral phorias the images are displaced vertically and aligned one above the other, whereas to measure vertical phorias the images are displaced horizontally and realigned horizontally (if a phoria is present). Syn. displacement test; prism dissociation test. 2. A test to investigate the integrity of the extraocular muscles in strabismus, in which the patient is required to view a light source in the dark with a red filter in front of one eye and a green filter in front of the other, to produce diplopia (prisms are sometimes necessary). The direction and extent of diplopia are evaluated relative to the size and direction of the angle measured with the cover test at the same distance.
See dissociation; test, red-glass.
displacement t. See test, diplopia.
dissociating t. Any test for measuring heterophoria in which fusion is dissociated.
See dissociation; Maddox rod; test, diplopia.
distortion t. A test for measuring heterophoria, in which the images presented to the two eyes are so unlike that they cannot be fused. The most common such test is the Maddox rod test.
doll’s head t. See phenomenon, doll’s head.
Dolman’s t. See test, hole in the card.
double-blind t . See study, double-blind.
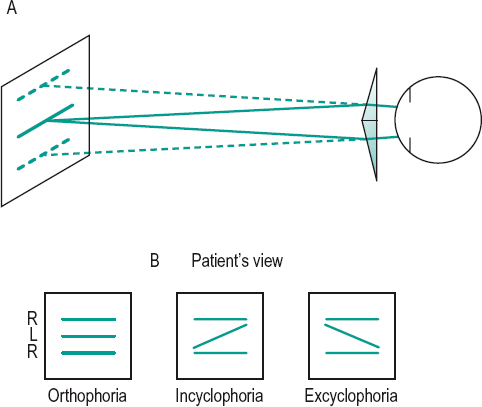
double prism t . A test for determining the presence of cyclophoria, in which a double prism (a pair of prisms set base to base) with the base line horizontal is placed before one eye. The patient is requested to fixate a horizontal line (or row of letters), which through the double prism appears as two lines (or two rows) vertically separated. On uncovering the other eye, the patient sees three lines (or rows). If there is no cyclophoria, all three lines (or rows) will appear parallel, but lack of parallelism indicates cyclophoria. The double prism used in this test consists of two weak prisms (about 4 or 5 Δ): this clinical type of double prism is commonly called a Maddox double prism (Fig. T5).
See bi-prism, Fresnel’s; test, Maddox rod.
Dunlop t. A test for determining motor ocular dominance. It consists in having the eyes fusing two slightly different targets in, for example, a synoptophore, and diverging the targets until diplopia appears. Just beforehand, fixation disparity occurs in one eye. That eye is called the non-dominant or non-reference eye. The other eye is the dominant or reference eye.
duochrome t. A subjective refraction test in which the subject compares the sharpness of black targets (e.g. Landolt rings) of similar sizes, on a red background on one side and on a green background on the other side (blue is sometimes used) of a chart. In undercorrected myopia or overcorrected hyperopia, the letters on the red background will appear more distinct, while in overcorrected myopia or undercorrected hyperopia the letters on the green background will appear more distinct, and in emmetropia or corrected ametropia the letters should appear equally distinct on both sides. The test makes use of the chromatic aberration of the eye and assumes that when the eye is looking at distant objects it is focused on the yellow part of the visible spectrum. Syn. bichrome test; duochrome method.
See lens, cobalt; Verhoeff’s circles.
dye dilution t. A test for detecting a blockage in the lacrimal (or drainage) system. It consists of instilling a few drops of fluorescein (or a mixture of rose bengal and fluorescein) into the conjunctival sac and observing how long it takes before it dilutes which is shown by the change in colour. No change in colour indicates a blockage or a lack of tear production.
See lacrimal apparatus; staining, fluorescein; test, Jones 1.
‘E’t. See ‘E’ game; chart, illiterate E.
equalization t. See test, balancing.
Esterman t. A method of quantifying visual field disability. It consists of a grid made up of rectangles of different sizes placed across the field, being smaller centrally, inferiorly and along the horizontal meridian than at other locations, as these areas are considered to be most important functionally. Each rectangle contains a dot in the centre. There is a grid for the monocular field with 100 rectangles and a grid for the binocular field with 120 rectangles. The grid is placed on top of the results of the field chart. A percentage score is calculated on the basis of the number of spots seen by the patient. The grids are incorporated into most automated perimeters.
fan and block t.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


