Systemic Diseases that Affect the Nose and Sinuses
Systemic Diseases that Affect the Nose and Sinuses
David A. Zopf
Mark A. Zacharek
The role of the otolaryngologist in the diagnosis and treatment of the following systemic diseases discussed in this chapter is multifaceted. Certain disorders may manifest their initial presentation in the nasal/paranasal sinuses. In this instance, an opportunity is presented for an initial workup and diagnosis while obtaining appropriate consultation of additional medical specialists when necessary.
Many of the following diseases present a challenge to the head and neck surgeon. They are oftentimes chronic in nature, with suspicion of an underlying, more widespread issue arising after failure of response to several interventions. A thorough history and physical examination, followed by the appropriate laboratory assays, diagnostic imaging, and tissue biopsies are essential to guiding patients to treatment and relief.
Surgical interventions and procedures may be offered for symptomatic relief in certain pathologies, though treatment for systemic disease is more often medical. For example, a septal button may alleviate symptoms in a patient with septal perforation secondary to granulomatosis with polyangiitis (a newer nomenclature for Wegener granulomatosis [WG]), but the otolaryngologist’s interventions provided in the clinic or operating room cannot replace steroid immunotherapy.
Furthermore, it is often possible to view several of the discussed systemic diseases as pathology on a continuum rather than distinct afflictions. As such, addressing individual conditions while keeping in mind their general pathophysiologic category will assist in understanding successful treatment and diagnosis.
Systemic diseases affecting the nasal and paranasal sinuses are presented in the following sections by pathophysiologic process: genetic/congenital, granulomatous, autoimmune, and hematologic (Table 31.1). However, these groupings are not mutually exclusive, and disease processes discussed may actually fit in more than one of these categories.
CONGENITAL/GENETIC
Cystic Fibrosis
Cystic fibrosis (CF), the most common autosomal recessive disorder in whites (1 case:2,500 live births) is a systemic disease affecting mucous viscosity secondary to a genetic mutation. Mutation in the CF transmembrane conductance regulator gene of chromosome 7 alters a transmembrane channel protein affecting chloride ion movement. An inflammatory reaction ensues leading to cellular breakdown and an accumulation of intracellular/intranuclear products, such as DNA (1). This affects the viscoelastic properties in the pancreas, reproductive organs, and respiratory tract, including the sinonasal cavities (2). In addition, increased bacterial colonization occurs, particularly with Pseudomonas aeruginosa and Staphylococcus aureus (3). Sinonasal disease is a proposed contributor of lung disease, a leading cause of death in CF (2).
Dysfunctional mucus clearance may lead to obstruction of the sinus ostia and mucosal edema leading to nasal obstruction, chronic sinusitis, and sinonasal polyposis. Nearly 100% of CF patients exhibit some aspect of sinus disease (4). The most common CT-imaging findings in CF include sinus opacification followed by the presence of pseudomucoceles. In one series of Brazilian patients, these findings were absent in only two of fifty patients. Hypoplasia or agenesis of the frontal sinuses has also been noted (3). Approximately 36% of carriers of recessive CF mutations reported chronic rhinosinusitis symptoms, versus 14% in the general population (5). In another series of homozygous recessive CF, 117/126 patients exhibited rhinosinusitis. Nasal polyps were discovered in 20% of this series (6).
Diagnosis is made with a positive sweat chloride test and/or genetic test with at least one of the following: (a) typical chronic obstructive pulmonary disease, (b) documented exocrine pancreatic insufficiency, or (c) positive family history.
TABLE 31.1 SUMMARY OF SYSTEMIC DISEASES AFFECTING THE NOSE AND SINUSES
[laser]coagulation, systemic therapies, hormonal therapy, septodermoplasty, Young procedure
Thrombocytopenia
History, CBC, bleeding/clotting parameters
Transfusion, addressing underlying pathology
Treatment should be symptom directed based on severity. Mild symptoms may be managed with nasal irrigations (1). More severe symptoms can be addressed with mucolytics, nasal corticosteroids, and antibiotics (7). Surgical intervention in CF should be utilized with the intent to reduce sinonasal symptoms and improve quality of life, though not with curative expectations. Revision surgery is required in approximately one-third (2) to one-half (8) of CF cases and may be predicted by polyp severity (2). In a randomized double-blind prospective trial, dornase alpha (recombinant human deoxyribonuclease) has been shown to be effective in extending benefits of surgery when used as an adjuvant therapeutic (1).
Lymphoma
Lymphoma may present with nasal involvement that is clinically restricted to the sinonasal airway. The cell lineage of the lymphoma origin is variable. One report investigated the cellular origins of nasal lymphomas in a western patient population and found that 55% of tumors were comprised of natural killer (NK)/T cells, 29% B cells, and 16% T cells. However, these estimates differ in Chinese and Japanese populations where tumors derived from the NK/T-cell lineage are more common (9). An association with Epstein-Barr virus has been proposed for NK/T-cell lymphoma.
Midline destructive lesions have historically been described by several different variations in nomenclature, such as idiopathic midline granuloma, lethal midline granuloma, polymorphic reticulosis, and Stewart syndrome. Improvements in cellular and molecular diagnostics, including immunohistochemistry and flow cytometry, have revealed that many of these lesions are actually WG or lymphomatous (10). Furthermore, extensive investigation into subdivision of classifications of NK/T-cell lymphoma is an active area of current research. Subdivision into upper aerodigestive tract NK/T-cell lymphoma (nasal cavity, nasopharynx, oral cavity, oropharynx, hypopharynx disease) and nonupper aerodigestive tract NK/T-cell lymphoma has been proposed (11).
Clinical presentation of lymphoma involving the sinonasal compartments includes epistaxis, nasal obstruction, nasal swelling, and constitutional or B-type symptoms (malaise, weight loss, fever). More advanced disease may reveal a friable necrotic mass, potentially obstructing the nasal cavity/nasopharynx. Local extension, when present, has been reported to involve the maxillary sinus (42%), ethmoid sinuses (36%), nasopharynx (25%), and rarely skull base or cranial nerves (9).
Diagnosis may be particularly challenging in instances of mild or early stage disease. An initial routine workup with baseline serologic assays and clinical/endoscopic examination are followed by biopsy of suspicious nasal mucosal disease. Sufficient fresh samples should be obtained for immunophenotyping by flow cytometry. Histologic analysis may reveal lymphocytic infiltrates with angiocentric necrosis.
TABLE 31.2 ANN ARBOR CLASSIFICATION FOR LYMPHOMA
Ann Arbor
Classification for Lymphoma
Stage I
Involvement of a single lymph node region or single extralymphatic site
Stage II
Involvement of two or more lymph node regions on the same side of diaphragm, localized contiguous involvement of only one extralymphatic site and lymph node region
Stage III
Lymph node involvement on both sides of the diaphragm
Stage IV
Disseminated involvement of one or more extralymphatic organs with or without lymph node involvement
Table 31.2 details the Ann Arbor Lymphoma staging system. Alternate staging based on various classifications, such as anatomic subsites, or treatment responses have been proposed (11).
Treatment and follow-up should be directed by hematology/oncology specialists. No advantage for the addition of chemotherapy to radiation has been shown in early stage (I/II) NK/T- cell lymphoma (overall 5-year survival (OS) rates of 38%-RT versus 35%-CRT (12); 66%-RT versus 76%-CRT (13); 59.2%-RT versus 52.3%-CRT (14)). Lack of success with chemotherapy alone may be a result of P-glycoprotein expression that confers increased multidrug resistance in CD56+ NK cells (15). Studies of combination therapy reveal sequence impacts outcomes. In chemotherapy followed by 45 Gy of radiation, the complete response (CR) rate was 49.1%, compared to 100% in those who received radiation followed by chemotherapy (16). A review by Kohrt and Advani cite several studies lending support for combined chemoradiation in high-risk or advancedstage disease (stage III/IV), where 5 year OS drops to 20%. Several aspects of the therapeutic strategy in nasal NK/T-cell lymphoma are topics of current investigations.
GRANULOMATOUS
Sarcoidosis
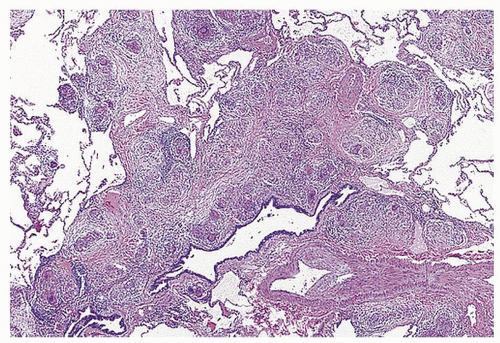
Sarcoidosis is a noncaseating granulomatous disease, oftentimes involving multiple systems (Fig. 31.1). A demographic predisposition for African American and Scandinavian individuals of age range in the twenties and thirties has been demonstrated (17).
Development is likely multifactorial, leading to an abnormal immune response, of which T cells and their proinflammatory cascades are thought to be at the center. Mycobacterial tuberculosis catalase-peroxidase protein was reported to be present in approximately 50% of sarcoidosis tissue samples (18). Activated tissue macrophages are the primary source for angiotensin-converting enzyme elevations (19). Genetics appear to contribute to predisposition of development of sarcoidosis. In one study involving 210 pairs of monozygotic and dizygotic twins and at least one proband, concordance rates of sarcoidosis were found to be significantly higher in monozygotic than in dizygotic twins. Compared with the general population, there was an 80-fold increased risk of developing sarcoidosis in cotwins of effected monozygotic brothers or sisters (20). Responsible genes, such as butyrophilin-like 2 gene, have been proposed (19). It is hypothesized that an environmental factor prompts an aberrant immunologic response, though no strong associations in the literature have led to a specific environmental offender.
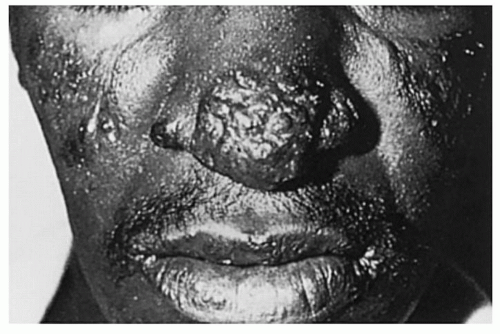
The wide range of symptomatology makes recognition of sarcoidosis a challenge. Incidental discovery on chest x-ray (CXR) in asymptomatic patients accounts for a large proportion of presentations. In the symptomatic patient, one or more of the following systems may be involved: respiratory (cough, dyspnea, chest pain), integumentary (lupus pernio, erythema nodosum, papules, nodules, plaques), ocular (orbital pain, uveitis, visual changes), rheumatologic (arthralgia, myalgia), and constitutional (fevers, night sweats, fatigue) (21). Lupus pernio, the most characteristic skin lesion for sarcoidosis, occurs at a higher preponderance in sarcoidosis with sinonasal features (Fig. 31.2).
As pulmonary findings are a hallmark of sarcoidosis, a close collaboration with a pulmonologist is recommended. Chest radiographic findings are classified as follows: stage 0, normal CXR; stage 1, isolated intrathoracic adenopathy; stage 2, intrathoracic adenopathy and parenchymal disease; stage 3, parenchymal disease; and stage 4, pulmonary fibrosis (22).
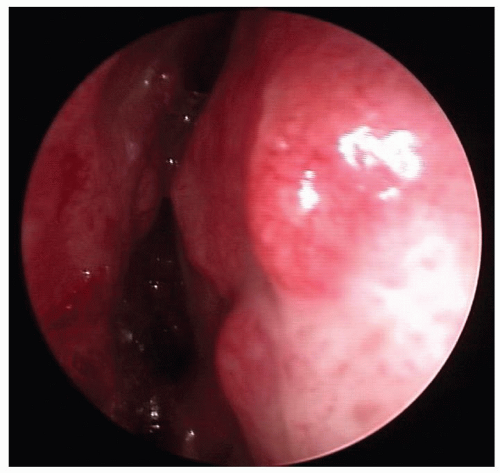
Sinonasal manifestations occur in approximately 1% to 5% of cases, of which only 10% are present in absence of pulmonary disease (23,24,25), and include nasal congestion, nasal obstruction, rhinorrhea, nasal crusting, epistaxis, nasal mass, facial/nasal pain, and anosmia (23,26). On physical examination, purplish, friable nasal mucosa, mucosal hypertrophy, nasal polyps, and yellow submucosal nodules may be observed, most commonly involving the septum and inferior turbinates (Fig. 31.3). Thickening of sinus mucoperiosteum and radiologic paranasal opacification mark sinus involvement (24,27). Of 15 patients undergoing CT with sarcoidosis and sinus symptoms, the maxillary (14), ethmoid (9), frontal (6), and sphenoid (3) sinuses demonstrated complete or partial opacification (23).
Figure 31.1 Sarcoidosis. Multiple noncaseating granulomas are present along the bronchovascular interstitium. Image from Rubin E, Farber JL. Pathology, 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 1999.
Figure 31.2 Raised lesions of lupus pernio. (From Crapo JD, Glassroth J, Karlinsky JB, et al. Baum’s textbook of pulmonary diseases, 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2004.)
When presented with sinonasal findings in suspected sarcoidosis, histological biopsy revealing noncaseating granulomas is the definitive mode of diagnosis. With the differential diagnosis including fungal and mycobacterial infections, the respective histopathology and tissue cultures are required to rule these out. However, patients who present with Lofgren syndrome (erythema nodosum, hilar adenopathy, and polyarthralgias) can be clinically diagnosed without the necessity of biopsy (19). ACE levels and serum calcium levels may be elevated. Though nonspecific, C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) levels are often elevated. Equally important are ruling out other potential disease processes and assessing the extent of pathology, for example, antineutrophil cytoplasm antibodies (ANCA) should be measured to rule out WG.
Figure 31.3 Endoscopic view of nasal sarcoidosis. The septal mucosa, as well as the lateral nasal wall reveals nodular, erythematous swellings.
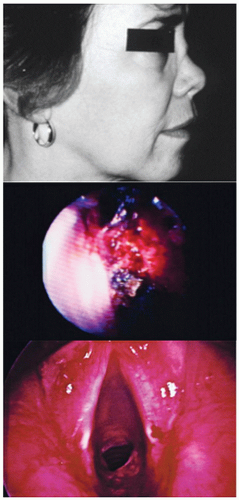
Figure 31.4 Saddle-nose deformity in WG, bloody crusts in WG, subglottic stenosis in WG. (From Koopman WJ, Moreland LW. Arthritis and allied conditions a textbook of rheumatology, 15th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2005).
Treatment should be tailored to the severity and extent of disease involvement. Many patients diagnosed with sarcoidosis do not require treatment. In symptomatic patients, nasal corticosteroids for skin disease and non-steroidal anti-inflammatory drugs (NSAIDs) may be utilized for mild disease, where higher dose systemic corticosteroids and immunomodulators for more extensive disease may be initiated with close medical follow-up. Six to nine months of prednisone, initiated at a dose of 30 to 40 mg daily followed by a 5 mg/day taper to a 10 to 20 mg/day maintenance dose, is recommended (19). Methotrexate has been shown to be an effective therapeutic and allows for decreased doses of systemic steroid administration in a randomized double-blind trial (28). Additionally, hydroxychloroquine, azathioprine, pentoxifylline, statins, and tumor necrosis factor (TNF-α) TNF-alpha binding proteins/inhibitors, such as infliximab, etanercept, and adalimumab, have been described for the same intent (29). A multicenter randomized, double-blind, placebo controlled trial of infliximab has shown improvements in pulmonary function with pulmonary sarcoidosis, though the remaining biologics mentioned have otherwise not shown dramatic efficacy to date (19). Sinonasal involvement has been shown to be a poor prognostic indicator with a high frequency of recalcitrant disease involving multiple vital organs, thus oftentimes necessitating systemic therapy (23).
The goal for surgical intervention in sarcoidosis is not eradication of disease, but potential quality of life improvement. Kay and Har-El examined the role for endoscopic sinus surgery in sarcoidosis. Six of 86 sarcoidosis patients underwent endoscopic sinus surgery with indications including granulomatous or polypoid lesions causing severe nasal obstruction or blocking the osteomeatal complex leading to symptomatic chronic or acute recurrent sinusitis. CO2 laser surgery has also been described for treating such granulomas (29
Only gold members can continue reading. Log In or Register to continue