Management of Temporomandibular Joint Pain and Dysfunction
Joseph J. Fantuzzo
Sveta Karelsky
Temporomandibular disorders (TMDs) are conditions affecting or arising from the temporomandibular joint (TMJ), muscles of mastication, or both. TMD typically manifests as pain in the head and neck region and there is often an effect on neighboring structures. The pain can mimic other painful disorders of the head and neck as well. TMDs may be interpreted as facial pain, headaches, earaches, aural fullness, clicking or popping of the ears, mild hearing loss, tinnitus, dizziness, difficulty with mouth opening, chewing or speech, closed or open lock of the TMJ, wear of the occlusal (biting) surfaces of the teeth, joint noises (clicking or popping), and other complaints. TMDs occur in an estimated 5% to 15% of the general population, peaking in young adults age 20 to 40 years. Signs of TMD occur equally in males and females, but symptoms occur and are reported more frequently in women of childbearing age. Approximately 2% of the general population seeks treatment for TMJ-related symptoms (1,2).
Patients with complaints of TMJ-related pain often have parafunctional oral habits or a history of trauma, as well as concomitant medical or psychological conditions. TMJ disorders TMDs may be divided into nonarticular muscle disorders and articular (intracapsular) disorders. Nonarticular disorders include masticatory muscle (myofascial) pain and dysfunction and can commonly be associated with fibromyalgia or other chronic pain states and irritable bowel syndrome (3). Trauma can affect the TMJ itself and associated structures. Articular disorders include osteoarthrosis, inflammatory joint diseases, infections, and benign and malignant lesions.
The role of the otolaryngologist is both to differentiate temporomandibular from other regional pathology and to initiate a treatment plan for the disease. Because of the variety of symptomatic presentations of TMDs patient perceptions of the origin of symptoms vary widely. Patients may be referred to the otolaryngologist for presumed pathology of the ear, sinuses, or parotid gland. It is not uncommon for patients to have been treated for infectious disorders of these structures prior to referral. An appropriate explanation of the anatomic basis of pain must be provided for the patient if trust is to be gained and recommendations are to be carried out. Symptoms and their severity must be accepted as reported and treated accordingly. Accurate diagnosis is important in the development of an effective treatment plan.
Patients should be reassured that TMD is generally a benign condition and clinical improvement is expected in time and with appropriate therapy. Complete elimination of symptoms is difficult and at times impossible. The goals of therapy include patient education, alleviation of pain, and improvement in jaw function.
Pain and jaw dysfunction are the hallmarks of TMD, and the pathophysiology, differential diagnosis, and management of the problems behind pain and limited jaw function are the primary focus of this chapter.
ANATOMY AND PHYSIOLOGY OF THE TMJ
The TMJ exists between the base of the skull (temporal bone) and the mandible (condylar process). The articulating bony surfaces, the articular disk, several ligaments, and numerous associated muscles make up the joint (Fig. 54.1). The purpose of the temporomandibular (or craniomandibular) articulation is to provide range of motion and to allow for the functional aspects of the mouth and jaws during breathing, speech articulation, mastication, and swallowing.
Of the bones of the head, only the TMJ and the ossicles of the ear have articulations. The secondary TMJ in humans develops by the 10th week of gestation, from mesenchymal condensations of two separate blastemas for the condyle and temporal bone. The TMJ and ear ossicles are derived from membranous bone (4,5). Superior to the condylar blastema, a band of mesenchymal tissue differentiates into
the disc as an extension of the lateral pterygoid muscle (4,5,6). Embryologic studies suggest an intimate relationship between the fetal TMJ and the middle ear through the petrotympanic fissure. This relationship may contribute to referred pain patterns or the spread of infection (7).
the disc as an extension of the lateral pterygoid muscle (4,5,6). Embryologic studies suggest an intimate relationship between the fetal TMJ and the middle ear through the petrotympanic fissure. This relationship may contribute to referred pain patterns or the spread of infection (7).
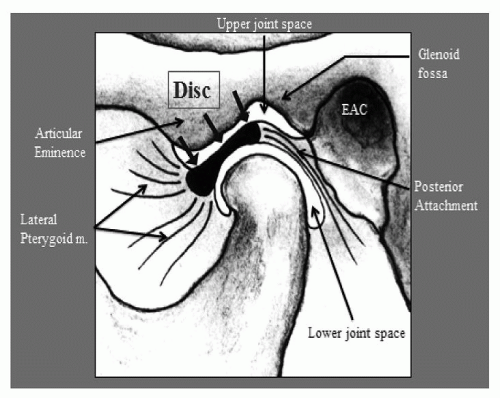 Figure 54.1 TMJ—Normal anatomy. |
The articular disc is a biconcave structure that prevents bone on bone contact of the articulating surfaces and more evenly distributes articular forces. It has an anterior and posterior band and intermediate, thinner avascular zone. The disc is also attached at the medial and lateral condylar poles. The disc divides the articular space of the TMJ into a superior and inferior joint space. Posteriorly, the retrodiscal attachment is bilaminar and has significant neurovascularity. This retrodiscal tissue is intracapsular, and pain within the joint itself may be due to retrodiscal injury or inflammation. Theories of intracapsular pain are discussed later in the chapter (4,5).
The development of the primary and adult dentition influences the shape of the fossa, eminence, and condylar head. The glenoid fossa represents a concavity within the temporal bone that fits the mandibular condyle. The anterior wall of the fossa is the articular eminence. The posterior wall, made up of the tympanic plate of the temporal bone, is also the anterior wall of the external acoustic meatus. An early periosteal lining becomes the dense, avascular, fibrous connective tissue cover for the articular surfaces. The articulating surfaces are different from hyaline cartilage surfaces of other synovial joints. Edentulism leads to secondary change within the fossa and eminence (8).
The TMJ is thinly encapsulated anteriorly, medially, and posteriorly, with a thick capsule laterally forming the temporomandibular ligament. The ligament has a narrow deep portion and wider fan-shaped lateral portion. The fibrous capsule and ligament provide support and limit jaw range of motion.
The sensory innervation of the TMJ is from the auriculotemporal, deep temporal, and masseteric nerves. The blood supply to the capsule and disc is from the branches of the maxillary artery.
The motor activity of the joint results from motor innervation of the masticatory musculature, through the third division of the trigeminal nerve. The various muscle groups of the face, tongue, palate, and hyoid are also involved in functions that include the TMJ: The masticatory muscles (masseter, temporalis, medial pterygoid, and lateral pterygoid) and other important muscles (digastrics and supra-and infrahyoid muscle groups) play a significant role in the functioning of the TMJ. The actions of the muscles together on the hyoid, mandible, and related structures are important during jaw function. This interrelationship is important to consider when arriving at a differential diagnosis. A thorough review of anatomy including the actions of this musculature is beyond the scope of this chapter.
Movements of the mandible include opening and closing, protrusion, retrusion, and lateral excursions. The motion of the mandible at the TMJ is hinge-like occurring primarily within the lower compartment and gliding or translatory within the upper compartment. Unlike other joints, the left and the right side disc, condyle, and associated musculature function simultaneously. Maximum mandibular opening (between incisors) is 40 to 55 mm, is generally less in women, and decreases with advancing age (4,5,9).
PATHOPHYSIOLOGY
TMDs typically present with pain with mandibular function, limitation of mandibular movement, and joint sounds. Muscle-related pain is more common than internal joint-related pain, but they often occur together. Muscle pain may adversely affect internal joint function and vice versa, over time. Differentiating muscle pain from internal derangement is important to successful treatment. Myalgias generally present regionally with muscle weakness or fatigue and limited passive range of motion. Palpation reveals muscle tenderness. Typical problems include myalgia and myositis due to parafunction, trauma, or infection. The involved musculature may be tender, swollen, and warm. Chronic masticatory muscle contraction may be seen, with myofibrosis limiting range of motion. Previous trauma, surgery, and planned restricted range of motion (maxillomandibular fixation) will result in limited range of motion that may or may not return to normal over time.
The literature suggests that patients with myofascial TMD pain may be hypersensitive to pain, or have altered pain perception pathways. Some have features of brain morphology consistent with other chronic pain states, such as fibromyalgia. In such patients, studies of CNS regions involved in pain processing indicate changes to areas processing pain signals from the trigeminal system (10,11).
An intracapsular disorder implies a disc-condylar fossa abnormality and is associated with joint noise, and abnormal, often limited condylar movement. Intracapsular disorders are referred to as internal derangements and represent anterior disc displacement with or without reduction. The anterior displacement is thought to represent adaptive change
within the joint to functional demand. Disc displacement with reduction is associated with joint noise, and may or may not progress to disc displacement without reduction. Anterior displacement without reduction is present when the disc remains displaced throughout mandibular motion. The disc may interfere with condylar movement. Typically there is an absence of joint noise. A nonreducing disc is thought to represent a more chronic problem (12) (Fig. 54.2).
within the joint to functional demand. Disc displacement with reduction is associated with joint noise, and may or may not progress to disc displacement without reduction. Anterior displacement without reduction is present when the disc remains displaced throughout mandibular motion. The disc may interfere with condylar movement. Typically there is an absence of joint noise. A nonreducing disc is thought to represent a more chronic problem (12) (Fig. 54.2).
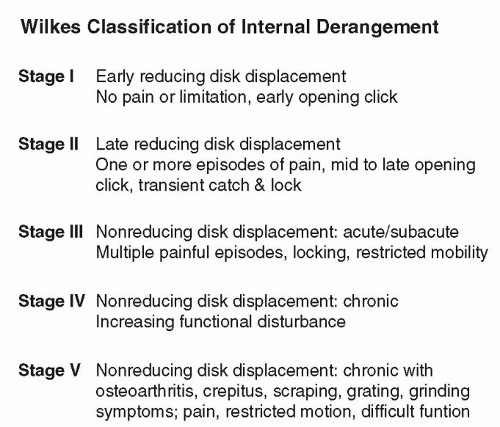 Figure 54.2 Wilkes classification of internal derangement. |
Mouth opening is typically limited to less than 25 mm with a nonreducing disc displacement (closed lock). The mandible will deviate to the affected side upon opening, as the unaffected side translates normally. Lateral excursion (toward the unaffected side) is limited on the affected side as well. Degenerative changes of the bone may or may not be present with disc displacement. Intracapsular adhesions may be present. These fibrous adhesions are thought to occur with stretching and bleeding within the superior joint space.
Psychosocial Comorbidity
TMD patients often present with a level of pain, stress, and depression beyond that expected by the clinician. It is not clear whether these occur as a result of chronic pain, or whether they contribute to the parafunctional habits that can generate TMJ-related disorders. A large Finnish study found that patient-reported TMD symptoms are significantly associated with stress, depression, overload at work, life satisfaction, and work satisfaction. Pain perception and predisposition to TMD may be significantly affected by psychosocial stressors (13). When evaluating patients with TMD stress must be addressed by the treating clinician.
Molecular Biologic Mechanism of Injury
Both mechanical functional limitation and inflammation contribute to pain. Inflammation may lead to intracapsular swelling and pain. There can be inflammation of the joint capsule (capsulitis) and of the synovial lining (synovitis) resulting in pain and limitation in movement.
Trauma to the vascular and richly innervated retrodiscal tissues can also cause effusion, pain, and limited range of motion. The inflammation within the joint can cause secondary muscle splinting leading to more limitation in range of motion and more discomfort.
Milan described a theory of direct mechanical stress leading to the creation of free radicals contributing to a degenerative process within the joint. Direct mechanical injury from excessive load leads to increased levels of IL-8 and production of nitric oxide synthetase with NO release and free radical formation causing direct tissue damage and induction of arachidonic acid, inflammation, and tissue breakdown within the joint (14).
Other causes of free radical formation include the theories of hypoxia-reperfusion and that of neurogenic inflammation. The theory of hypoxia-reperfusion proposes that clenching increases pressure within the joint, which overwhelms capillary perfusion pressure, leading to hypoxia. Reperfusion leads to free radical formation. Neurogenic inflammation occurs with the release of neuropeptides (substance P, calcitonin) released from activated nerve terminals within the capsular ligament and retrodiscal tissue contributing to the inflammatory response.
Another hypothesis for closed lock of the TMJ is that of adhesion of the disc to the articular eminence secondary to insufficient lubrication of the joint from overloading. Nitzan described impairment of joint lubrication due to free radical formation. Inflammation secondary to macro- or microtrauma causes free radical formation and increased oxidative stress within the joint leading to the loss of lubricating hyaluronic acid (HA) and chondroitin sulfate within synovial fluid. Increased hyaluronidase leads to breakdown of HA, the major lubricant within the joint. Loss of lubrication causes capsular fibrosis and immobility of the TMJ disc. Arthrocentesis has been proposed by Nitzan and colleagues to allow for immediate release of the disc. Decreased lubrication increases viscosity and contributes to disc dislocation as the disc adheres to the glenoid fossa during motion. Adhesions vascularize and add to restriction. Increasing laxity of the lateral disc attachment occurs and the disk is gradually displaced (15,16).
Synovial fluid analysis attempts to identify the underlying pathogenesis of TMDs. The synovial membrane provides nutrients to cartilage. Diminished synovial fluid quality and quantity is thought to compromise nutrition of the articular surfaces and diminish protection and lubrication of the joints (15).
Inflammatory mediators within the injured joint worsen and prolong pain and dysfunction. Cytokines, proteases, and other substances have been implicated in internal derangement and degenerative joint disease (17). Osteoarthritis may be an imbalance between protease and protease inhibitor. Specific cytokines and growth factors have been implicated. Cytokines (IL-1, IL-6, IL-8, interferon, and TNF) may
induce proteases. Growth factors induce tissue inhibitor of metalloproteinase. Matrix metalloproteinase has been identified as a mediator of cartilage degradation (18). PGE2 synthesized by synovial cells, mediated by IL-1, plays a role in bone resorption. LTB4, synthesized by synovial cells, is elevated in painful joints and is chemoattractant for inflammatory cells. Synovial fluid analysis demonstrates increased IL-B and IL-6 in osteoarthritis (19,20,21,22,23,24).
induce proteases. Growth factors induce tissue inhibitor of metalloproteinase. Matrix metalloproteinase has been identified as a mediator of cartilage degradation (18). PGE2 synthesized by synovial cells, mediated by IL-1, plays a role in bone resorption. LTB4, synthesized by synovial cells, is elevated in painful joints and is chemoattractant for inflammatory cells. Synovial fluid analysis demonstrates increased IL-B and IL-6 in osteoarthritis (19,20,21,22,23,24).
Surgical procedures have been developed, based on the above theories. The goal of arthrocentesis or arthroscopy as the initial surgical intervention for internal derangement and osteoarthritis is to reduce the presence of inflammatory mediators as well as to lyse adhesions.
Hypomobility Disorders
Causes of TMJ hypomobility may be trismus or anatomical obstruction such as bony or fibrous ankylosis. Pain and limited range of motion may also be secondary to internal derangement of the joint. Imaging is helpful in arriving at a diagnosis. A screening panoramic radiograph may be helpful to rule out fracture, unusual anatomy (coronoid hyperplasia), or pathology. Computerized tomography (CT) imaging may be necessary to identify a fracture, degenerative disease, ankylosis, or neoplasia. Magnetic resonance imaging (MRI) is helpful when evaluating the location of the articular disc, presence of joint effusion (inflammation), and in revealing the presence of fibrous ankylosis. Hypomobility due to trismus is most frequently caused by infection, inflammation, neoplasm, radiation, or trauma. If painless, trismus may be associated with the presence of a tumor. Rarely temporal arteritis can cause trismus (25,26,27).
Ankylosis can be due to fibrous scar formation, bone formation, or a combination of both. Trauma is the most frequent cause in developed nations. Children who are unable to translate with opening the jaw are at increased risk of developing ankylosis. TMJ infections are rare but are reported as the cause of TMJ ankylosis in 10% to 49% of cases (28). Inflammatory arthritis such as rheumatoid and psoriatic arthritis contributes to another 10%. Juvenile idiopathic arthritis can affect the TMJ often with absence of symptoms in 50% of children (29,30,31). Clinical examination findings of limited opening or deviation with opening without pain should prompt the clinician to evaluate further with MRI. Intra-articular steroid injections may be beneficial (32).
The ankylotic joint requires surgical management to release fibrous tissue or resect heterotopic bone. Reankylosis is a common complication. Gap arthroplasty has a low (50%) success rate and TMJ reconstruction is often indicated with autogenous or alloplastic materials (28).
Hypermobility Disorders
Hypermobility leading to subluxation or dislocation of the TMJ can occur with yawning, prolonged opening, during a seizure, or due to trauma. A subluxed condyle becomes temporarily trapped anterior to the articular eminence. Typically, the patient will spontaneously self-reduce the mandible. Treatment is often necessary with dislocation. Dislocation implies the need for manually assisted mandibular reduction. Immediate manual reduction is essential as manipulation becomes more difficult with time. If the patient experiences repetitive dislocations with pain interfering with daily function, surgical intervention is considered. Surgical options include plication with wires, osteotomy of the zygomatic arch (Le Clerc procedure) to create an obstruction and eminectomy to remove obstruction and allow spontaneous reduction of the subluxed mandible. With eminectomy, subluxation will continue to occur, but without risk of dislocation. Lateral pterygoid myotomy is described by some authors as beneficial therapy (33,34,35,36).
Posttraumatic TMDs
Maxillofacial trauma may be the initiating event in certain cases of TMD. Many types of traumatic events are associated with temporomandibular dysfunction, including accidental, assault-related, or surgical trauma. Fractures of the mandible and surrounding structures often require treatment by the otolaryngologist, and awareness of their effect on the temporomandibular articulation is helpful.
Mandibular fractures often cause pain, malocclusion, restricted opening, loss of mandibular height, muscle spasm, or deviation of the mandible to one side. If not properly addressed, any of these features may cause disabling TMD. Normal TMJ function requires a complex mechanism of intact bone and balanced muscular forces, and traumatic disruption of any of these elements can lead to joint pathology. Anatomic reduction and rigid fixation, when indicated, are important for a good functional outcome.
Fracture of the mandibular condyle, in particular, tends to predispose to pathology of the TMJ. Condylar fractures comprise around 30% of mandible fractures, and may involve the condylar neck or, more rarely, be intracapsular. The position of the articular disc relative to the fracture site is thought to have prognostic significance. Disk displacement from the fracture appears to strongly predispose to posttraumatic joint ankylosis, as the insulating role of the disk between the articulating surfaces is lost. Joint ankylosis, or fusion, is perhaps the most severe form of TMD and produces complete joint immobility on the affected side. This is not frequently encountered in the industrialized world, but in developing countries it is quite a common consequence of mandibular trauma. Up to 98% of ankylosis cases have been estimated to originate from trauma to the mandibular condyle (37). This may be particularly common in sagittal fractures, especially when a bone fragment with a raw edge is displaced laterally or there is another, associated mandible fracture (38,39,40) (Fig. 54.3).
The treatment of mandible fractures involving the condylar process has long been controversial. Generally, anatomic reduction and fixation of condylar fractures in
adults is recommended when there is loss of mandibular height or gross comminution or dislocation of fractured segments. Anatomic fracture reduction along with postoperative rehabilitation seems to generate good results (41



adults is recommended when there is loss of mandibular height or gross comminution or dislocation of fractured segments. Anatomic fracture reduction along with postoperative rehabilitation seems to generate good results (41
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
