16 Surgical Technique for Migrated Disk with Foraminoplasty • Since the introduction of the concept of percutaneous posterolateral nucleotomy by Kambin in 1973, percutaneous endoscopic lumbar diskectomy (PELD) has evolved over the years.1–7 • PELD is increasingly becoming a preferred choice of treatment for the management of lumbar disk herniation. • The transforaminal approach offers several advantages: — Protection of the posterior ligamentous and bony structures causing a lower incidence of postoperative instability,8–10 facet joint arthropathy, and disk space narrowing.2–5,11–21 — No interference of the epidural venous system that may lead to chronic neural edema and fibrosis.2,14–16,22 — Epidural scarring, a common sequel after open diskectomy, which leads to clinical symptoms in more than 10% of patients, is rare in PELD.23–25 • The narrow transforaminal window provides limited access that proves adequate for the removal of nonmi-grated or low-migrated disk herniations. • Limited access may render the PELD procedure ineffective in cases of high-grade migrations.6,7,25 • Migrated intracanal disk herniations, especially high-grade migrations, pose a greater challenge even for an experienced endoscopic surgeon. • The success of the PELD procedure depends considerably on appropriate placement of the working instruments in optimal trajectory to directly visualize and access the migrated ruptured fragment.19,26,27 • Improper trajectory to the pathology is an important cause for the failure of the procedure. • The biggest difficulty encountered during retrieval of high-migrated disk herniations is obtaining this optimal trajectory,26 which is significantly hindered by the natural obstacles of the normal anatomy and worsened by the degenerative changes. • Enlargement of the “foraminal gate” by widening one of the walls via foraminoplasty can help us to address this issue. • We define foraminoplasty as “widening of the foraminal gate by undercutting a ventral (nonarticular) part of the superior facet and sometimes the upper part of the inferior pedicle along with ablation of the foraminal ligament to visualize the anterior epidural space and its contents.” • This is achieved with the help of bone trephines or reamers, an endoscopic drill, endoscopic chisels, and a side-firing holmium:yttrium-aluminum-garnet (Ho:YAG) laser. • There is a need for foraminoplasty, especially to access highly migrated intracanalicular disk herniations, because of the following: — Lumbar disk herniations are common at the lower levels where the diameter of the intervertebral foramen is small as compared with the higher levels.28 — Degenerative changes leading to hypertrophy and overriding of facets and thickening of the foraminal ligament may cause additional narrowing of the transforaminal window. — High-migrated disk herniations lie in the region of the spinal canal that is hidden from the endoscopic view by natural anatomical barriers.— These barriers prevent direct access to the migrated fragment (Table 16.1). — Min et al29 have demonstrated that the dimensions of the working zone in the sagittal plane, specifically the base dimension, are of clinical importance in the current practice of endoscopic surgery. — Foraminoplasty provides adequate working space needed for the excision of the ruptured fragment under direct endoscopic vision through the enlarged foramen.
Introduction
Anatomical Considerations
Downward Migrated | Upward Migrated |
Hypertrophied superior facet of the inferior vertebra | Superior foraminal ligament |
Lateral edge of the ligamentum flavum | Lateral edge of the ligamentum flavum |
In severely migrated cases—upper part of the inferior pedicle |
|
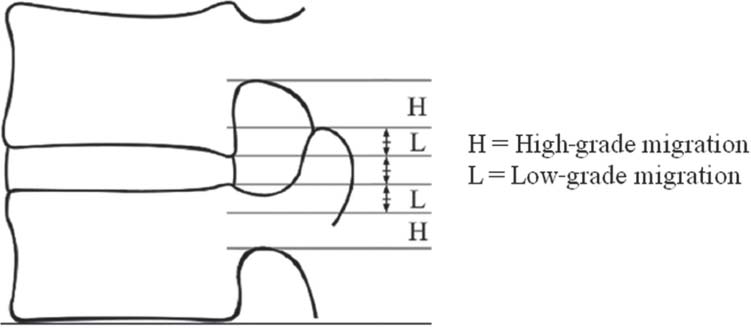
Fig. 16.1 The degree of migration of the herniated fragment in relation to the posterior height of the disk space.
Migrated Disk Herniations
• Regardless of whether extruded or not, herniations displaced either above or below the end plate level are called migrated disk herniations.
• Migrated disk herniations are classified into two grades depending on their extent of migration.
• If the extent of migration is greater than the measured height of the posterior marginal disk space on T2-weighted sagittal magnetic resonance imaging (MRI), it is called a high-grade migration.26,27,31
• Migration smaller than the height of the disk space is classified as a low-grade migration (Fig. 16.1).32
Types of Foraminoplasty
Foraminoplasty is classified into two types depending on the extent of bony resection.
Conventional Foraminoplasty
• Conventional foraminoplasty essentially involves undercutting of the nonarticular part of the superior facet and removal of the lateral edge of the ligamentum flavum in cases of downward-migrated disk herniations.
• The release of the superior foraminal ligament and the ligamentum flavum in cases of upward-migrated disk herniations
• The need for undercutting of the facet may diminish at high lumbar levels above L3-L4.
• Because the upper part of the foramen is wider than the lower part and there is no superior facet to obstruct visualization of the anterior epidural space, bone cutting is not needed in cases of upward-migrated disks (Fig. 16.2).
Extended Foraminoplasty (Foraminoplasty with Oblique Pediculotomy)
• In severely downward-migrated disk herniations where the ruptured fragment lies in close contact with the medial wall of the pedicle, the upper part of the inferior pedicle may prevent its direct visualization.
• Removal of the upper and medial wall of the pedicle along with the undercutting of the superior facet can help visualize and access the ruptured fragment (Fig. 16.3).
• The downward inclination of the endoscopic trajectory enables oblique cutting of the upper part of the pedicle and is thus called oblique pediculotomy.
Surgical Technique
Position and Anesthesia
• PELD is performed under local anesthesia with the patient in the prone position on a radiolucent table under the guidance of C-arm fluoroscopy.
• Conscious sedation with midazolam and fentanyl allows continuous feedback from the patient during the entire procedure to avoid causing damage to the neural structures.
• Midazolam is administered in the dose of 0.05 mg/kg intramuscularly a half hour before surgery followed by another dose intravenously during surgery if required.
• Fentanyl dosage is 0.8 μg/kg intravenously 10 minutes before surgery followed by additional doses intraoperatively if required.
Preoperative Planning
• Axial MRI or computed tomographic (CT) scans are used to calculate the distance of the needle’s skin entry point from midline.
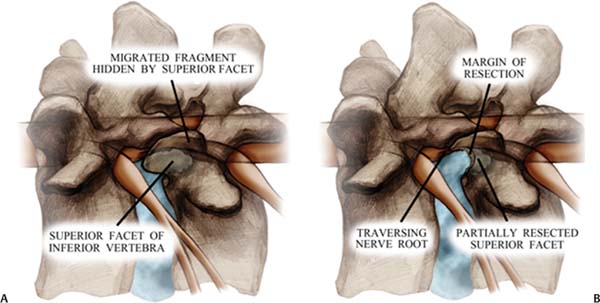
Fig. 16.2 The anatomical change of the neural foramen before (A) and after (B) foraminoplasty.
• These scans are also used to calculate the needle trajectory, targeting the ruptured fragment while avoiding the contents of the peritoneal sac (Fig. 16.4).
Needle Insertion Technique
• It is imperative to achieve proper placement of the needle, which is facilitated by complying with the following guidelines:
— The site of annular puncture by the needle tip should be at a medial pedicular line in the anteroposterior view and a posterior vertebral line in the lateral view of fluoroscopic imaging (Fig. 16.5). This corresponds to the Kambin safe triangle in the axillary area between exiting and traversing nerve roots.
— The midpedicular line should be considered for upper lumbar disk herniations (L3, L4, and above) to avoid neural injury because the dural sac is bigger with more nerve tissue, lying more laterally due to the narrow width of the pedicles at the upper levels.33–36
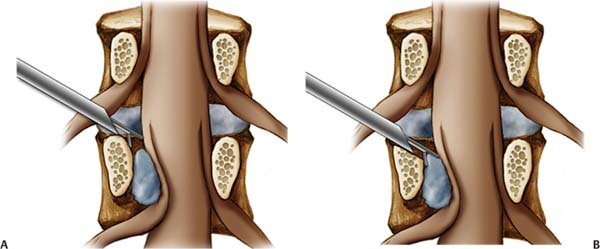
Fig. 16.3 Oblique pediculotomy. Removal of the upper and medial walls of the pedicle (A), along with the undercutting of the superior facet (B), can help visualize and access the ruptured fragment.
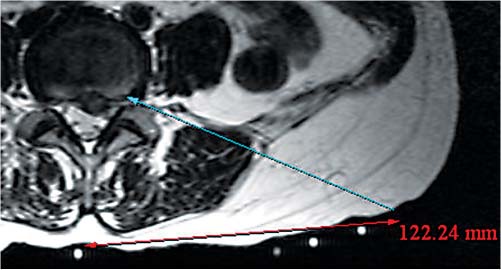
Fig. 16.4 Preoperative planning. Axial MR or CT images are used to calculate the distance of the skin entry point of the needle from the midline, and the needle trajectory is aimed to target the ruptured fragment while avoiding the contents of the peritoneal sac.
Inclination of the Needle Trajectory
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


