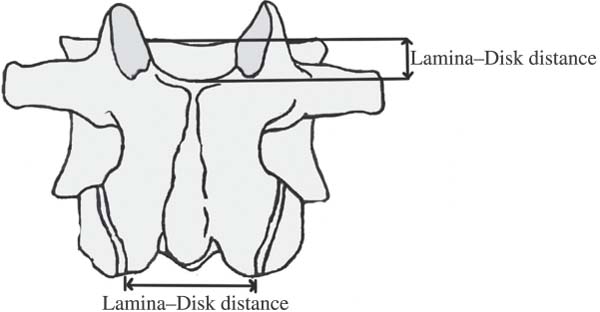
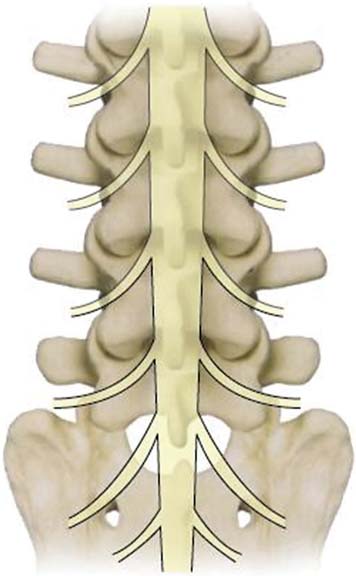
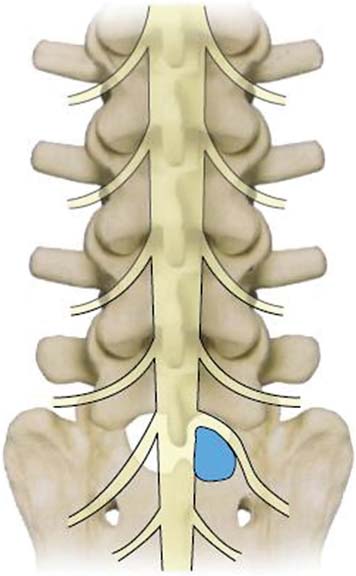
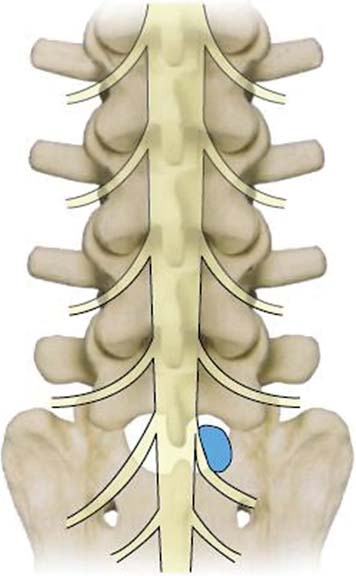
17 Interlaminar Surgical Approach Thorough knowledge of anatomy is an essential requirement in every surgical specialty. • Endoscopic spine surgery is a target-oriented surgery that relies on a precise mental projection of a pathological lesion and its relations to surrounding bony landmarks. • Unlike with microsurgery, in endoscopic surgery the surgeon does not have the liberty of visually identifying the bony landmarks and then going through them to find the neurological structures. • The surgeon must know the intimate relation of various neurological structures with the surrounding bone and rely heavily on the fluoroscopic guidance to insert the initial needle at the exact target point as has been identified on the preoperative plan while avoiding all the important anatomical structures lying in between. • Another important aspect of endoscopic spine surgery is knowing the endoscopic images of various anatomical structures. This chapter describes the important anatomical features needed to carry out a percutaneous interlaminar endoscopic diskectomy at the L5-S1 level in three sections: • Discuss the unique anatomical features of the L5-S1 segment that makes it amenable to this approach. • Describe the methods used to project various important anatomical structures [as defined on computed tomographic (CT) and magnetic resonance imaging (MRI) scans] onto the radiographs and make the pre-operative plan. • Describe the endoscopic pictures of various anatomical structures seen during the course of this procedure so the reader can have a fair idea of what to expect before embarking upon this exciting journey. It is not applied only for the L5-S1 level; we can apply this technique into other levels. The L5-S1 level has unique anatomical features that come into play for interlaminar endoscopic diskectomy technique: • Most of the lumbar disks have a laminar overhang, meaning that the lamina of the upper vertebra extends inferiorly in a manner that the concerned disk space lies at a level relatively superior to the lower margin of the lamina. However, this laminar overhang over the disk space decreases as we move from the upper lumbar to the lower lumbar levels. At the L5-S1 level, the cephalocaudal distance between the lower margin of the L5 lamina and the upper margin of the L5-S1 disk space varies from 3.0 to 8.5 mm. This is the smallest of the lumbar levels. • The small laminar overhang at the L5-S1 level creates a relatively larger interlaminar space. • The inferior margins of the upper lamina lie at a level relatively posterior to that of the superior margins of the lower lamina in the whole of the lumbar spine. This difference is seen more clearly at the L5-S1 level than at the other levels. • In combination with a wider interlaminar space and a negligible laminar overhang, this arrangement creates a trapezoidal space configuration that allows more working space for the outer cannula and its manipulation during the procedure, especially if the initial needle trajectory is kept at a 5- to 10-degree caudocranial angle. • The maximum interlaminar width as defined by the distance measured between the most inferomedial aspects of the inferior facets is also greater at the L5-S1 space as compared with the upper levels (Fig. 17.1). • The interlaminar width average at L5-S1 is 31 mm (range 21 to 40 mm), as compared with an average width of 23.5 mm seen at the L4-L5 level, due to the relatively wider laminae of L5.1 • The wider interlaminar width provides an easy passage of the working cannula (Fig. 17.1). • The S1 nerve root has a relatively cephalad exit from the thecal sac compared with the upper lumbar levels. The S1 nerve root exits from the thecal sac at the level of the L5-S1 disk space or above it. In their cadaver analysis of the origin of lumbar spinal roots in relation to the intervertebral disk, Suh et al reported that the S1 nerve root originates above the level of the L5-S1 disk in 75% of the subjects and at the level of the disk in 25%, but never below the level of the disk.2–5 • The S1 nerve root average take-off angle from the thecal sac is 17.9 ± 5.8 degrees.2 Although this angle is relatively less than the upper lumbar levels, an L5-S1 disk herniation is more likely to be axillary because of the cephalad exit of the S1 nerve root in front of the L5-S1 disk space (Fig. 17.2).4,5 • This axillary disk herniation can also displace the S1 nerve root far into the subarticular region, creating a potential space between the thecal sac and the nerve root. This artificial space created by the pathological lesion can be gainfully exploited for carrying out a safe inter-laminar approach endoscopic diskectomy (Fig. 17.3). • Shoulder disk herniation at the L5-S1 level is relatively uncommon; in this case, the herniated disk pushes the S1 nerve root medially, toward the thecal sac, and the needle can be targeted directly over the hernia mass lying over the superomedial aspect of the pedicle (Fig. 17.4). Fig. 17.1 Illustration of the maximum interlaminar width at the L5-S1 level. Fig. 17.2 Illustration of the S1 nerve root, which takes off at a relatively smaller angle from the thecal sac. Fig. 17.3 Illustration of an axillary disk herniation, which can displace the S1 nerve root far into the subarticular region, creating a potential space between the thecal sac and the nerve root. Fig. 17.4 Illustration of a shoulder disk herniation at the L5-S1 level, which pushes the S1 nerve root medially, toward the thecal sac. • The ligamentum flavum is a 2- to 6-mm-thick, yellow structure that spans the interlaminar space. It is an active ligament that has an essential biomechanical role. It also acts as a protective barrier for the thecal sac, and any injury to it is probably not without consequences.6 • Peridural fibrosis is the direct consequence of intrusion into the spinal canal with a break of the ligamentum flavum7 because the peridural fibrosis occurs due to migration of fibroblasts that are derived from the differentiation of overlying detached muscle that have gained access to the spinal canal.6–8 • Although the ligamentum flavum is thinnest at the L5-S1 level, it is the only major protective barrier to the neural structures at this level because of the minimal laminar overhang. Therefore, preservation of integrity and continuity of the ligamentum flavum at the L5-S1 level is the most important.
Anatomical Considerations
Unique Features at the L5-S1 Level
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


