Surgical Management of Posterior Uveal Melanoma
Carol L. Shields
Jerry A. Shields
There have been several new developments in the management of patients with choroidal melanoma over the past decade. Depending on the clinical circumstances, observation, photocoagulation, transpupillary thermotherapy, plaque radiotherapy, charged particle irradiation, local resection, enucleation, orbital exenteration, chemotherapy, and immunotherapy have been employed.1,2,3,4 There has been a trend away from photocoagulation, with increasing interest in transpupillary thermotherapy (TTT) alone for small melanomas or TTT in combination with radiotherapy for small, medium, and some large melanomas. The recently recognized clinical risk factors for growth and metastasis of small melanocytic tumors allows for earlier detection and treatment of small choroidal melanoma. Consequently, there is a trend away from observation and a focus toward earlier treatment of small melanocytic lesions that possess risk factors. This chapter provides an overview of the methods of management for patients with choroidal melanoma.
GENERAL CONSIDERATIONS
Historically, enucleation of the affected eye was considered to be the only appropriate management for the patient with a posterior uveal melanoma. However, several years ago, some authorities challenged the effectiveness of enucleation for preventing metastatic disease and even proposed that enucleation may somehow promote or accelerate metastasis.5,6 The validity of these arguments was challenged by others who believed that early enucleation offered the patient the best chance of cure.7,8 This controversy over enucleation was responsible for initiating a trend away from enucleation and the increased use of more conservative therapeutic methods.
Depending upon several clinical factors, management options today include observation, photocoagulation, TTT, radiotherapy, local resection, enucleation, and various combinations of these methods. The two most frequently employed treatment methods today are enucleation and plaque radiotherapy. The Collaborative Ocular Melanoma Study (COMS) was organized and funded in 1985 to address several issues related to management of choroidal melanoma.9 More recently, there has been a documented trend of detection of smaller choroidal melanomas and increasing use of conservative treatment methods such as plaque radiotherapy.1,10,11,12
PERIODIC OBSERVATION
Approximately 6% of the Caucasian population manifests choroidal nevus.13 Choroidal nevi are managed by periodic observation. It is estimated that 1 in 5,000 choroidal nevi evolve into choroidal melanoma.14 Risk factors predictive of growth of small melanocytic lesions and their combined predictive values are listed in Tables 1 and 2 (Fig. 1). Documented growth of a melanocytic choroidal tumor is suggestive that the lesion is a choroidal melanoma. Because documented growth may be associated with worse systemic prognosis, some patients with small tumors that show three or more risk factors are treated promptly, without waiting for documentation of growth.12,15,16 On the basis of the few patients with medium-size choroidal melanoma who refuse treatment and are followed, natural history studies have found that there is greater mortality and higher risk of death.17
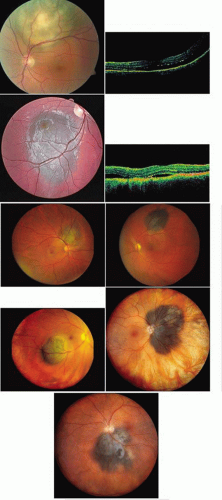 Fig. 1. Clinical risk factors for growth of small choroidal melanoma. (TFSOM = To Find Small Ocular Melanoma represents factors of Thickness over 2 mm, subretinal Fluid, Symptoms, Orange pigment, and Margin of tumor at optic disc) A. Thickness greater than 2 mm. Perimacular small choroidal melanoma measuring 2.9 mm in thickness and with overlying orange pigment and subretinal fluid, manifesting as retinal striae. B. Thickness greater than 2 mm. Optical coherence tomography demonstrating subfoveal fluid in the patient in A. C. Subretinal fluid. Sixteen-year-old patient with documented enlarging small choroidal melanoma and shallow subretinal fluid. D. Subretinal fluid. Optical coherence tomography demonstrating subfoveal fluid in the patient in C. E. Symptoms. Small choroidal melanoma producing symptoms of blurred vision from subfoveal fluid. Note the overlying orange pigment. F. Symptoms. Small choroidal melanoma located superiorly with trough of subretinal fluid in the foveola producing symptoms of metamorphopsia. G. Orange pigment. Macular choroidal melanoma with prominent overlying orange pigment and a rim of subretinal fluid. H. Margin at the optic disc. Minimally elevated small choroidal melanoma touching the optic disc. I. Other features. Juxtapapillary small choroidal melanoma with overlying orange pigment, shallow subretinal fluid, and irregular margins suggestive of tumor activity. |
Table 1. Clinical features predictive of growth of small melanocytic choroidal tumors (≤3 mm thickness)12 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 2. Tumor growth in 1287 small (≤3 mm thickness) melanocytic choroidal tumors based on combination of clinical risk factors11 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
PHOTOCOAGULATION
Photocoagulation is still an acceptable method for treating selected small choroidal melanomas.18,19 It was originally performed with xenon photocoagulation and later with argon laser photocoagulation. Studies showed that xenon achieved better tumor control but argon was associated with fewer complications.19 Low-energy long-exposure laser therapy has been advocated by some authorities.18 Recently, TTT has largely replaced argon laser for treating selected small melanomas, particularly those that are less than 3 mm in thickness and located more than 3 mm from the foveola.
Photodynamic therapy using verteporfin has been considered, but there is little evidence of its effectiveness. One report on four patients showed tumor regression for 18 months in one patient, but lack of response or continued growth in three patients.20
TRANSPUPILLARY THERMOTHERAPY
Transpupillary thermotherapy (TTT) is a recently popularized method of treating selected small- and medium-sized choroidal melanomas.21,22,23,24 With this technique, infrared radiation, using a modified diode laser system, delivers heat to the tumor, causing tumor necrosis. Transpupillary thermotherapy is typically delivered in three sessions and, at completion, leaves an atrophic chorioretinal scar at the site of the previous tumor. Tumor control is found in over 90% of properly selected cases.24 The tumors most suitable for TTT are small, heavily pigmented melanomas less than 3 mm in thickness, with minimal or no subretinal fluid, and are located in the extramacular region, not touching the optic disc (Fig. 2). Tumors at the optic disc show greater recurrence and are best managed with plaque radiotherapy combined with thermotherapy. Choroidal melanoma treated with TTT should be followed long term because delayed recurrence, even with extrascleral extension, can occur.25,26 Currently, TTT is used most frequently as a supplement to plaque radiotherapy.27 A newer technique using a transscleral thermotherapy probe has been found effective for choroidal melanoma and intrascleral tumor.28
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


