 Surgical Management of Conjunctival Tumors
Surgical Management of Conjunctival TumorsSurgical Management of Conjunctival Tumors
It is important that malignant or potentially malignant conjunctival tumors be completely removed with as little manipulation as possible. The most appropriate surgical method differs with limbal tumors, extralimbal tumors, and primary acquired melanosis (PAM) (1,2,3,4). The surgical techniques are reported in detail in the literature (1) and are briefly described herein. Limbal lesions are generally best managed by localized alcohol corneal epitheliectomy, removal of the main mass by a partial lamellar scleroconjunctivectomy, and supplemental double freeze thaw cryotherapy. Tumors located in the extra-limbal conjunctiva are managed by alcohol application, wide circumferential surgical resection, and cryotherapy.
There are no rigid methods for management of PAM of the conjunctiva. In general, it is best managed by alcohol epitheliectomy, removal of suspicious pigmented foci, quadratic staging biopsies, and cryotherapy from the underside of the conjunctiva. In all cases, a “no-touch” method is used and direct manipulation of the tumor is avoided in an effort to prevent tumor cell seeding into a new area (1). During this surgery, it is often prudent to place punctual plugs in the upper and lower canaliculus to prevent seeding of tumor cells in the lacrimal drainage system.
Certain ancillary approaches are frequently employed in conjunction with primary surgical resection of selected conjunctival lesions. These methods include mucous membrane or amniotic membrane grafting, topical chemotherapy or immunotherapy, and radiotherapy. Grafting is used when large portions of conjunctival tumors are excised and tissue is required to close the defect. Topical mitomycin C, 5-fluoroacil, and interferon are used primarily as alternatives to further surgical resection of superficial lesions of the bulbar conjunctiva and cornea, particularly conjunctival/corneal intraepithelial neoplasia and PAM. Radiotherapy is used primarily for cases of squamous cell carcinoma, melanoma, or other conjunctival neoplasms in which further surgical excision is not feasible to achieve good tumor control and in which orbital exenteration is becoming the only therapeutic option.
Regarding topical chemotherapy, we have primarily employed mitomycin C. It is administered by applying one drop of 0.04% mitomycin four times daily for 7 days and then withholding the drug for 1 month. This 2-week cycle is repeated two or three times, depending on the observed response as determined mainly by slit-lamp biomicroscopy. Topical chemotherapy has been highly successful in controlling selected superficial conjunctival malignancies.
Selected References
1. Shields JA, Shields CL, De Potter P. Surgical approach to conjunctival tumors. The 1994 Lynn B. McMahan Lecture. Arch Ophthalmol 1997;115:808-815.
2. Shields JA, Shields CL, De Potter P. Surgical management of circumscribed conjunctival melanomas. Ophthal Plast Reconstr Surg 1998;14:208-215.
3. Shields CL, Shields JA. Overview of tumors of the conjunctiva and cornea. In: Foster CS, Azar DT, Dohlman CL, eds. Smolin and Thoft’s The Cornea. 4th ed. Philadelphia: Lippincott, Williams & Wilkins; 2005:735-755.
4. Shields JA, Shields CL. Tumors of the conjunctiva. In: Stephenson CM, ed. Ophthalmic Plastic, Reconstructive and Orbital Surgery. Stoneham, MA: Butterworth-Heinemann; 1997:260-261.
Surgical Resection of Circumscribed Conjunctival Tumors Near Limbus
Surgical planning and technique are very important in management of conjunctival tumors. Depicted is the drawing that is done in the clinic and placed in the operating room at the time of surgery. The surgical steps are shown in the drawings.
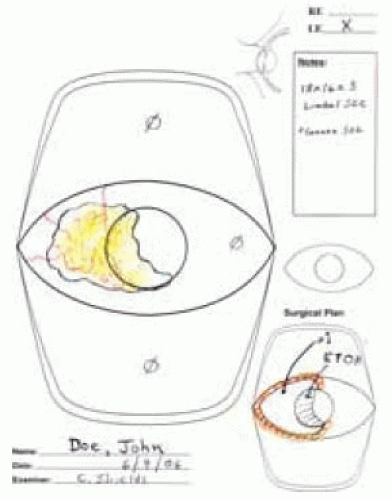 Figure 25.1. Large drawing of circumscribed limbal and corneal tumor. The large drawing is done in the office at slit-lamp examination and is used in all cases at the time of surgery. The drawing shows the extent of corneal involvement, as seen in the office using slit-lamp biomicroscopy. Number 1 is the extent of the lesion to be resected. The orange color is used to indicate the extent of cryotherapy, done immediately after tumor is removed. ETOH indicates the area where absolute alcohol is applied. |
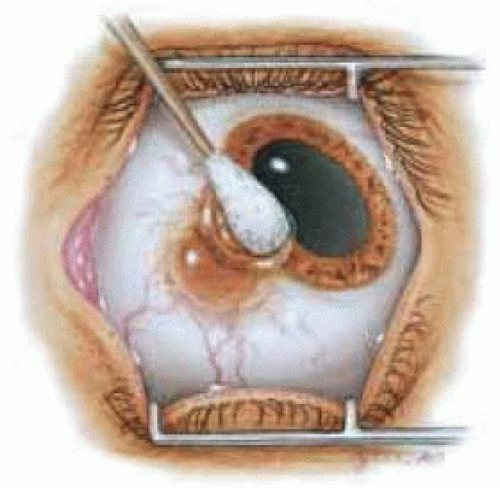 Figure 25.2. Alcohol being applied with a cotton-tipped applicator to a conjunctival melanoma with peripheral corneal invasion. A small cellulose sponge is more often used today. |
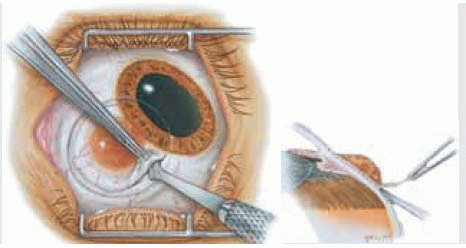
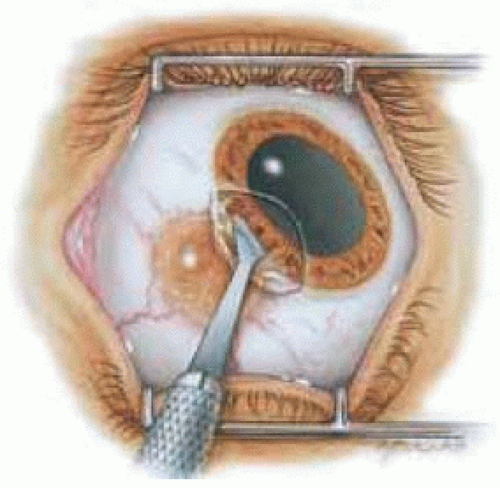 Figure 25.3. Localized corneal epitheliectomy being performed with a small scalpel using a gentle, controlled scrolling technique. The corneal epithelium is gently everted and laid on the surface of the main tumor at and behind the limbus. |
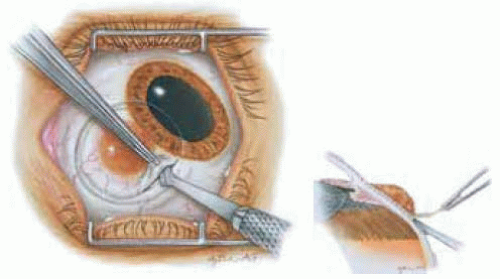 Figure 25.4. A superficial scleral groove has been made around the tumor base, which is being removed by dissecting a thin layer of superficial sclera immediately beneath the tumor and just posterior to the limbus. Inset shows side view of depth of superficial scleral dissection.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|