Surgical Management of Congenital Obstruction of the Lacrimal Collecting System
Richard M. Robb
PROBING AND IRRIGATION
Indications and Timing
The indication for probing and irrigation of the lacrimal collecting system is persistent obstruction with tearing and discharge dating from the early months of the first year. Probing is the initial procedure to consider for such obstruction. Except for the lacrimal puncta, the drainage system cannot be visualized directly, and probing helps to locate the level and nature of the obstruction. Fortunately, in children the probing also is highly effective in relieving the blockage,1,2,3 and in most instances, further procedures are not necessary.
Congenital nasolacrimal duct obstruction has a high rate of spontaneous resolution during the first year,4,5,6,7 There is some difference of opinion about how early to resort to probing to clear persistent obstructions. Early probing may clear the symptoms faster, but a routine of early probing leads to performing many procedures that would be unnecessary. I usually advise delay of probing until near the end of the first year. Mucopurulent discharge from infection in the collecting system usually is present to some degree. It can be managed with lid hygiene and the application of antibiotic ointments. Pressure over the lacrimal sac can be used to prevent accumulation of discharge. This pressure usually results in retrograde flow of the sac contents onto the eye, where they can be wiped away. Occasionally, the pressure is transmitted hydrostatically down the nasolacrimal duct, and with a sudden popping sensation the obstruction may be relieved.8 Failing this, persistent purulent discharge and lid irritation are reasons to proceed with probing. An episode of frank dacryocystitis with swelling and redness in the area of the lacrimal sac is a more pressing indication for probing. The dacryocystitis is first treated with systemic antibiotics, but subsequent probing to relieve the obstruction is necessary to prevent recurrence. A further indication to probe on an accelerated timetable is the need to clear the lacrimal system infection before anticipated ocular, facial, or intracranial surgery. Occasionally, the timing of a probe may be influenced by the need for general anesthesia for some unrelated surgery and the convenience of doing both procedures under one anesthesia.
A special indication for early probing is distention of the lacrimal sac at birth, caused by a combination of nasolacrimal duct obstruction and a physiologic canalicular blockage of retrograde flow, the so-called congenital dacryocystocele. Probing should be undertaken in the newborn period rather than later because secondary infection is likely to develop in the closed system.4,9 Beyond this, dacryocystoceles also may be associated with distention of the nasolacrimal duct and intranasal cysts, which cause respiratory distress in young infants.10,11 The lacrimal puncta and canaliculi are small at this early age, but even without anesthesia, the inferior canaliculus usually can be dilated and probed to decompress the lacrimal sac, and the lower duct obstruction can be broken by passing the probe on into the nose. If a distal intranasal cyst is present, it may require a more extensive procedure under anesthesia, including nasal endoscopy and marsupialization of the cyst.11
The timing of probing and irrigation may be affected by the decision whether or not to perform the procedure under general anesthesia. In the newborn period, the procedure is often done without anesthesia, and many ophthalmologists prefer to perform the probe in the office with topical anesthesia until the infant is 6 months of age.1, Beyond 6 months, I routinely use general anesthesia in an ambulatory operating room setting. Probings done under general anesthesia are more comfortable for the patient, and they are technically easier and better controlled for the surgeon. An endotracheal tube usually is not required for standard probing, although without a tube, irrigation must be limited to prevent aspiration. If access to the nose is required, intubation is necessary. A skilled pediatric anesthesia staff helps to make probing under general anesthesia a safe and reliable procedure.
Contraindications
Whereas there are no absolute contraindications to probing and irrigation for persistent obstruction of the lacrimal drainage system, several considerations may affect the timing of the probe. There is no reason to perform a probe in the early months of the first year if the lacrimal sac is not distended and symptoms are manageable. Spontaneous clearing occurs in most obstructions up to at least 12 months of age.4,5,6,7 If parents are anxious about a surgical procedure, especially one under general anesthesia, additional time can be allowed for clearing. Probing should be delayed if there is an upper respiratory tract infection or if there is acute dacryocystitis. Any contraindications to general anesthesia, such as severe congenital heart disease, may delay treatment. If probing is done in the presence of congenital heart disease, prophylactic antibiotics are advisable because of the possibility of transient bacteremia.
Procedure
When performing a probe without anesthesia, the lower canaliculus usually is easier to enter, but under general anesthesia the upper canaliculus is the preferred access to the system. The upper punctum is dilated, and a Bowman no. 0 (0.7-mm diameter) or no. 1 (0.8-mm diameter) probe (Fig. 1) is passed through the canaliculus into the lacrimal sac (Fig. 2). Occasionally, the obstruction is at the level of the punctum itself, a blockage signaled by symptoms of tearing without discharge, and when the punctum is opened, tear flow is normalized. More often, the obstruction is at the lower end of the lacrimal duct, and the probe can be passed to that point relatively freely. It is helpful to bend the probe to a gentle curve so that after it reaches a firm stop at the medial wall of the sac in the lacrimal fossa, it can be directed down and posteriorly into the duct (Fig. 3). Lubricating the probe with an ophthalmic ointment also eases its passage. At the lower end of the lacrimal duct, slightly firmer pressure is necessary to break through the membranous obstruction into the nose. It may help to direct the curve of the probe posteriorly and medially to break into the nose under the inferior turbinate. Then the probe either stops at the floor of the nose or, due to the curvature of the probe, runs posteriorly along the floor without a hard stop. If uncertainty exists as to whether the probe has entered the nasal cavity, a second Bowman probe can be placed in the nose under the inferior turbinate to feel the contact of metal on metal. The probe then is withdrawn, and saline is irrigated through the system using a glass syringe and a 23-gauge cannula threaded through one canaliculus into the sac (Fig. 4). The other canaliculus is plugged with a lacrimal dilator to prevent reflux. Only a small amount of fluid (approximately 1 mL) is required to establish that the lacrimal duct is open; larger amounts increase the risk of aspiration. Fluorescein can be used to stain the irrigant so that it can be visualized using a clear suction catheter in the nose, but patency of the system usually can be recognized by feeling the free movement of the plunger of the glass syringe.
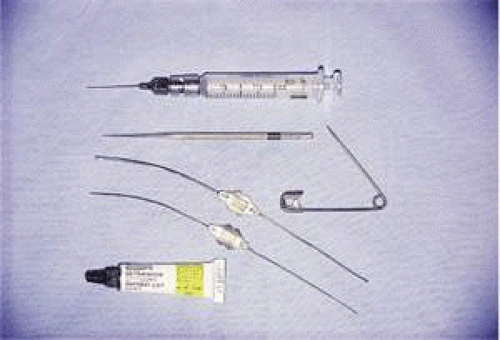 Fig. 1. Instruments required for lacrimal probe: a 23-gauge cannula attached to a glass syringe to irrigate the lacrimal drainage system; a punctum dilator or safety pin to dilate the canaliculus; the Bowman probes, which are bent to a gentle curve; and ophthalmic ointment to lubricate the probes. |
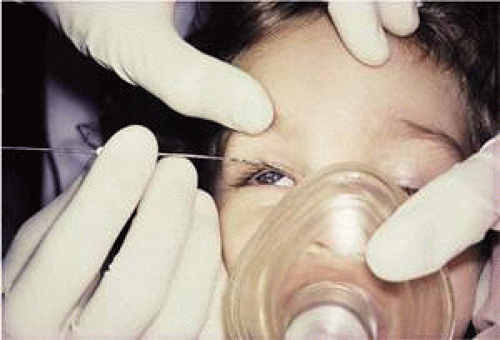 Fig. 2. A Bowman probe is passed through the upper canaliculus into the lacrimal sac in an anesthetized patient. The probe can be presumed to be in the sac when its tip is stopped by the firm medial wall of the lacrimal fossa. |
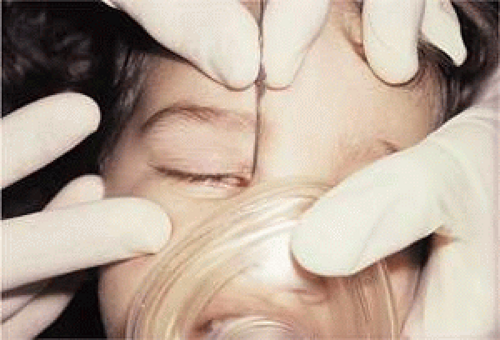 Fig. 3. The Bowman probe has been directed down and posteriorly along the lacrimal duct. Slightly more pressure may be necessary to break through the membranous obstruction at the lower end of the duct. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


