Surgical Management of Anterior Segment Trauma
Peter S. Hersh
Bruce M. Zagelbaum
Kenneth R. Kenyon
Bradford J. Shingleton
The leading causes of ocular morbidity include lacerating and blunt anterior segment trauma. The primary goal in the surgical management of these injuries is directed primarily at the restoration of normal ocular anatomy; the ultimate goal is to prevent secondary complications and maximize the patient’s visual prognosis. Today, a better understanding of ocular injury and the development of modern surgical approaches may permit the primary repair and eventual reconstruction of severely traumatized eyes that would have been lost in the past. The severity of the injury will usually dictate which management approach is instituted.
LACERATING ANTERIOR SEGMENT TRAUMA
PREOPERATIVE MANAGEMENT
To determine the extent of injury, a meticulous preoperative assessment is crucial. A detailed history of the traumatic event should be taken. One must consider the presence of an intraocular foreign body. If a perforating injury is suspected, a rigid protective shield should be used to avoid any inadvertent pressure on the globe that may result in extrusion of intraocular contents.1 Radiologic testing is obtained as necessary, again stressing to all of those involved the importance of avoiding external pressure on the eye during the study. Orders are written to give the patient nothing by mouth in anticipation of surgical intervention. Antiemetics and analgesics are administered to avoid vomiting and agitation. Appropriate informed consent for the surgical procedure(s) anticipated should be obtained before administering any pain medications or sedatives. Immediate family members should be notified when possible.
The proper operating room staff should be assembled and surgery should be performed as soon as possible. Administration of broad-spectrum intravenous antibiotics is begun immediately. A combination of a cephalosporin (e.g., cefazolin) or vancomycin for gram-positive bacteria and an aminoglycoside (e.g., gentamicin) for gram-negative prophylaxis may be appropriate. Vancomycin may be preferable to a cephalosporin because of better coverage of Bacillus species and resistant Staphylococcus epidermidis.2 Clindamycin is added to this regimen if an intraocular foreign body is present, especially if the wound has been contaminated with vegetable matter, because such patients are prone to devastating Bacillus infections.2 Fluoroquinolone agents (e.g., levofloxacin), which have a broad spectrum of activity against gram-positive, gram-negative, and atypical bacteria, may be used as well. Subconjunctival antibiotic injections are avoided preoperatively because they may cause eyelid squeezing and could potentially deliver concentrated drug into the open globe. Similarly, topical antibiotics are avoided unless the wound is self-sealing. Although the risk of tetanus from an anterior segment injury is low, tetanus prophylaxis should be administered in accordance with the recommendations of the Centers for Disease Control and Prevention.3
During repair of corneoscleral lacerations, cultures should be taken from the wound margins, prolapsed and devitalized tissues, and intraocular foreign bodies if there is a high index of suspicion for infection. Specimens are inoculated directly on blood and chocolate agar plates, Sabouraud’s dextrose medium for fungus, and fluid thioglycolate or cooked meat broth for anaerobes.
CONJUNCTIVAL LACERATIONS
With any conjunctival laceration, one should always consider the possibility of an occult globe rupture, laceration, or retained intraocular foreign body. A topical anesthetic agent should be instilled and the laceration carefully examined with particular attention to the underlying sclera. Conjunctival lacerations of less than 1 cm generally do not require surgical repair. Smaller wounds that are gaped as the result of tissue avulsion, or those with poor appositional closure, should be sutured closed. For larger conjunctival lacerations, closure may be obtained by good wound apposition and suturing with either absorbable or nylon sutures. Care is taken to avoid incarcerating Tenon’s capsule. Lacerations involving the plica, semilunar fold, or caruncle warrant restoration of normal anatomic relationships to prevent scarring and poor cosmesis.
CORNEAL LACERATIONS
With surgical repair of corneoscleral lacerations, the primary goal is to achieve a watertight globe and maintain structural integrity. Secondary goals include removing any disrupted lens fragments and vitreous, repositioning any uveal tissue, relieving vitreous incarceration, removing any intraocular foreign bodies, and restoring normal anatomic relationships. A methodic surgical strategy is essential for injury repair. Such a stepwise schema affords the surgeon a standard and reproducible approach to the protean manifestations of penetrating anterior segment trauma (Fig. 1).
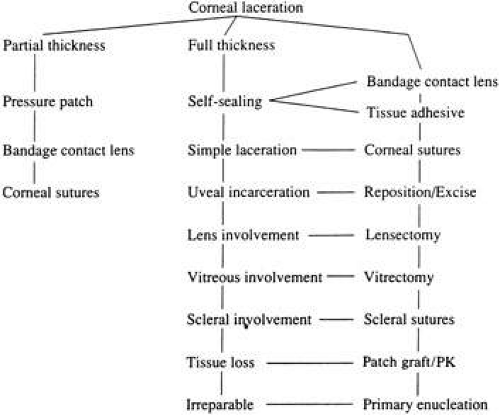 Fig. 1. Management flow chart for treatment of corneal lacerations. |
Partial-Thickness Corneal Lacerations
Corneal lacerations that appear to be nonperforating must be examined carefully to rule out any rupture of Descemet’s membrane. Seidel testing with 2% fluorescein should be performed to check for microscopic leaks. Gentle digital pressure may reveal a self-sealing wound. Such self-sealing wounds may be a result of stromal swelling when tears and aqueous come into contact with raw stroma. If the injury is indeed full thickness, treatment strategy is notably affected whereas partial thickness injuries may be treated on an outpatient basis, full-thickness lacerations are at risk for endophthalmitis and hospitalization with intravenous antibiotic usage may be considered.
The goals in treating partial thickness corneal lacerations include preventing infection and promoting re-epithelialization and stromal healing. Every effort is made to minimize scarring and surface irregularity. If the wound edges are in good apposition with no wound gape, pressure patching with the use of prophylactic topical antibiotics is sufficient. Re-epithelialization is usually rapid. If the wound is unstable, a bandage soft contact lens may be used to support the wound and encourage re-epithelialization by minimizing the traumatic effect of lid movement (Fig. 2). Topical antibiotic prophylaxis, as well as cycloplegia for comfort, is used while the lens is in place. The lens should remain in place until wound healing is stable and complete re-epithelialization has occurred.
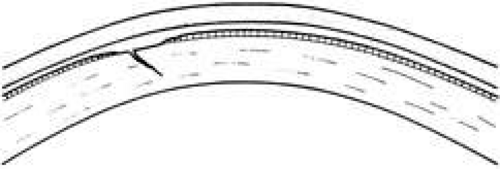 Fig. 2. A bandage soft contact lens supports the corneal wound and promotes re-epithelialization. For wounds that appose poorly or in which tissue is avulsed, sutures may be used to reapproximate the wound margins. In these settings, properly placed sutures will minimize scarring and perturbation of the ultimate surface corneal topography. Whenever possible, sutures should be placed outside the visual axis. |
Full-Thickness Corneal Lacerations
BANDAGE SOFT CONTACT LENS.
For small, self-sealing corneal perforations, a bandage contact lens may be sufficient to protect and support the wound as it heals. Such lacerations include nondisplaced, beveled, self-sealing wounds. If aqueous leakage persists for more than 24 hours or there is progressive shallowing of the anterior chamber, more definitive treatment should be undertaken. Treatment with a bandage contact lens in children should be done only with extreme caution and close follow-up care.
In cases that respond satisfactorily, the contact lens should be kept in place until the wound has stabilized (usually 3–6 weeks). A protective shield should be worn at all times. Topical antibiotic prophylaxis and cycloplegia are recommended with the lens in place.
TISSUE ADHESIVE.
Cyanoacrylate tissue adhesive has been successfully used by ophthalmologists for many years despite not being approved by the U.S. Food and Drug Administration. Tissue adhesive is particularly useful for puncture wounds with small amounts of central tissue loss and selected small lacerations.4
Tissue adhesive should be applied to a dry, deepithelialized bed. A capillary microapplicator or fine-gauge disposable needle is used to apply a very thin film of adhesive over the site (Fig. 3). Alternatively, adhesive may be applied using a sterile 2- to 4-mm polyethylene or silicone disc affixed to the end of an applicator stick with sterile ophthalmic ointment. The disc may be left in place or removed with care. Three to five minutes are required for polymerization of the adhesive. A bandage soft contact lens is applied for comfort and to prevent the glue from dislodging. While the contact lens is in place, a prophylactic antibiotic drop is administered. Over time, the tissue adhesive dislodges spontaneously as the wound surface reepithelializes. Alternatively, it may be gently removed with forceps after adequate stromal healing has occurred.
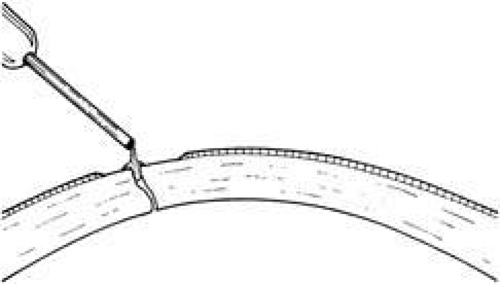 Fig. 3. After the wound bed is carefully de-epithelialized and dried, tissue adhesive is applied using a capillary microapplicator or fine-gauge disposable needle. Care is taken to use the minimum required amount of adhesive. |
SUTURE REPAIR OF SIMPLE CORNEAL LACERATIONS.
Most lacerating anterior segment injuries require the placement of corneal sutures. The primary goal of corneal suturing is to achieve a watertight wound. Secondary goals include minimizing scarring, restoring normal anatomic relationships, and reconstructing the normal corneal topographic contours. Local anesthesia may be used in selected cases. General anesthesia is used for more severe injuries or with an uncooperative patient, unless medically contraindicated. The affected eye is aseptically prepared and draped with caution to avoid any unnecessary pressure on the globe. To stabilize or manipulate the globe, 6-0 silk stay sutures may be placed at the limbus, 90 degrees away from the wound. Rectus bridle sutures may be passed as well, again taking care to avoid any pressure on the globe.
If the anterior chamber is formed and the wound is watertight, sutures may be placed directly without entering the anterior chamber with instrumentation. For a wound that is less stable, a viscoelastic may be irrigated into the anterior chamber either directly through the wound itself or through a separate limbal paracentesis incision (Fig. 4). This will aid in re-forming the anterior chamber, tamponade intraocular contents, and protect the corneal endothelium, iris, and lens. Balanced salt solution or air may also be used to re-form the anterior chamber. In most cases, a limbal paracentesis is preferred because it will minimize disruption of the wound edges and permit better access as the case proceeds.5 A 15-degree sharp microsurgical knife or MVR blade may be used to create the paracentesis, placing the incision 90 degrees away from the wound. If a very shallow or flat anterior chamber is present, extreme care should be taken to avoid damage to the iris or lens when constructing the paracentesis site.
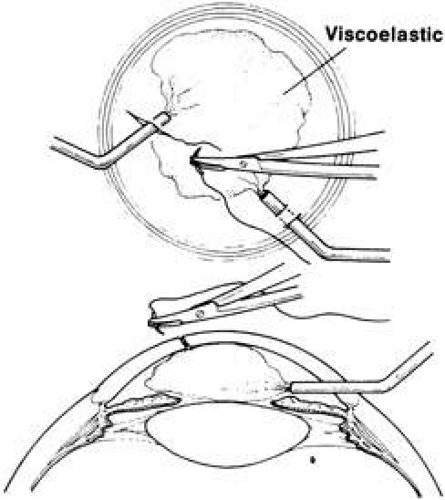 Fig. 4. Viscoelastic placed through the wound or paracentesis maintains the anterior chamber as temporary or definitive sutures are placed to stabilize the wound. |
Temporary sutures may be used if the initial placement of deep definitive sutures would cause loss/flattening of the anterior chamber. These temporary sutures should be placed without distorting the wound. Accurate placement of the final definitive sutures can be achieved subsequently. The number of temporary sutures should be minimized, however, to prevent undue trauma to the wound margins and surrounding stroma.
For corneal suturing, 10-0 monofilament nylon on a fine spatula-design microsurgical needle is used. This suture causes little tissue reaction, keeping vascularization and scarring at a minimum. Even finer 11-0 nylon suture may be used for lacerations near or involving the visual axis. Computed corneal topography analysis of corneal suturing techniques has suggested strategies designed to ensure adequate wound closure, minimize corneal scarring, and restore the native corneal contour.6,7
A number of options are available for suturing a corneal laceration. Tissue margins should appose as precisely as possible while suturing. The simplest method is to progressively halve the wound with simple interrupted sutures. Corneal sutures should be approximately 90% to 95% depth through the stroma, 1.5 mm in length, and of equal depth on each side of the wound. Shallow sutures create internal wound gape, whereas sutures of unequal length and depth on each side of the wound result in wound override. Sutures should generally not be passed through 100% thickness because the tract may theoretically act as a conduit allowing microorganisms from the external surface to enter the eye. For shelved lacerations, sutures should be placed equidistant with respect to the internal aspect of the wound and tied with minimal tension to achieve good tissue apposition, avoiding wound slippage with consequent tissue override (Fig. 5). Wounds with edematous or irregular margins generally require longer sutures for closure.
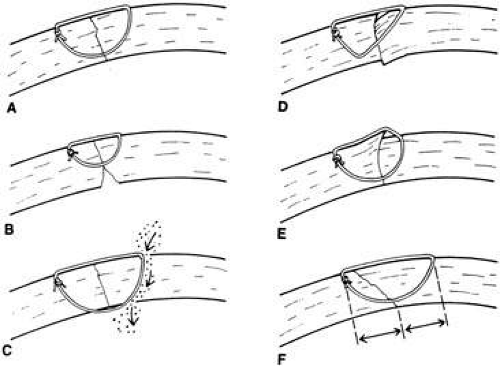 Fig. 5. Effects of suture placement for corneal lacerations. A. For sharp perpendicular wounds, deep suture placement equidistant from the wound margins gives excellent wound approximation. B. Shallow sutures create internal wound gape. C. Full-thickness sutures may create a conduit for microbial invasion. D. Sutures of unequal depth create wound override. E. Sutures of unequal length create wound override. F. For shelved lacerations, sutures should be placed equidistant with respect to the internal aspect of the wound to achieve good wound apposition. |
Placement of sutures through the visual axis should be avoided. If it is necessary to pass sutures near the visual axis, they may be placed on each side of, but not directly through, the axis itself. In addition, the bite closest to the visual axis may be made shorter, thus avoiding this area (Fig. 6). A “no-touch” technique also may be used to minimize trauma at the visual axis. With this technique, the eye is secured by grasping the globe with forceps away from the cornea. The suture needle end is then placed perpendicular to the corneal surface, and the needle is rotated through the corneal tissue following the needle’s curvature (Fig. 7).8
 Fig. 6. For lacerations affecting the visual axis, sutures should avoid the central cornea (A) by placing them on either side of, but not through, the axis or (B) by making the suture bites close to the visual axis short. |
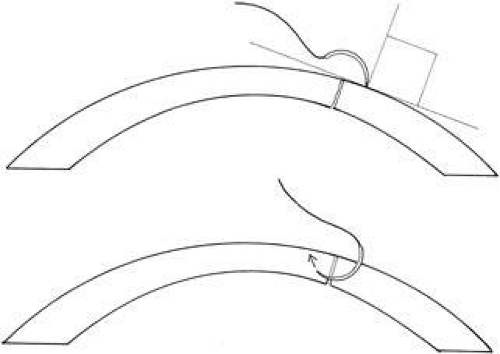 Fig. 7. Suture placement using a “no-touch” technique. Needle enters tissue perpendicular and is rotated by following the curvature of the needle. |
With more complex lacerations, good wound apposition with minimal distortion is the goal. An irregular wound is first subdivided into straight segments with interrupted sutures. Perpendicular areas of the laceration should be sutured before beveled ones to achieve watertight closure with the fewest number of sutures. As suggested by Rowsey and Hays,7 long, deep, and relatively tight peripheral wound sutures in combination with shorter, shallower, appositional sutures near the visual axis may help restore the normal corneal contour by restoring the relatively steep central corneal dome (Fig. 8). For irregular or curvilinear lacerations, all interrupted sutures should be placed perpendicular to the wound, thus avoiding transverse shifting of the wound margins. Although a running shoestring suturing technique may be used with straight lacerations to minimize astigmatism and facilitate subsequent suture removal, a running suture may tend to distort an irregular or curvilinear laceration because it will tend to form a straight line. Thus, if used, running suture bites should be placed perpendicular to and equidistant from an imaginary “regression” line through the wound rather than with respect to the wound itself (Fig. 9).
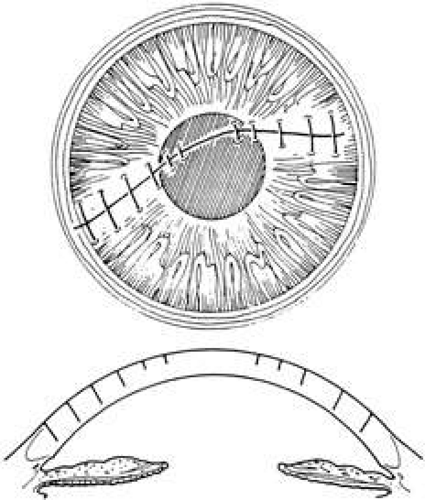 Fig. 8. Long, deep, and relatively tight peripheral sutures and shorter, shallower, appositional sutures near the central cornea may restore the normal corneal dome and surface topography. |
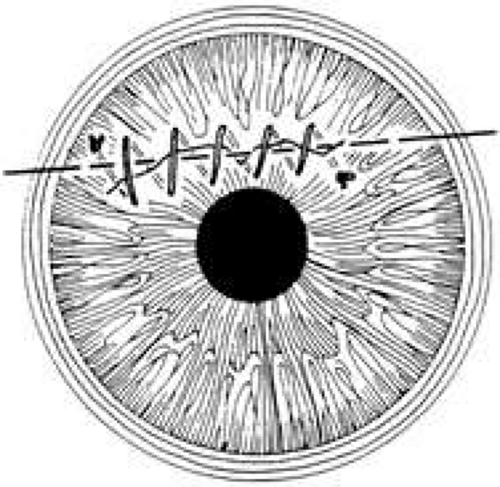 Fig. 9. When using a running suture for a nonlinear laceration, the suture should be placed with respect to a straight “regression” line approximating the wound to avoid distortion of the corneal topography. |
To facilitate subsequent suture removal from the cornea, a locked 2-1-1 knot or a 1-1-1 slipknot may be used. All suture knot ends should be trimmed short and then buried superficially on the side away from the visual axis. This minimizes scarring, inflammation, neovascularization, and buildup of mucus. The knot should be buried by directing the ends away from the surface to ease future removal (Fig. 10).
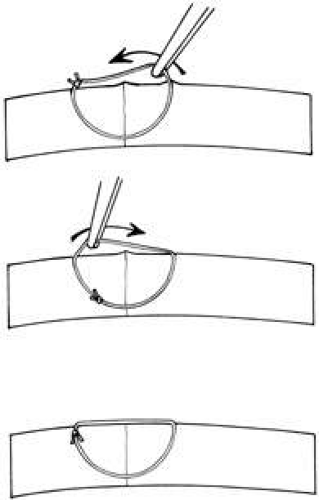 Fig. 10. Suture knot burial. A. Knot is trimmed short and rotated beneath the corneal surface using smooth forceps. B. Direction of knot is reversed, leaving knot end away from corneal surface. C. Knot is rotated back just beneath the corneal surface. |
Once the laceration is repaired, the anterior chamber should be deepened, preferably through the paracentesis port, if not through the wound itself. The wound is then checked for leaks using dry cellulose sponges or 2% fluorescein sodium. The paracentesis port is usually self-sealing; however, if it is leaking, stromal hydration using a canula or closure with a single interrupted 10-0 nylon suture may be necessary.
STELLATE CORNEAL LACERATIONS.
Stellate lacerations and partial tissue avulsions are often difficult to repair because it is difficult to obtain watertight closure. Good tissue apposition is often difficult to obtain. Several techniques may be used for stellate lacerations. These include multiple interrupted sutures, bridging sutures, pursestring sutures, and star-shaped sutures9. If closing a stellate laceration is difficult, and leaking persists, tissue adhesive or a corneal patch graft may be used (Fig. 11).
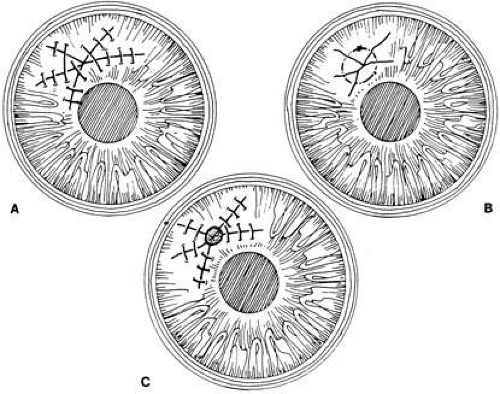 Fig. 11. Stellate laceration closed by (A) bridging sutures, (B) pursestring suture, and (C) multiple interrupted sutures and tissue adhesive. |
If an avulsed tissue pedicle is seen, it should be carefully replaced into position and sutured into place. Such avulsed tissue is best pulled into place by angling sutures toward the apex of the wound.6
CORNEAL LACERATIONS WITH UVEAL PROLAPSE.
Iris incarceration and prolapse are frequently noted conditions that accompany corneal lacerations. A peaked pupil signals tissue incarceration. If prolapsed tissue is present, it must first be carefully examined. Usually, macerated, feathery, devitalized, or depigmented iris should be excised. The prolapsed tissue should be evaluated for any signs of surface epithelialization. In this case, it should be excised to prevent any epithelial cells from proliferating in the anterior chamber. In general, tissue that has been prolapsed for longer than 24 hours should be excised to avoid infection; however, if the tissue appears healthy, it may be replaced with caution. Any tissue to be excised should be gently grasped with fine forceps without applying undue traction. The tissue is then cut flush with the cornea. When excising any tissue, every effort is made to preserve as much as possible to maintain a normal iris diaphragm and conserve tissue for secondary reconstructive efforts.8
Incarcerated tissue will usually require mechanical reposition. Selected cases of mild incarceration may be treated with pharmacologic agents. Agents such as intraocular acetylcholine or carbachol cause pupil constriction, thus pulling iris from the wound. If incarcerated iris is located in the central cornea, mydriatic agents (e.g., intraocular epinephrine 1:10,000) may be used. If mechanical reposition is required, simply deepening the anterior chamber may release incarcerated tissue. Viscoelastic agents may be irrigated through the paracentesis port or the wound adjacent to the involved iris tissue in an attempt to draw the incarcerated iris from the wound (Fig. 12). If unsuccessful, a cyclodialysis spatula or irrigating canula may be passed through the paracentesis site and used to directly sweep incarcerated tissue free (Fig. 13). Care is always taken to avoid trauma to the corneal endothelium, iris, and lens. Any excised tissue should be sent to the pathology department for examination.
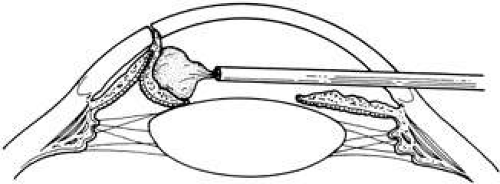 Fig. 12. A viscoelastic is used to drive incarcerated tissue from the wound. |
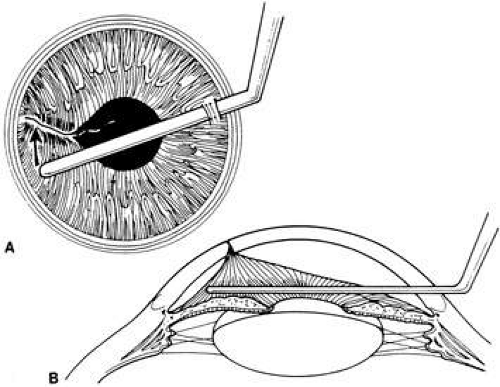 Fig. 13. A spatula is used to mechanically sweep incarcerated tissue from the wound. The anterior chamber is maintained with viscoelastic during the maneuver. |
Once incarcerated or prolapsed tissue is excised or repositioned, the corneal laceration is sutured as described earlier. Careful inspection is warranted once closure is complete to ensure that no tissue incarceration persists. The anterior chamber should be filled through the paracentesis site, and wound integrity should be ascertained.
CORNEAL LACERATIONS WITH LENS OR VITREOUS INVOLVEMENT.
Perforating injuries may also have lens and vitreous involvement. Direct and indirect forces may damage the lens capsule, causing cataract formation. Penetration or rupture of the lens capsule often leads to lens opacification. Blunt trauma may result in globe distortion with equatorial expansion, which can cause capsular rupture or result in dehiscence of zonules with consequent lens subluxation or dislocation. Vitreous may find its way around the lens into the anterior chamber when loss of zonules occurs. Careful preoperative and intraoperative assessment will dictate whether lens removal is required at the time of primary repair. Removal of a cataractous lens rarely needs to be done in the emergency setting. In particular, there are some situations in which lens removal in the acute setting is not recommended. For instance, a fibrinous anterior chamber reaction and pupillary membrane may occasionally masquerade as a flocculent cataract10 or poor visualization secondary to an edematous cornea may make intraocular surgery hazardous. However, if surgical visualization is good, it is preferable to complete all surgical interventions at one setting.11 If any doubt regarding lens clarity exists, the lens should be left in place and, if necessary, removed at a later date. There are other situations in which primary removal of the lens is indicated. A lens with a disrupted capsule and flocculent cortical material liberated into the anterior chamber should be removed at the primary setting in an effort to prevent phacogenic postoperative inflammation. In cases in which vitreous is involved with lens remnants, this may be best addressed in the initial surgery. In addition, when it is clear that a lens is cataractous and surgical visualization is good, the lens may be removed in the primary operation.12,13 Lens removal should take place only under controlled circumstances with proper instrumentation. A cataractous lens with an intact capsule and no liberated cortical material may be removed at a later date.
With lens removal, attention should first be paid to any prolapsed or incarcerated tissue. This should be repositioned or excised, and the corneal laceration should be sutured and the anterior chamber re-formed as described. The nature of the injury will suggest the surgical technique used for lens removal. If the lens capsule remains intact, standard phacoemulsification or extracapsular cataract extraction may be performed, making every effort to preserve the integrity of the posterior capsule. In children and young adults, a soft cataractous lens may be removed through a small incision using manual or automated aspiration. When extracting the nucleus in the patient post-trauma, one should be aware of the possibility of poor zonular support. Should zonular weakness, dialysis, or loss be present, a capsular tension ring (CTR) may be used. Implanting a CTR may decrease intraoperative zonule dehiscence, subluxation of the capsular bag, and posterior capsular rupture. A CTR inserted before phacoemulsification will permit support of the capsular bag, reestablishing its contour and protecting it from getting aspirated.14 The CTR (Morcher; distributed by FCI Ophthalmics, Inc., Marshfield Hills, MA) comes in three sizes and is usually inserted after capsulorrhexis and hydrodissection. For insertion, it is best to enter the bag in the area of greatest zonular weakness, thus placing stress on the stronger zonules, 180 degrees away. The ring is dialed into the bag using a second instrument (e.g., Y-hook) (Fig. 14). Alternatively, a CTR injector may be used.
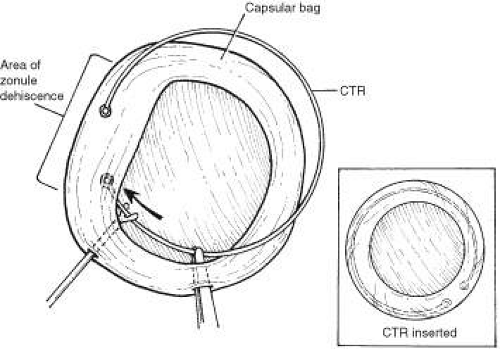 Fig. 14. Capsular tension ring (CTR) is guided into the capsular bag by Y-hook and is directed toward the area of zonular weakness. CTR inserted (inset). |
If the lens capsule is ruptured, vitreous is involved, or the lens is subluxated or dislocated, microvitrectomy instrumentation should be used, because caution must be taken not to exert vitreous traction during lens removal. This may be performed through either a limbal or pars plana approach, depending on the surgeon’s preference. It is important to remove all lens fragments from the anterior chamber, using caution to prevent any remnants from receding into the vitreous chamber. Any vitreous remaining in the anterior chamber should be removed to prevent incarceration into the wound.
Intraocular lens implantation in the primary trauma setting is a controversial area; however, generally it is associated with a more favorable visual outcome.12,13 The patient’s age, the visual and refractive status of the fellow eye, and the ability to use an aphakic contact lens postoperatively are factors in the decision. If the posterior capsule is intact, and the patient’s age is appropriate, a posterior chamber intraocular lens may be implanted. Currently, intraocular lenses are used at a much younger age. In cases in which there is inadequate capsular support, posterior chamber lenses may be supported by transscleral or iris sutures (Fig. 15). 15,16 An anterior chamber lens may also be placed in the absence of capsular support after all vitreous and lens remnants are removed. These should likely be reserved for older patients; however, intraocular lens implantation should not be performed if visualization is poor or the eye is severely inflamed and may be deferred if secondary anterior segment reconstructive surgery is anticipated. Moreover, although intraocular lens placement may be preferable in some patients, contact lens correction may afford a better optical result in those patients with irregular astigmatism from a corneal scar.17
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


