10

Surgical Approaches: Endonasal
Endoscopic
Stammberger,1 Messerklinger,2 Wigand,3 and Kennedy and colleagues4,5 created a revolution in the thinking and surgical management of nasal sinus disease. The ability to use nasal endoscopy for the diagnosis, identification of sinus and nasal pathology within the narrow spaces and recesses of the nose, and delicate management of the disease has benefited the patient by more accurate surgery, preservation of function, and faster healing. From its introduction, the concepts of endoscopic sinus surgery continue to evolve because of increased understanding of the anatomy, improved endoscopes and video equipment, newer instrumentation, and improved technology.
The author’s previous surgical concepts were described in a prior textbook, but they have since evolved as the concepts have changed and the technology has improved.6 Although some of the principles and concepts remain the same, many others are different.
Although sinus surgery with endoscopes was initially called functional endoscopic sinus surgery (FESS), many would agree that this nomenclature is often misused because not all of the surgery is truly “functional.” Because all of the surgery is endoscopic, it is appropriate to use the more general term endoscopic sinus surgery and realize that there are several types of procedures done in this manner. For all sinus surgeons there is a spectrum of procedures performed. At times the surgery is certainly “functional,” and FESS is an appropriate term. There may be minimal disease, disease confined to the anterior or posterior ostiomeatal complex or nasal cavity. During FESS, the nasal and sinus mucous membrane lining, nasal turbinates, and sinus ostia mostly are preserved or nearly totally preserved. In other patients, there is extensive disease involving all of the sinuses, nasal turbinates, or nasal sinus mucous membranes. There may have been previous surgery or disease that has destroyed normal anatomy and/or sinus lining, leaving a scarred and distorted nasal sinus cavity. In these instances, the goal cannot be to re-create sinus function. Rather, the goal is to eradicate disease by creating a single large cavity that permits adequate aeration into the sinuses and adequate egress of mucus. Here, a marsupialized cavity is created. The author has called this marsupialization endoscopic sinus surgery (MESS). In between FESS and MESS there is a spectrum of operations depending on the pathology found.
 Preparation for Surgery
Preparation for Surgery
Surgery is indicated for those patients who have medically unresponsive sinus disease, a complication of sinus disease such as orbital abscess, or an intracranial complication such as meningitis or abscess. Prior to surgery, all patients have had a nasal endoscopic evaluation and CT scan of the sinuses. The nasal endoscopic exam not only helps to identify the pathology, but also helps determine the areas of technical difficulty in performing an endoscopic sinus procedure. The CT scan used is a coronal CT visualizing the sinuses from the anterior wall of the frontal sinus through the posterior wall of the sphenoid sinus. Axial scans are occasionally obtained when frontal or sphenoid sinus pathology is seen. These axial CT scans aid in the endoscopic surgical management by determining the anterior to posterior dimensions of the sphenoid or frontal sinuses.
Patients avoid the use of any medications that may alter blood coagulation (e.g., aspirin, nonsteroidal anti-inflammatory drugs, or vitamin E) for at least 1 week prior to surgery.
 The Operating Room
The Operating Room
Patients are positioned on the operating table with a pillow placed under the knees to reduce strain on the lower back. In an effort to reduce bleeding and keep the blood pressure lowered, the head is slightly elevated, a soft roll or pillow is placed under the base of the neck, and the head rests upon a soft “doughnut” to bring the head and neck into a head forward sniffing position (Fig. 10–1).
The surgeon stands at the patient’s side and operates from the monitor (the author is left-handed and therefore stands on the patient’s left side) (Fig. 10–2). A Mayo stand with the most frequently used surgical instruments is at the head of the table. The scrub assistant stands opposite the surgeon, with the remainder of the instruments on the back table just behind the scrub technician. The video system cart with monitor, digital camera, recording, and still photographic capability is just above the Mayo stand. Image-guided triplanar localization surgical technological systems are just to the side of the video cart (Fig. 10–3). The anesthesia team sits with their equipment at the patient’s side. The CT scan is on an x-ray view box in full view of the surgeon for reference during the surgical procedure. The intravenous fluids and ports are located on the side closer to the anesthesia team for easy access. The blood pressure cuff is on the opposite side on the arm by the surgeon.
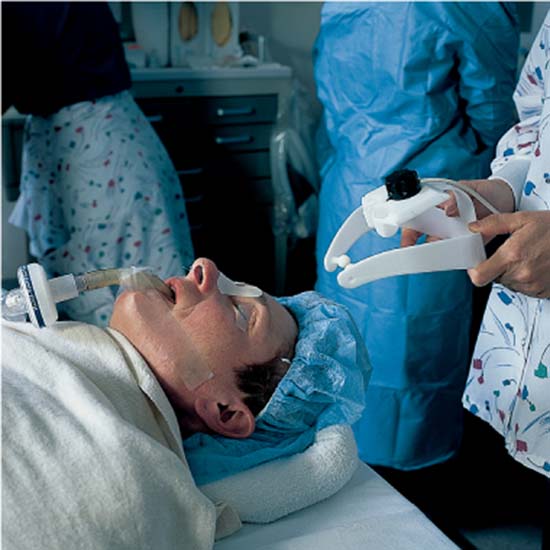
FIGURE 10–1 Positioning of the patient at the time of endoscopic sinus surgery, with the head slightly elevated and on a soft “doughnut” pillow. A pillow is placed beneath the knees.

FIGURE 10–2 Organization of the operating room for endoscopic sinus surgery with the surgeon to the side, the anesthesiologist and operating room nurse opposite the surgeon and instruments at the head of the patient.

FIGURE 10–3 The CT scan is in view of the surgeon. The monitor off of which the surgery is done is at the head of the patient, and the computer-assisted navigational monitor (Visualization Technology Inc. [VTI], Wilmington, MA) is next to it. The surgeon in this case is left-handed and therefore stands at the left side of the patient.

FIGURE 10–4 The laryngeal mask airway is inserted from the head of the patient.
Nearly all cases are done under general anesthesia, which is chosen for several reasons. This is easiest especially for revision cases where there may be a great deal of scar tissue, making a regional block difficult. Intubation or laryngeal mask airway (LMA) protects the airway, especially in the patient with reactive airway disease, in which a small amount of blood in the trachea may cause bronchospasm (Figs. 10–4, 10–5). (LMA is presently used in nearly all patients. It minimizes bronchospasm in the patient with reactive airway disease and seems to allow blood pressure to remain lower and more controlled with minimal use of medications. After several hundred patients undergoing ESS with LMA, no patient has had aspiration.) General anesthesia is valuable for those patients undergoing image-guided surgery, during which a headpiece is worn; it is imperative that there be minimal head movement during such surgery.

FIGURE 10–5 The laryngeal mask airway fits over the larynx and the hypopharynx and can be inflated appropriately to seal the laryngohypopharynx.

FIGURE 10–6 A separate table is set up with topical decongestants and injectable local anesthesia (if needed) so that the nose may be prepared prior to the surgeon scrubbing.
Once the patient is asleep, the endotracheal or LMA tube is secured to the lower lip and jaw, taking care to keep tape away from the nose, which might hamper visualization of the nasal/sinus cavity. The eyelids are taped closed to prevent corneal injury, and the eyes are left un-draped in the field of surgery as a reference.
Prior to scrubbing, the surgeon uses a headlight and nasal speculum to decongest the nose using oxymetazoline (Fig. 10–6). The oxymetazoline is colored with gentian violet to prevent its being confused with another solution on the operating table. Neurosurgical cottonoids are soaked in the oxymetazoline and placed medial to the middle turbinate, in the region of the anterior ostiomeatal complex and along the inferior turbinate. These are left in place with their strings extending out from the nares until after the surgeon has scrubbed and the patient has been draped. The patient’s face and nose are not prepped because the inside of the nose is laden with bacteria and cannot be adequately sterilized. (In several thousand cases, the author has not seen any postoperative infection caused by lack of facial preparation.)
Once the oxymetazoline has produced adequate vasoconstriction, the patient has been draped, and the blood pressure is in the range of less than 100 mm Hg systolic, the procedure is begun. The nasal cavity is initially examined with a 0-degree, 4 mm endoscope. Xylocaine 1% with 1:100,000 epinephrine is injected into the region of the uncinate process and attachment of the middle turbinate. The anesthetic is injected slowly and allowed to flow posteriorly into the ostiomeatal complex (Fig. 10–7). The injection is used not because of the anesthetic but rather because of the vasoconstriction the epinephrine produces. Preoperative photographs are taken of the anterior ostiomeatal complex and any pertinent pathology. These intraoperative photographs are kept as part of the patient’s office record and referred to during subsequent follow-up visits. These photographs (combined with a photograph taken at the end of the procedure) provide a valuable reminder to the surgeon of what was found and what was accomplished at surgery.
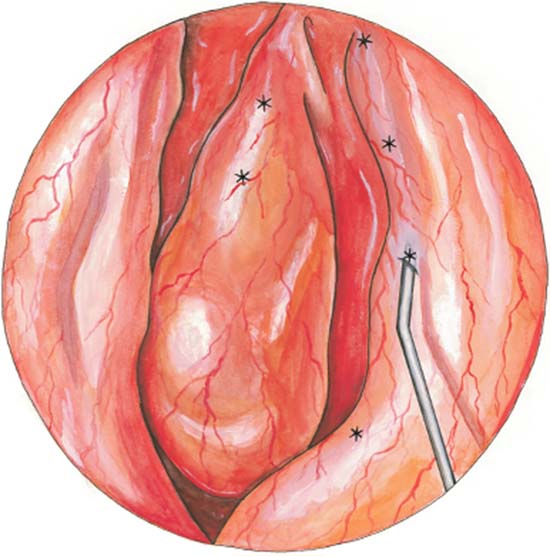
FIGURE 10–7 Injection of local anesthesia for vasoconstriction into the anterior ostiomeatal complex.
 Nasal Septal Surgery
Nasal Septal Surgery
If a deviated nasal septum is present, obstructing the nasal cavity and limiting the nasal airway or access to the sinus cavities, a septoplasty is performed prior to beginning the sinus surgery. The septoplasty is performed in a traditional manner or with a microshaver, removing bony spurs as needed. Following the septoplasty, cottonoids with oxymetazoline are placed in the nose while the instruments are changed over from the septoplasty to the sinus surgery. These cottonoids provide additional vasoconstriction and minimize the edema along the nasal septal flap that occurred from the septal surgery.

FIGURE 10–8 The Xomed XPS microshaver is used for the majority of endoscopic sinus surgeries.
 General Principles of Endoscopic Sinus Surgery
General Principles of Endoscopic Sinus Surgery
Most endoscopic sinus surgery is done using the Xomed XPS microshaver (Medtronic Xomed, Jacksonville, FL) (Fig. 10–8). The microshaver is delicate and provides accurate and atraumatic tissue removal. Bleeding is minimal. Normal mucosa is better preserved while pathologic tissue is removed. The irrigating system that is an integral part of the Xomed microshaver minimizes the blockage in the system and permits ease and efficiency of use. The attached suction draws bone and soft tissue into the blade. An additional irrigating system (Clear-ESS) (SLT Laser, Mongomeryville, PA) is added to the microshaver (Fig. 10–9). Saline is used either continuously or intermittently, as determined by the surgeon. through trumpet-type control valves on the endoscope, to irrigate away secretions or blood. Several blades and burs are available and used, depending on the pathology and its location. A 4.2 mm Tricot blade is used for most of the procedure. When disease is present in the frontal recess, frontal sinus, or maxillary sinus, a 40- or 60-degree angulated Tricut blade is used. These blades are used in an oscillating mode at 1500 rpm. This is slow enough to permit the suction to draw tissue into the blade opening. It is generally used for polyps, soft tissue, and thin bone. When a moderate amount of thin bone is present, the microshaver is used at 3000 rpm to enhance the bone-cutting capacity. The mode can be shifted into a continuous mode to cut through thin to medium bone.
Straight burs with one side protected or 55-degree burs permit access into the heavier bony areas of the frontal or sphenoid sinus. The burs are used in a continuous mode generally at 5000 rpm.

FIGURE 10–9 The Clear ESS system can be attached to the microshaver, permitting intermittent or continuous irrigation of blood and/or debris from the sinus cavity.

FIGURE 10–10 Collection of the specimen in the “sock” within the operating room suction apparatus.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


