1

Surgical Anatomy of
the Paranasal Sinus
The paranasal sinus region is one of the most complex areas of the human body and is consequently very difficult to study. The surgical anatomy of the nose and paranasal sinuses is published with great detail in most standard textbooks, but it is the purpose of this chapter to describe those structures in a very clear and systematic presentation focused for the endoscopic sinus surgeon.
A thorough knowledge of all anatomical structures and variations combined with cadaveric dissections using paranasal blocks is of utmost importance to perform proper sinus surgery and to avoid complications. The complications seen with this surgery are commonly due to nonfamiliarity with the anatomical landmarks of the paranasal sinus during surgical dissection, which is consequently performed beyond the safe limits of the sinus.
The sinus surgeon must be able to orientate himself or herself while looking through optical instruments that provide better illumination and a greater view of the delicate structures of the nose and paranasal sinus. The surgeon must also develop a mental three-dimensional anatomical image, allowing himself or herself to know the precise location, the relationships with vital structures, and especially where the danger points lie.
Besides clinical judgment and technical skills, a competent surgeon must also be a good anatomist. To achieve these goals, it is wise to perform a reasonable number of surgical dissections on cadaveric specimens, attend several dissection courses, and participate in many meetings. During the past years the author has organized international dissection courses on paranasal sinus surgery with limited numbers of participants. This is the best way to improve medical teaching, hospital practice, and patient care.
This chapter is divided into three sections: developmental anatomy, macroscopic anatomy, and endoscopic anatomy. A basic understanding of the embryogenesis of the nose and the paranasal sinuses facilitates comprehension of the complex and variable adult anatomy. In addition, this comprehension is quite useful for an accurate evaluation of the various potential pathologies and their managements. Macroscopic description of the nose and paranasal sinuses is presented through a discussion of the important structures of this complicated region. A correlation with intricate endoscopic topographical anatomy is discussed for a clear understanding of the nasal cavity and its relationship to adjoining sinuses and danger areas. A three-dimensional anatomy is complemented with schematic diagrams.
 Developmental Anatomy
Developmental Anatomy
Nose Development
The embryogenesis of the nose and paranasal sinuses is related to the regional embryology of the cranial-oral-facial region. These primary events occur between the fourth and eighth weeks of fetal life. The first nasal structures are initially identifiable in the 5 mm, 4-week-old embryo.1,2 At this point, there are three developing facial projections that contribute to the formation of the nose: the frontonasal process, the maxillary process, and the mandibular process.
The frontonasal process is ectodermally derived, and it develops independently over the forebrain giving rise to the forehead and the nasal olfactory placodes. A thickened plaque of ectoderm develops during the fourth intrauterine week on each side of the ventral surface of this frontonasal elevation. Within a few days these thickenings become paired lateral nasal placodes (Fig. 1–1). Initially the placodes have a convex external surface, but the unequal forward growth of the frontonasal swelling (particularly the medial and lateral sides of the nasal placodes) will transform these surfaces into concave nasal grooves. These grooves are well developed when the embryo is 32 to 34 days old. They are surrounded by the medial nasal swelling at the medial side of the nasal placode and the lateral nasal swelling at the lateral side of the nasal placode.3
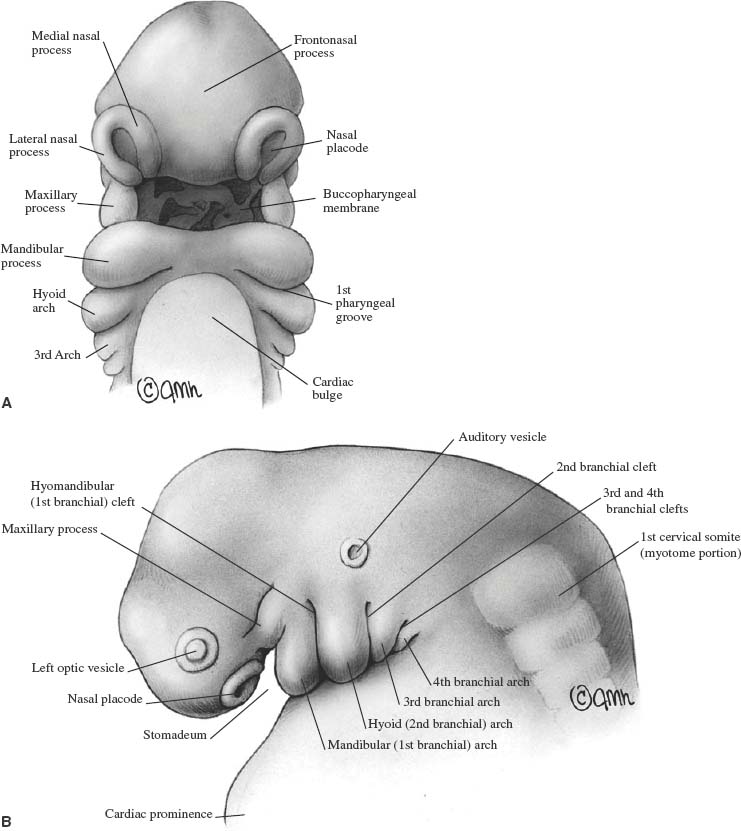
FIGURE 1–1 Embryo at 4 to 5 weeks. (A) Frontal view: Observe the branchial arch formation and the ruptured buccopharyngeal membrane. (B) Lateral view.
Meanwhile, other outgrowths of mesenchymal origin called the maxillary processes grow ventrally from the dorsal ends of the mandibular processes (first visceral) arch. These maxillary swellings are located at the inferolateral border of the placodes. These three swellings are separated from each other by shallow depressions and continue to grow forward and downward. As they do so, the epithelial linings of the medial and lateral nasal swellings fuse inferiorly, and the nasal grooves become blind-ending tubes or pits, called the nasal pits, that will ultimately become the nares. The epithelium within the pits eventually develops neural processes that extend toward the brain to become the olfactory nerves. Thus, the development of the nasal pits is part of the cranial and neural tube formation.
The floor of each nasal pit is constituted by the fused medial and lateral nasal swellings and further anteriorly by the fused medial nasal and maxillary swellings. The epithelial lining in the contact plane is called the nasal fin and is disrupted anteriorly by the outgrowth of the surrounding tissues. Posteriorly, this epithelial band persists for a short period of time in the floor of the nasal pit. As the nasal pit deepens, it becomes the nasal sac. As the cavity enlarges, the posterior limiting membrane (initially the nasal fin) becomes the oronasal membrane.
During the forward and downward growth of the various facial swellings, each swelling also increases its dimensions in a mediolateral direction. Thus, during the transformation of the nasal groove into the primary nasal cavity, the furrows between maxillary and lateral nasal swellings are increased, both on the external surface and on the internal surface of the lateral wall of the primary nasal cavity. The early structures responsible for the development of the eyes are visible at 28 days. Initially, the early eyes are oriented laterally (80 degrees to the neural axis), but during the next weeks the growth of the mesenchyme posterior to the eyes reorients the eyes forward toward the midline. The groove on the external surface is transformed into the nasolacrimal duct by the interposition of surface epithelium between the maxillary and lateral nasal swellings and by the loss of contact between this epithelium and the surface epithelium. It is like an infolded epithelial transformation. The groove on the inside surface will develop into the inferior meatus of the nasal cavity. The nasolacrimal duct connects the eye to the internal nasal cavity inferior to the attachment of the inferior turbinate. As the eye migrates from a lateral orientation relative to the developing nose, the nasolacrimal duct assumes a more oblique rather than horizontal direction (Fig. 1–2).
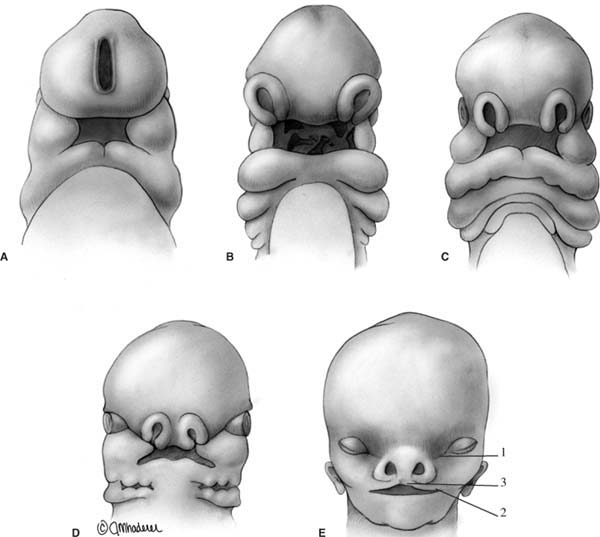
FIGURE 1–2 Developing face. (A) Fourth week. (B) Fourth to fifth week. (C) Fifth to sixth week. (D) Sixth to seventh week. (E) Eighth to tenth week. Note the orientation of the eyes forward and toward the midline, the nose development, the sealing of the nasolacrimal groove (1), and the formation of the upper lip (2) and the philtrum (3).
The rupture of the oronasal membrane in the 15 mm embryo takes place between days 42 and 44 in the posterior floor of the nasal pit, transforming this blind-ending cavity into a primary nasal cavity that communicates with the primary oral cavity through the newly formed opening, or primitive choana.1–3 Lack of disintegration of the oronasal membrane results in choanal atresia. The part of the roof of the mouth in front of the choana is the premaxilla (primitive palate). The external nares are widely separated by the remaining median frontonasal process, which gradually reduces, bringing the openings close together.
Embryonic Part | Facial Derivatives | Skeletal Derivatives |
Frontonasal process | Nasal bridge | Nasal bones |
Median nasal process | Columella of nose | Perpendicular plate of the ethmoid bone |
Philtrum | Vomer | |
Lateral nasal process | Sides and ala of nose | |
Maxillary process | Major portion of upper lip | Maxilla, zygoma, secondary palate |
Upper cheek | ||
Mandibular process | Lower lip, Lower cheek | Mandible |
Simultaneously, other facial structures develop rapidly. The digestive tube is formed, and the cephalic opening of this tube, called the oral stoma, is found just caudal to the level of the nasal pits. The branchial clefts and arches form ventral to the eyes and caudal to the oral stoma. The maxillary process, derived from the first branchial arch with part of the medial nasal process, becomes the upper jaw (Table 1–1).
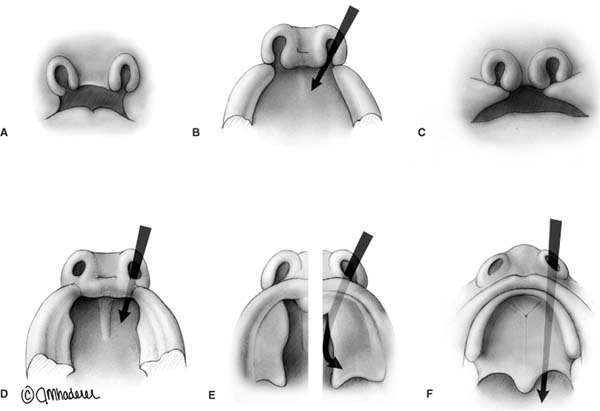
FIGURE 1–3 Development of the nose, mouth, and palate. (A–C) Formation of the nose, upper lip, and philtrum. (D–F) Different stages of palate formation and the separation of the nasal and oral cavities.
From days 45 to 48 formation of the secondary palate begins, due to the separation between the nasal cavity and the oral cavity. By that time, vertical projections from the maxillary process, named palatal shelves, are identified. The palatal processes are located along the lateral aspect of the tongue, but as the tongue descends, they develop horizontally toward each other. The secondary nasal cavity is thus formed. The palatal closure progresses from anterior to posterior, and by days 63 to 70 the palatal shelves have fused along most of their length (Fig. 1–3). Only the area between the junction of the premaxilla and the palate remains incomplete during the prenatal life and thereafter. This persistent communication at the anterior palate is the incisive canal, which carries vessels and nerves between the nose and the mouth.4
The posterior choana is repositioned more posteriorly due to the development of the secondary nasal cavity and the formation of the palate. Also, the developing nasal septum fuses with the palatal shelves, creating two separate right and left nasal cavities. The precise timing of these events is subject to individual variations and possibly also to sexual and racial ones.5 However, early in this stage the definitive nasal cavities are formed, and a cartilaginous frame begins to provide support to the nasal region as well as primary skeletal protection.
The nasal capsule is a cartilaginous envelope that encases the developing nasal structures and is part of the developing skull base (Fig. 1–4). This mesodermal structure forms a boundary to the nasal and paranasal sinus development. The paranasal cellular growth either is limited to the bounds of the perichondrium of the nasal capsule or extends beyond the borders of the perichondrium with reabsorption of the cartilaginous cells. This is the situation created by the development of the maxillary, frontal, and sphenoid sinuses beyond the ethmoid complex.
The developmental origin of the cartilaginous nasal capsule is unclear and subject to controversy.6,7 It is possible that the mesenchyme (the loose embryonic mesodermal tissue) is directed by the neural crest cells, arising at the junction of the neural tube and ectoderm and streaming out into the mesoderm. The resulting mesoderm is then termed head mesenchyme.
The process of chondrification of the nasal capsule begins within the head mesenchyme with the lying down of chondroitin (the intercellular matrix). The fibrovascular tissue on the periphery of the nasal capsule is the perichondrium, which provides the nutrients to be diffused to the chondrocytes (cartilage cells). This induced process of chondrification starts in the cranial base at the anterior aspect of the sphenoid bone. The nasal capsule begins to chondrify after the chondrocranium at the level of the nasal septum sometime during the middle of the third prenatal month. Cartilage formation in the lateral ethmoid bone starts in the fourth month and extends to the anterior or caudal area of the nose and septum, and subsequently to the dorsal part of the nasal capsule.
The process of ossification of the nasal capsule involves two mechanisms of bone formation: endochondral and membranous. Endochondral bone formation is related to the layered deposit of bone matrix along the perichondrial blood vessels that invade the cartilaginous tissue. Simultaneously, the cartilage is resorbed. The cells that form along these vessels are called osteocytes and have their own supply vessel. The compacted fibrovascular tissue at the periphery of this process of ossification becomes the periosteum. Membranous bone is the result of laying down bone matrix directly from periosteal cells without a preceding formation of cartilage.
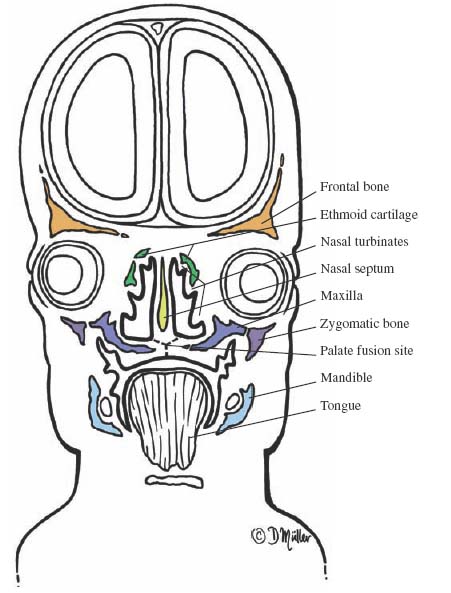
FIGURE 1–4 Eight- to 10-week embryo (coronal section) showing early development of the nasal capsule, including the lateral nasal wall and the turbinates.
Paranasal Sinus Development
The embryological development of the paranasal sinus is a very complex process, and its description varies among different authors. The growth pattern of the paranasal sinus is totally unpredictable and extremely variable from one individual to another, or even from side to side in the same person.8
The initial development of the nasosinus cavities takes place early in fetal life, occurring at the same time as the growth of the palate below, facial structures anteriorly, and the cerebral cranium above. The paranasal sinuses, with the exception of the sphenoid sinus, arise as evaginations from the lateral nasal wall.
At the begining, the lateral nasal wall is a smooth, undifferentiated structure, but during the seventh gestational week it starts to develop. A projection into the nasal capsule just superior to the palatal shelves appears first and is called the maxilloturbinal. It is followed by five other ethmoturbinals and the nasoturbinal. However, through reposition and fusion three to four ridges ultimately persist4,9,10 (Fig. 1–5).
The maxilloturbinal forms the inferior turbinate, which is not considered ethmoid in its embryological origin. The first ethmoturbinal originates at either the superior aspect of the septum or the superior junction of the septum and the lateral nasal wall, and it gives rise to the middle turbinate. The furrow between the maxilloturbinal and the first ethmoturbinal eventually develops into the middle nasal meatus. It is at the primitive middle meatus that, during about the 13th week of development, an evagination of the lateral nasal wall produces a blind diverticulum: the embryonic infundibulum. The infundibulum is formed by a cord of epithelial cells that is surrounded by the underlying mesenchyme. On either side of this structure, the mesenchyme proliferates, deepening the infundibulum. The second ethmoturbinal develops shortly after the first ethmoturbinal and ultimately forms the superior turbinate. The furrow between the superior turbinate and the middle turbinate is the superior meatus. The third ethmoturbinal is the precursor of the supreme turbinate, which is present in only 26% of adults.11 The supreme meatus is the furrow between the superior and the supreme turbinates. All of these structures are considered to be ethmoid in their origin.
The nasoturbinal is an additional prominence anterior and superior to the ethmoid furrow or middle nasal meatus and will develop into the agger nasi. At about the same time it is identified another mesenchymal ridge, called the uncinate process, develops on the superior and posterior border of the agger nasi. The uncinate process may extend superiorly to the roof of the anterior ethmoid bone and posteriorly along the superior surface of the inferior turbinate.
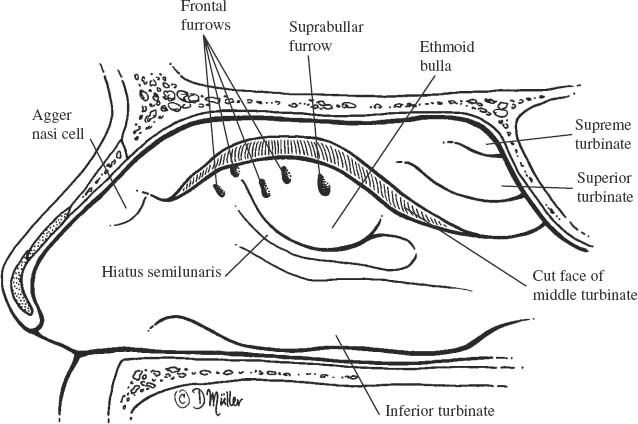
FIGURE 1–5 Right nasal wall of a neonate showing the turbinates and the agger nasi. The middle turbinate has been removed to present the anatomical structures of the middle meatus.
All craniofacial structures (at first made of cartilage, then of bone) that are adjacent to the infundibular region are subject to penetration by the process of evagination and reabsorption. The maxillary bone, frontal bone, ethmoid bone, and nasoturbinate bone (agger nasi) are invaded and filled with air from the ethmoid cells. This process is called primary pneumatization. It is followed by secondary pneumatization, during which these epithelial-lined pockets expand into the adjacent bony structures for which the sinuses eventually will be named. Primary pneumatization occurs during the chondrocranial stage. Much of the secondary pneumatization takes place postnatally.
Generally, the sinuses are established in prenatal life, with the shape of each sinus being regular in appearance and somewhat “globular.” The overall development of the paranasal sinuses is slow for the first 6 years of life, but after that age the speed of growth increases and the shape becomes irregular due to the distorting effects by the growing adjacent bony structures, including the other paranasal sinuses. By age 12 to 14, most of the sinuses have reached the adult size, but some sinuses continue to grow into late adulthood.10,12
Maxillary Sinus Development
The maxillary sinus is the first to develop during human fetal life, roughly during the 10th week. The maxillary sinus begins to form from an outpouching of the lateral wall of the ethmoid area of the nasal capsule within the infundibulum and immediately posterior to the developing uncinate process.13,14
This outgrowth enlarges slowly throughout fetal life due to the constriction by the perichondrium of the nasal capsule, limiting extension into the maxillary process (maxilla). Thus, the maxillary sinus appears as a slit, caught between the developing ethmoid cells, the inferior turbinate, and the bone of the maxilla. Only as the nasal capsule is resorbed during its ossification does the maxillary sinus have an opportunity to enter the developing maxillary process. As the maxillary sinus expands into the maxilla, it is restricted by dental development. Further growth of the maxillary sinus into the maxilla follows the development of the maxilla and the descent of the teeth (Fig. 1–6).
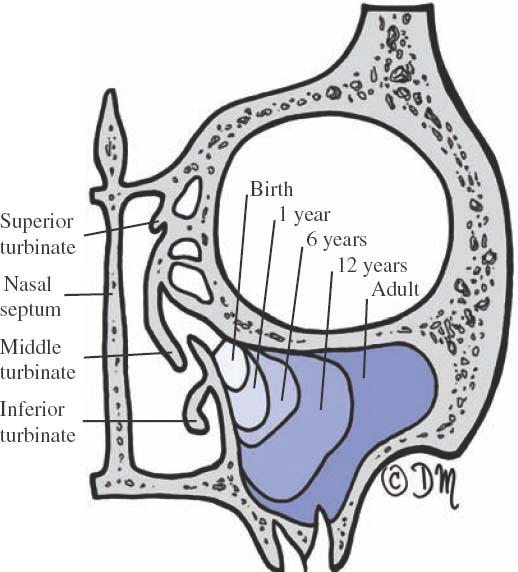
FIGURE 1–6 Developmental pattern of the maxillary sinus.
In the neonate, the largest sinus is represented by a small cavity whose lower border lies above that of the nasal floor and is encroached upon by the upper dentition. However, as the development of the mid-third of the face progresses and eruption of the permanent dentition occurs, the floor of the sinus migrates to a lower level than that of the nasal cavity (0.5–10 mm).15
Ethmoid Sinus Development
The earliest signs of development of the ethmoid sinus are seen during the fourth fetal month.1–3 The ethmoid sinus has a multicentric origin. A great majority of the cells begin at the middle meatus as anterior ethmoid cells, and a minority develop from the superior and supreme meatus as posterior ethmoid cells. The anterior ethmoid cells appear as evaginations in the lateral nasal wall of the middle meatus. Somewhat later, the posterior cells evaginate the nasal mucosa in the superior meatus. All of these cells enlarge gradually throughout fetal life.
Other primitive structures called ethmoturbinals (middle, superior, and supreme), the uncinate process, the agger nasi, and the ethmoid bulla are medial extensions of the lateral wall of the nasal capsule. The attachments of these structures to the lateral nasal wall of the nasal capsule are the lamellae. There exist five lamellae with the following nomenclature (Table 1–2): first basal lamella (lateral extension of the uncinate process), second basal lamella (lateral extension of the ethmoid bulla), third basal lamella (attachment of the middle turbinate), fourth basal lamella (attachment of the superior turbinate), and fifth basal lamella (attachment of the supreme turbinate) when present (Fig. 1–7). The sinus cells during their development may stretch the lamellae but do not break through them, thereby retaining the integrity of each of the compartments.
First basal lamella | Lateral extension of uncinate process |
Second basal lamella | Lateral extension of ethmoid bulla |
Third basal lamella | Attachment of middle turbinate |
Fourth basal lamella | Attachment of superior turbinate |
Fifth basal lamella | Attachment of supreme turbinate (when present) |
During primary pneumatization, the rudiments of the ethmoid sinus consist of dimple-like depressions of the nasal mucosa into the nasal capsule. These depressions may originate from any of the mucosal furrows in the middle meatus or along the mucosa of the superior meatus, which is, itself, no more than a furrow at this time. The depressions gradually deepen and become globular air cells. As development progresses and these cells reach maximum growth and encroach on adjacent bony cells, they become flattened.
The ethmoid sinus is well developed at birth. During the second year after birth the air cells may grow beyond the confines of the ethmoid bone into the surrounding bones: maxilla, frontal, lacrimal, and sphenoid. The growth pattern of the ethmoid sinus is completely unpredictable, and development will continue until the ethmoid has reached almost adult size by the age of 12 years. Some further enlargements may take place in early adulthood.
The ethmoid sinus cells are divided into anterior and posterior groups based on their initial sites of pneumatization and the subsequent locations of their ostia (Fig. 1–8). Ethmoid cells may be further characterized on the basis of the skeletal structures they pneumatize. Thus, it is possible to define groups of cells as remaining within the ethmoid and others as lying beyond the ethmoid.
Ethmoid cells that belong to the ethmoid bone include the conchal, bullar, infundibular, and frontal recess cells. Among those that extend beyond the ethmoid bone are the agger nasi cells (anterior ethmoid cells that pneumatize the agger nasi on the medial surface of the frontal process of the maxilla and lacrimal bone), frontal sinus cells (anterior ethmoid cells that pneumatize the frontal bone), orbital cells (anterior ethmoid cells that pneumatize the orbital roof), and palatine bone and sphenoid bone cells (posterior ethmoid cells that pneumatize these bones).
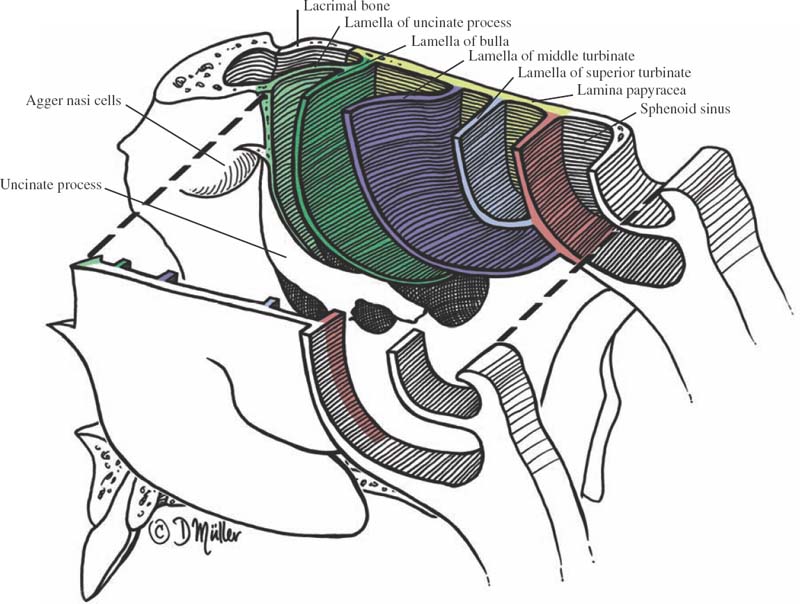
FIGURE 1–7 Relationship of the different lamellae.
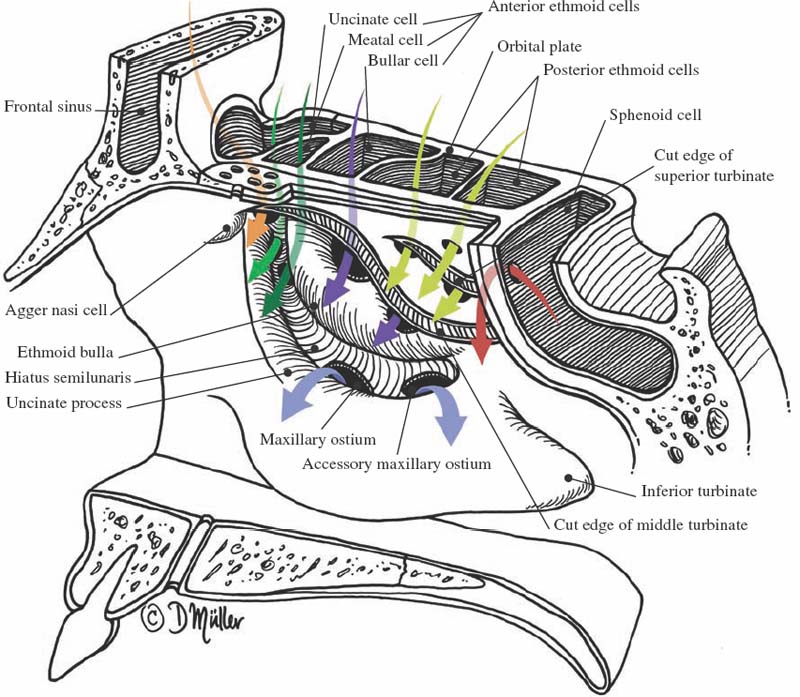
FIGURE 1–8 Bony anatomy of the various drainage systems of the paranasal sinuses.
The ethmoid sinus is responsible for cellular colonization into the surrounding structures: anteriorly, the agger nasi; superiorly, the frontal sinus; posteriorly, the sphenoid sinus; inferiorly, the uncinate process; laterally, the orbital bony structures; and medially, the medial surface of the middle turbinate to produce a middle turbinate concha bullosa. This haphazard growth makes the ethmoid sinus different from one individual to another. The cells that are located within the ethmoid bone are termed intramural cells, whereas those whose development involves an adjacent bone such as the maxilla, lacrimal bone, frontal bone, or sphenoid bone are called extramural cells (Fig. 1–9). Regardless of their origins, the sinuses are named for the bone in which they finally reside. For example, the frontal sinus is, in reality, often formed by displaced anterior ethmoid cells.
In the superior meatus there is a ridge in the lateral wall that is similar to the uncinate process. An accessory swelling is also seen there that resembles the ethmoid bulla of the middle meatus. A variety of structures of the superior nasal meatus are reminiscent of those that develop more completely in the middle meatus. The superior meatus is the origin of most of the posterior ethmoid air cells. These cells may also grow laterally into the junction of the nasal capsule and orbit posterior to the maxillary sinus cleft. Expansion of these cells into the posterior, lateral, and superior aspect of the maxilla is the usual origin of the ethmomaxillary cells (Haller’s cells).9,10,12 These cells may be small or even of significant size, and those of maximum development may give the appearance of an accessory maxillary sinus (Fig. 1–10).
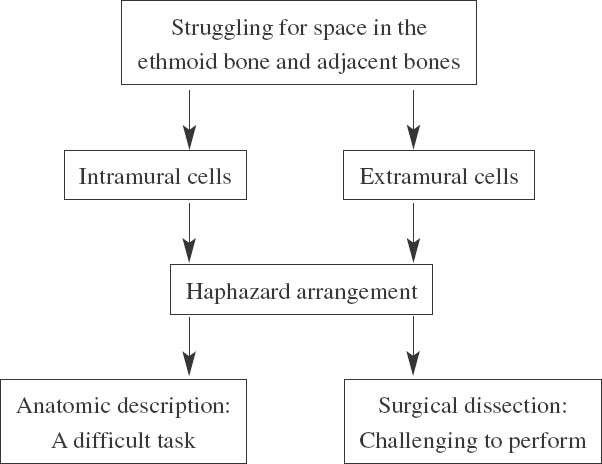
FIGURE 1–9 Ethmoid Sinus Development
Frontal Sinus Development
The frontal sinus begins to develop during the fourth fetal month, after the development of the frontal recess. Initially, this recess is a pocket found medial to the very cephalic or superior aspect of the uncinate process and expands into the thick nasal capsule mesenchyme. The fetal frontal recess is found between the uncinate process and the anterior attachment of the middle turbinate. There are two or four furrows or pits within the frontal recess that can potentially form air cells.
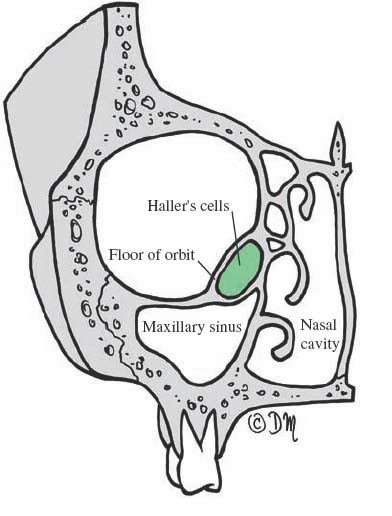
FIGURE 1–10 Haller’s cells.
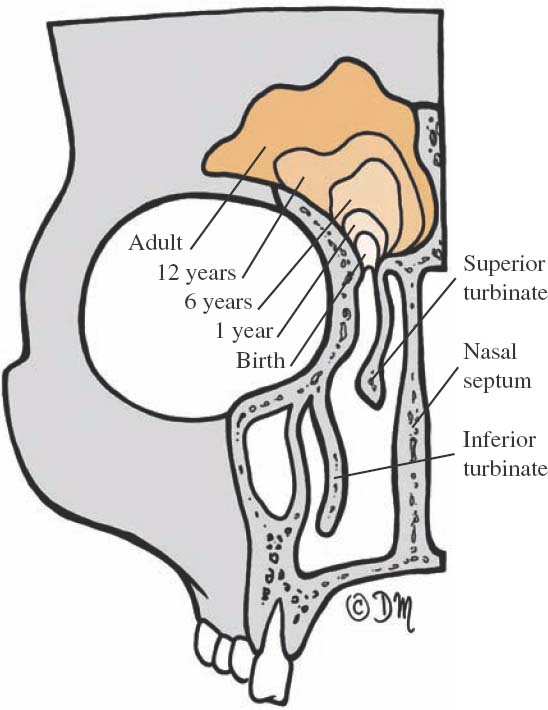
FIGURE 1–11 Developmental pattern of the frontal sinus.
The frontal sinus is described as developing in several ways:
1. by direct extension of the whole frontal recess
2. from the laterally placed anterior ethmoid cells within the frontal recess
3. from the ethmoid infundibular cells
4. from one or more of the anterior group of ethmoid cells arising in the frontal furrows
The great variation in the development of the frontal sinus accounts for the changes found in its drainage systems and for the presence or absence of a true frontonasal duct, the existence of which is the subject of some controversy.
The frontal sinus can therefore be formed by a direct extension of the whole frontal recess into the frontal bone or from the extension of anterior ethmoid cells within the frontal recess. A frontal sinus that develops from the ethmoid infundibulum or the first or second frontal furrows may have its drainage pathway restricted into a nasofrontal duct. The growth of the surrounding anterior ethmoid cells may also encroach on the proximal part of the frontal sinus, compressing it into a nasofrontal duct.3,14 The diameter of this duct depends largely on the degree of encroachment by the surrounding ethmoid cells. This usually does not affect the frontal sinus, which develops directly from the wall of the frontal recess and has a distinct ostium named the primary frontal sinus ostium (the point of origin of the frontal sinus). Prenatally, the frontal sinus does not expand much further.
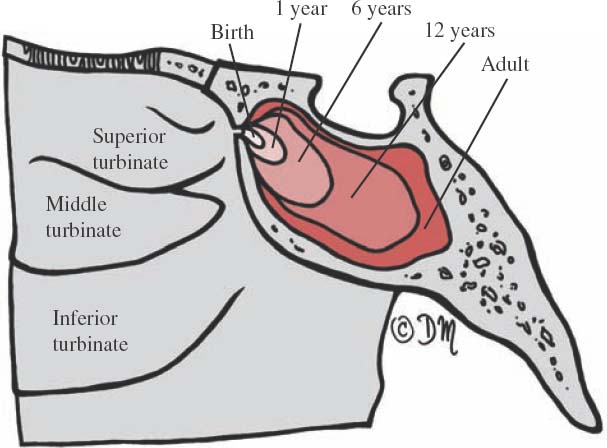
FIGURE 1–12 Developmental pattern of the sphenoid sinus.
Secondary pneumatization occurs postnatally, generally beginning between the ages of 6 months and 2 years. Initially, the secondary pneumatization occurs laterally toward the orbital side of the frontal bone, but during the second year of life pneumatization has a more vertical direction. However, by definition, a frontal sinus is not present until the cell enters the vertical (ascending) portion of the frontal bone. During its development, the superior extremity of the frontal sinus reaches the midvertical height of the orbit at 4 years of age and the level of superior orbital rim at 8 years. It grows into the frontal squama at 10 years of age. The frontal sinus continues its growth at a slow rate into adolescence, when it may reach its final size (Fig. 1–11). The expansion into the vertical frontal bone occurs closer to the cranial cavity, and consequently the external table of the frontal bone is thicker than the inner table.
The development of the frontal sinus may be affected by the expansion of the surrounding anterior ethmoid cells. In this situation, one or more of these cells begin pneumatizing the frontal bone and may even exceed the primary frontal sinus outgrowth. The “true” sinus that is first present in such a case may encroach on the lumen of the second sinus by forming a bulbous projection (bulla frontalis) in the wall of the latter larger sinus. In these cases, a thin plate of bone separates the two sinuses.
The left and the right frontal sinuses develop independently, and asymmetry between the frontal sinus is more the rule than the exception, in contrast to the case with the maxillary sinus. Pneumatization may also extend as far laterally as the temporal bone, but this is unusual.
Sphenoid Sinus Development
The development of the sphenoid sinus is unique because of two factors: (1) It is the only sinus that does not arise as an outpouching from the lateral nasal wall and (2) there is no primary pneumatization, but rather a constriction of the developing presphenoid recess followed by secondary pneumatization.
During the third month of fetal development the nasal mucosa invaginates into the posterior portion of the cartilaginous nasal capsule. This primordium is only a small presphenoid recess within the posterior end of the cartilaginous nasal capsule. By the end of the third and early fourth fetal months the posterosuperior portion of the recess is separated incompletely from the nasal cavity by the development of a nasal mucosal fold, inferiorly based, curving upward and anterior to the body of the presphenoid. As the nasal capsule undergoes chondrification, a cartilaginous concha forms within this fold, developing cartilaginous concavities, which, by the fifth fetal month, enclose the presphenoid recess. This site of initial sinus rudiment and of initial constriction is preserved in adulthood as the location of the sinus ostium. The wall surrounding this cartilage is ossified in the later months of fetal development.
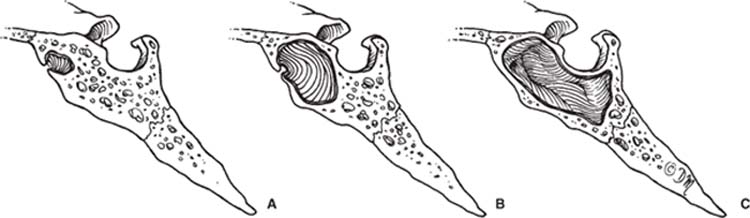
FIGURE 1–13 Anatomical variations of the sphenoid sinus pneumatization. (A) Conchal or fetal type. (B) Presellar or juvenile type. (C) Sellar or adult type.
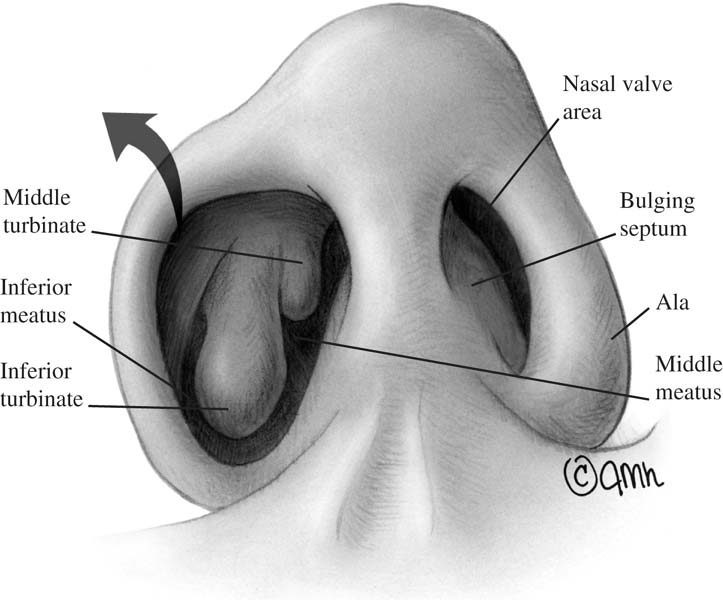
FIGURE 1–14 The nasal valve area. It is the area of peak restriction of nasal airflow.
At birth the sphenoid sinus is no more than an encircled recess, located between the sphenoid concha and the presphenoid body. After birth, the sphenoid sinus primordium grows inferiorly and posteriorly. In the second and third years the intervening cartilage is resorbed, and part of the sphenoid concha fuses to the presphenoid body; the resulting cavity clearly becomes the sphenoid sinus. The presphenoid recess becomes the sphenoethmoid recess. Following this fusion, pneumatization of the sphenoid occurs with expansion into the presphenoid and, later, the basisphenoid parts of sphenoid bone, with the sphenoid concha remaining as the anterior sinus wall. By the age of 8 to 10 years a real sinus cavity may be observed, although the definitive form of the sinus is attained at puberty (Fig. 1–12). The origin of the sphenoid sinus from the posterior nasal cavity is always identified by the sinus ostium (the location where the sphenoid recess retained its continuity with the nasal cavity), which is located high on the anterior sinus wall, just a few millimeters below the sphenoethmoid recess.
The shape of the sinus is determined by the varying degrees of pneumatization that take place in the secondary pneumatization. The sphenoid sinus may pneumatize beyond the confines of the sphenoid body to the greater or lesser wings, the medial and lateral pterygoid plates, the palatine and basioccipital bones, or the ethmoid bone. The lateral expansion brings the sphenoid into contact with the second and third divisions of the trigeminal nerve as well as the nerve of the pterygoid canal (vidian nerve).
The sphenoid sinus may be classified according to its degree of pneumatization: (1) conchal or fetal-type sinus with minimal extension, which is relatively rare (2%); (2) presellar or juvenile-type sinus, expanding posteriorly to the anterior sellar wall, which occurs in ~10 to 24% of the adult population; and (3) sellar or adult-type sinus, extending below the sella or farther, which may be found in as many as 86% of all adults (Fig. 1–13).3,10,14,16
 Macroscopic Anatomy
Macroscopic Anatomy
Nasal Cavity
The internal nose is constituted by two nasal cavities extending from the nares to the choanae and separated by the nasal septum. The nasal cavity is roughly a right triangle in outline, slightly wider toward its central position. The nares lead into the vestibule, the skin-lined part of the nasal cavity that contains the vibrissae (nasal hairs), the hair follicles, and the sebaceous glands.
The vestibule is limited above and behind by a curved ridge, the limen nasi. A recess of the vestibule reaches upward into the tip. The junction of the nasal skin and the mucous membrane of the nasal cavity occurs at a variable distance inside the nose, but it is clearly defined visually by the difference in color between skin and mucosa. The union of the skin-lined nasal vestibule with the mucosa-lined chamber of the nasal cavity has the shape of a triangular aperture, and it constitutes the narrowest area of the normal nasal airway called the nasal valve (Fig. 1–14). Its superior and lateral limits are formed by the upper lateral cartilage; its medial wall is represented by the nasal septum; and its base, by the floor of the nose. The nasal valve area marks the junction between the lower limit of the upper lateral cartilage and the upper portion of medial and lateral crura of the lower lateral cartilages.17–22
The mucosa of the nasal cavity has a pseudostratified ciliated columnar epithelium and communicates with the adjoining paranasal sinus and with the nasopharynx via the posterior choana. The nasal cavity has a roof, a floor, a medial wall, and a lateral nasal wall.23–27
ROOF
The upper zone of the nasal cavity is named the olfactory cleft. It is divided into a nasal part lying anteriorly, an ethmoid area centrally, and a sphenoid part posteriorly. The sloping anterior portion of the roof of the nasal cavity is formed by the nasal bones and the nasal spine of the frontal bone. The central segment of the roof is mainly defined by the cribriform plate of the ethmoid bone and is often referred to as the olfactory area. The descending posterior part of the roof of the nasal cavity is constituted by the anterior wall of the sphenoid sinus. The sphenoethmoid recess lies in this posterior segment. The junction between the vertical anterior wall and the horizontal floor of the sphenoidal sinus marks the end of the nasal cavity and forms the boundary of the choana.
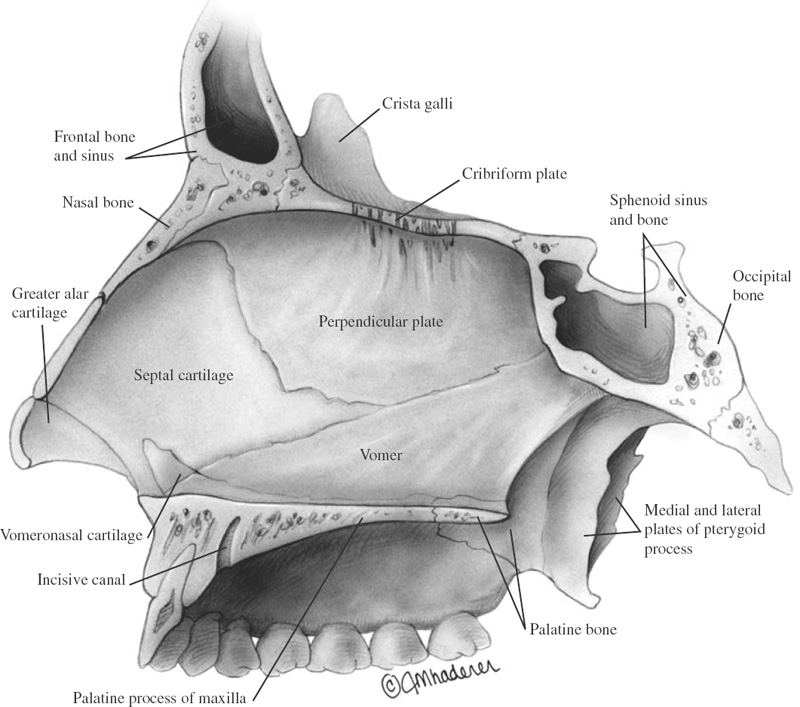
FIGURE 1–15 Nasal septum.
FLOOR
The bony floor of the nasal cavity is formed by the premaxilla, the maxilla, and the horizontal plate of the palatine bone in the posterior portion. The floor is ~4.5 cm long and continues posteriorly into the soft palate. It extends laterally into the inferior meatus and medially to the nasal septum.
MEDIAL WALL
The medial wall of the nasal cavity is represented by the septum, which is composed of cartilaginous and bony segments (Fig. 1–15). The cartilaginous segment consists of the quadrilateral cartilage, with a contribution from the lower and upper cartilages. The upper margin of the septal cartilage is connected to the posterior border of the internasal suture and to the upper lateral cartilages. Anteriorly, this cartilage is related to the medial crura of the lower lateral cartilages at its superior level, and inferiorly, it rests on the anterior nasal spine. This spine is an extension of the maxillary crest, and it is positioned like the prow of a sailing ship. Also, inferiorly the quadrilateral cartilage sits in the groove of the maxillary crest. The bony elevation on the floor of the nose on which the entire cartilaginous septum sits is shaped much like the lines of a railroad track. The bony segment of the nasal septum includes the perpendicular plate of the ethmoid bone and the vomer. The perpendicular plate forms the upper and anterior part of the bony septum and is continuous above with the cribriform plate. The vomer is located below and behind the perpendicular plate of the ethmoid bone. The long anterior border of the vomer articulates with the perpendicular plate superiorly and with the quadrilateral cartilage inferiorly. The inferior border is related to the nasal crest formed by the maxillae and the palatine bones.
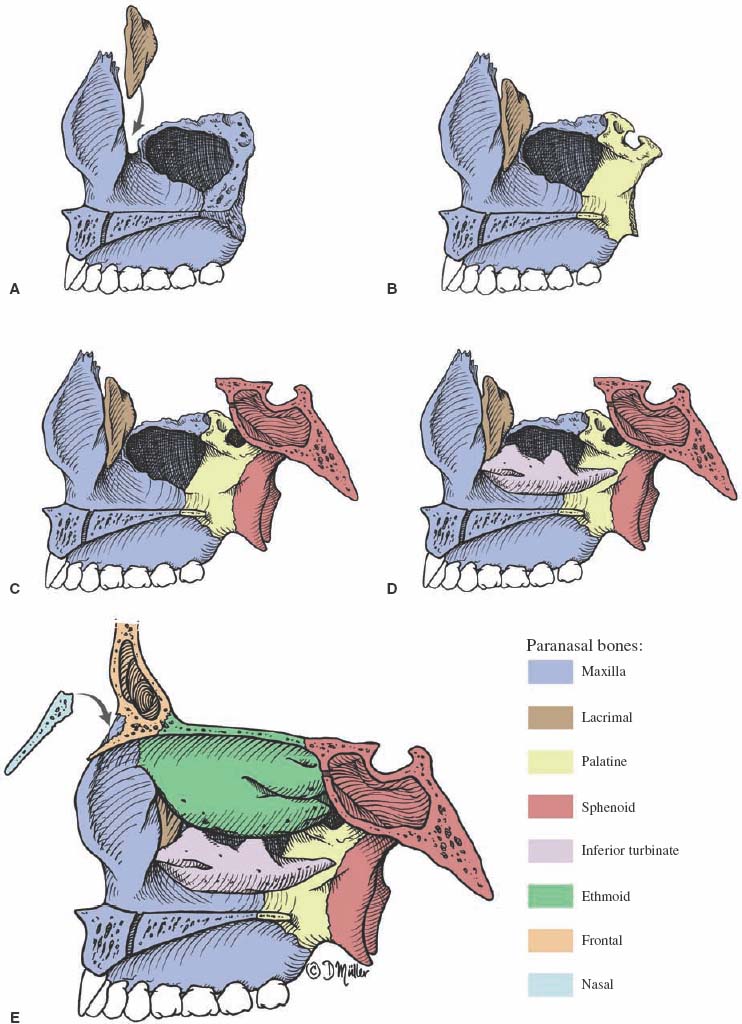
FIGURE 1–16 Osteology of the right lateral nasal wall (medial view). (A) Articulation of the maxilla with the lacrimal bone. (B) Articulation of the maxilla with the palatine bone. (C) Articulation of the maxilla with the sphenoid bone. (D) Articulation of the maxilla with the inferior turbinate. (E) Articulation of the maxilla with the ethmoid labyrinth and nasal bone.
LATERAL NASAL WALL
The lateral nasal wall is a very complex anatomical structure and a very important area clinically. The lateral wall of the nasal cavity can be divided into three areas: Anteriorly, the lateral nasal wall consists of the frontal process of the maxilla and the lacrimal bone; the middle area is formed by the ethmoid labyrinth, the maxilla, and the inferior turbinate; and the posterior portion of the lateral nasal wall is represented by the perpendicular plate of the palatine bone and the medial pterygoid plate of the sphenoid bone. The osteology of the lateral nasal wall is complex and represented by eight bones, which are articulated in such a way as to build up a firm bony structure (Fig. 1–16).
The most important features of the lateral wall of the nasal cavity are the turbinates (Fig. 1–17). There are usually three (or rarely four), and they appear as delicate shelflike bony structures protruding from the lateral nasal wall covered by ciliated columnar mucous epithelium. The superior, middle, and inferior turbinates are present in almost all individuals, and a very small supreme turbinate may also occur. The supreme, superior, and middle turbinates are included in the ethmoid bone. The inferior turbinate is an independent bone. The air spaces below and lateral to the turbinates are named the superior, middle, and inferior meatus, respectively. They communicate with the common nasal cavity at the lower edge of each meatus (Fig. 1–18).
The inferior surfaces of the free-hanging portions of the turbinates are almost parallel to the nasal floor, but their supporting attachments usually are oriented diagonally from posterior-inferior to anterior-superior. Each supporting portion is called a primary lamella. There are five lamellae located from anterior to posterior: the uncinate process, the ethmoid bulla, the basal lamella of the middle turbinate, the basal lamella of the superior turbinate, and the fifth lamella of the supreme turbinates when present (Fig. 1–7). The superior and supreme turbinate lamellae are relatively horizontal.
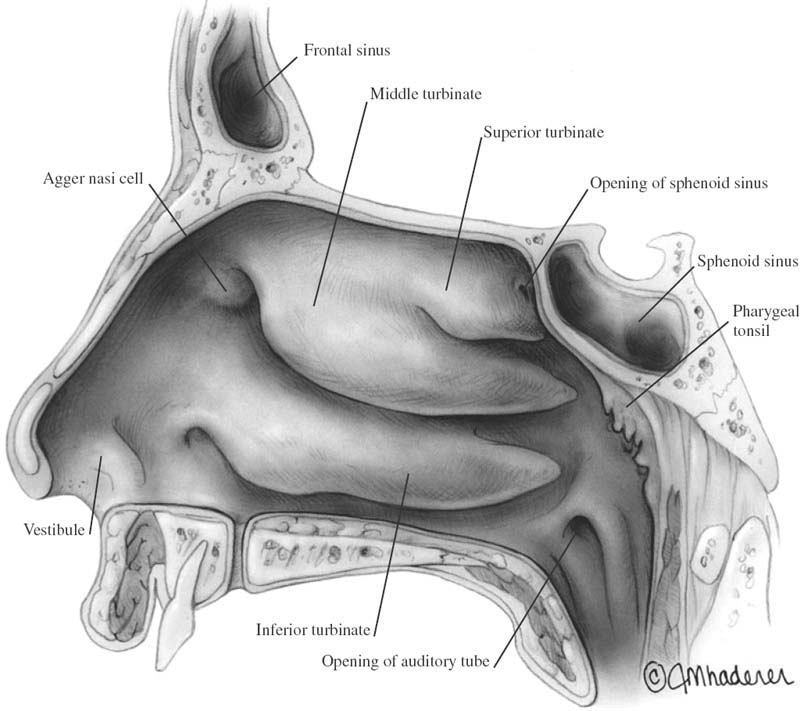
FIGURE 1–17 Lateral nasal wall.
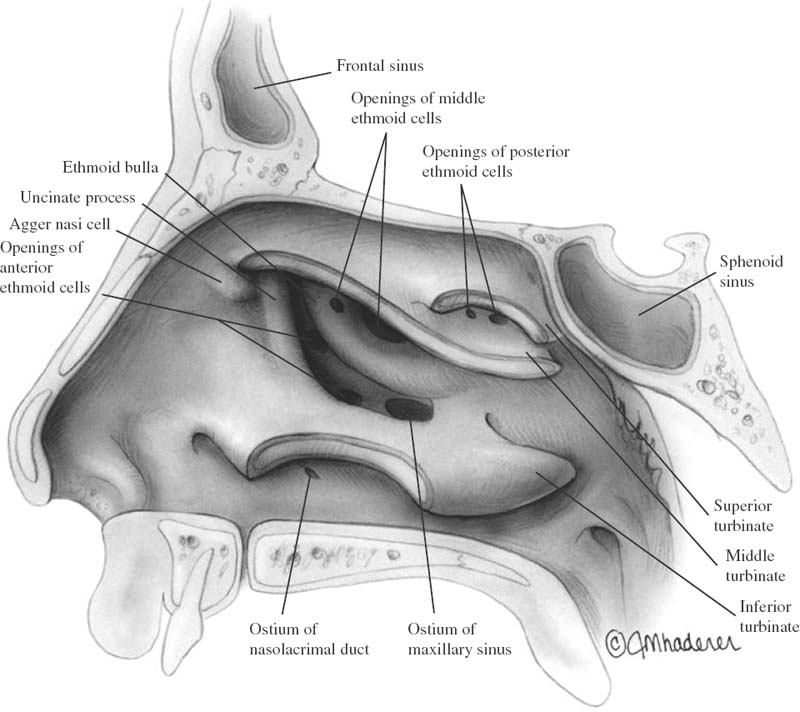
FIGURE 1–18 The turbinates are cut, and the meatus area is exposed.
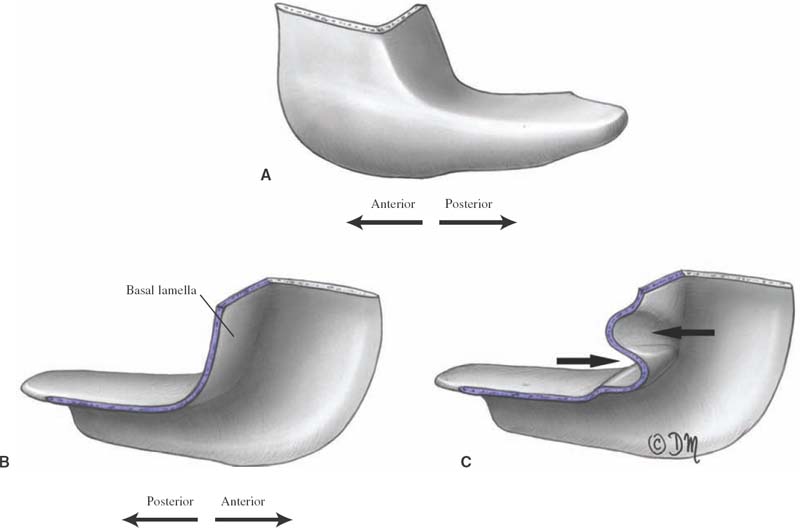
FIGURE 1–19 Anatomical configuration of the basal lamella of the right middle turbinate. (A) Medial view. (B) Lateral view. (C) Lateral view with distortion of the basal lamella by the ethmoid cells.
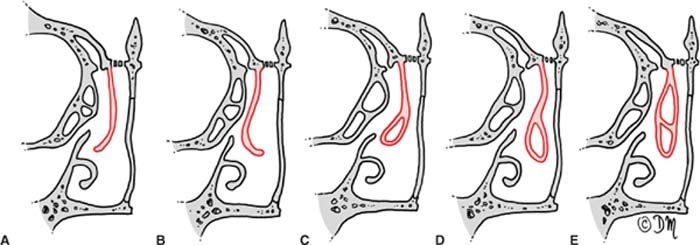
FIGURE 1–20 Anatomical variations of the middle turbinate. (A) Normal. (B) Paradoxical turbinate. (C) Normal turbinate with partial pneumatization. (D) Paradoxical turbinate with partial pneumatization. (E) Concha bullosa.
The superior turbinate belongs to the ethmoid bone, and it measures ~1.5 cm in length. The superior turbinate is attached to the lamina papyracea of the ethmoid bone by a thin bony partition. It is usually pneumatized, and it forms part of the posterior ethmoidal cells. The superior meatus lies between the middle and superior turbinates and contains the ostia of the posterior ethmoidal cells. Immediately behind the superior meatus is situated the sphenopalatine foramen. A small ridge, the supreme turbinate, is sometimes visible above the superior turbinate. If a supreme turbinate is present, a fifth basal lamella arises from it and extends laterally.
The middle turbinate is a portion of the ethmoid bone and is ~4 cm in length. The anterior end of the middle turbinate inserts into the ascending process of the maxilla and the posteromedial edge of the agger nasi. The superior attachment is in the paramedian sagittal plane and adheres to the lateral edge of the perforated portion of the cribriform plate along the ethmoid roof to a more vertical orientation along the lamina papyracea of the ethmoid bone. This twisting attachment of the middle turbinate bends within the middle third of the basal lamella, resulting in a prominent anterior vertical portion and a posterior descending horizontal plate (Fig. 1–19). The posterior portion of the insertion of the middle turbinate runs in a horizontal plane forming the roof of the posterior middle meatus. This posterior end is attached to the ethmoid crest of the perpendicular plate of the palatine bone. Pneumatization of the middle turbinate is frequent at its anterior end and in the main body mass. The pneumatized middle turbinate (also known as concha bullosa) is present in one-third of the population (Fig. 1–20). The middle turbinate is composed of a conchal bone, mucoperiosteum, a submucosal cavernous plexus, and respiratory mucous membrane.
The middle meatus lies between the middle and inferior turbinate attachments. The lateral wall of the middle meatus is the most important area of the lateral wall of the nasal cavity, as many of the paranasal sinuses open here. It houses several key anatomical structures: the uncinate process, the hiatus semilunaris, the ethmoid infundibulum, the ethmoid bulla, the lateral sinus, and the frontal recess. The term ostiomeatal complex is used to describe a group of anatomical structures belonging to the nasal lateral wall that are contributing to the final common drainage pathways of the anterior ethmoid, maxillary, and frontal sinuses. The ostiomeatal complex includes the middle meatus, the uncinate process, the hiatus semilunaris, the ethmoid infundibulum, the ethmoid bulla, the maxillary sinus ostia, and the frontal recess (Fig. 1–21).
Uncinate Process
The uncinate process (from the Latin uncinatus, meaning “hooked”) is a thin, sagittally oriented lamella that runs anterosuperiorly to posteroinferiorly from the roof of the ethmoid bone to the perpendicular plate of the palatine bone and to the ethmoid process of the inferior turbinate. Three to five bony spicules unite the inferior convex border with similar structures of the ethmoid process of the inferior turbinate. The posterior end of the uncinate process curves laterally upward toward the roof of the maxillary sinus and may be continuous with the perpendicular plate of the palatine bone, or a complete bony absence may occur. This bony absence allows the mucosa of the maxillary sinus to contact the mucosa of the lateral nasal wall. This area is called the posterior fontanelle. A similar dehiscence in the uncinate process at its articulation with the inferior turbinate is termed the anterior fontanelle, and it is located anterior to the natural ostium of the maxillary sinus. Perforation of these membranes leads to openings of accessory ostia of the maxillary sinus. The upper portion of the uncinate process is hidden by the insertion of the middle turbinate, and it runs a variable course (Fig. 1–22). It may attach to the roof of the ethmoid bone, or it may also turn medially and fuse with the middle turbinate. When the uncinate process inserts laterally on the lamina papyracea, the ethmoid infundibulum is closed superiorly by a blind pouch named the recessus terminalis. In this situation, the ethmoid infundibulum and the frontal recess are separated from each other, and so the frontal sinus drains into the middle meatus medial to the infundibulum (Type I). When the uncinate process is inserted into the middle turbinate, the frontal recess and, consequently, the frontal sinus open directly into the ethmoid infundibulum (Type II) (Fig. 1–23).
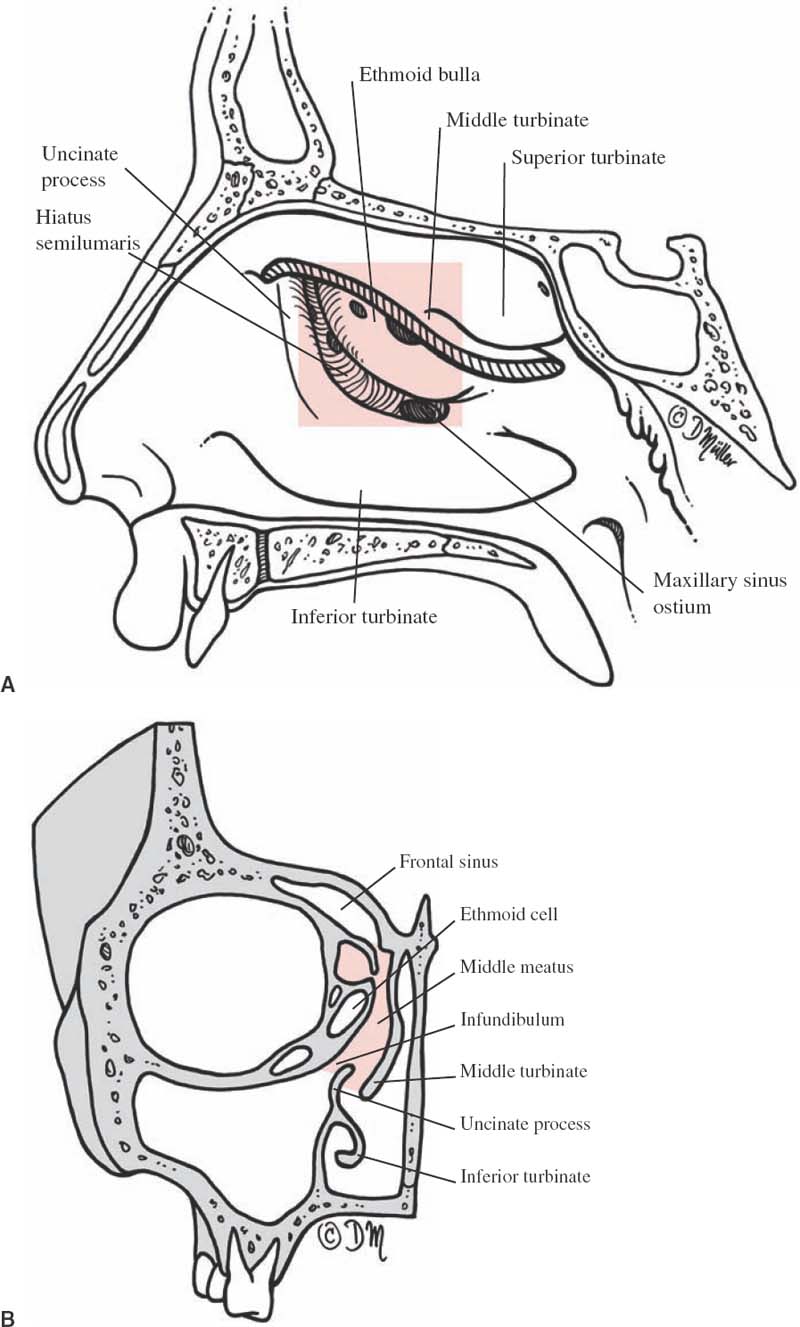
FIGURE 1–21 The ostiomeatal complex is illustrated after removing the middle turbinate (cut edge shaded). It includes the middle meatus, the uncinate process, the hiatus semilunaris, the ethmoid infundibulum, the ethmoid bulla, the maxillary sinus ostia, and the frontal recess. (A) Lateral view after removing the middle turbinate. (B) Coronal section.
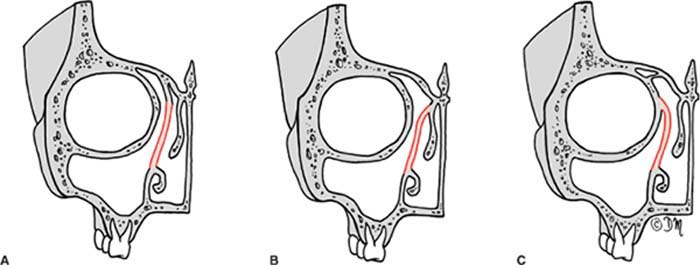
FIGURE 1–22 Anatomical variations of the uncinate process. Its superior portion may attach to the roof of the ethmoid bone centrally (A), to the middle turbinate medially (B), or to the lamina papyracea laterally (C).
The uncinate process may itself become pneumatized and provoke narrowing of the ethmoid infundibulum. Also, it can expand anteriorly and develop into infundibular cells. These cells may extend anteriorly and superiorly as far as the lacrimal bone, thereby creating the ethmolacrimal cells. The uncinate process can occasionally be absent and be replaced by a fibrous band.
Hiatus Semilunaris
The hiatus semilunaris is the two-dimensional space between the posterior edge of the uncinate process and the anterior wall of the ethmoid bulla. The hiatus semilunaris is usually hidden by the overhanging middle turbinate. It measures ~1.5 to 2 cm in length and runs from its inferior end in an anterosuperior direction. The hiatus semilunaris forms the doorway that leads to a lateral space called the ethmoid infundibulum.
Ethmoid Infundibulum
The ethmoid infundibulum is the three-dimensional space bounded by the uncinate process medially, the ethmoid bulla posteriorly, and the lamina papyracea laterally. The entire length of the ethmoid infundibulum may reach 4 cm, depending on the shape of the uncinate process. The ethmoid infundibulum can be entered through the hiatus semilunaris. The anterior end may extend to the posterior surface of the agger nasi cells or, in some cases, to the ascending process of the maxilla. The infundibular space is wider anterosuperiorly and narrower at its more posterior end because of the union of the uncinate process with the inferior turbinate and the membranous anterior fontanelle. The greatest width (free margin of the uncinate process to the lamina papyracea) is 5 to 6 mm, but in some cases it can be very shallow because the uncinate process runs close to the lamina papyracea (~1–1.5 mm away). The ethmoid infundibulum may be almost atelectatic according to anatomical variations of other structures such as paradoxical bending of the middle turbinate, a concha bullosa, or a hypoplastic maxillary sinus. In the most extreme conditions it may disappear if pathologic lesions compress the uncinate process laterally against the lamina papyracea.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


